You might also like
- DSM 5 Vs DSM 4 Case StudiesDocument18 pagesDSM 5 Vs DSM 4 Case Studiesapi-261267976100% (1)
- Learning A More Beneficial Way of CommunicationDocument4 pagesLearning A More Beneficial Way of CommunicationGoing ApeSNo ratings yet
- Case 3Document21 pagesCase 3Mustabeen TairNo ratings yet
- Neem by Ellen NortenDocument100 pagesNeem by Ellen NortenMano DrabuzeliaiNo ratings yet
- Psychological Report of SR - DeseoDocument3 pagesPsychological Report of SR - DeseoRommel SarjNo ratings yet
- BlsDocument62 pagesBlspaediatrica89% (19)
- Trauma Disorders Chapter IntroductionDocument25 pagesTrauma Disorders Chapter IntroductionIzzyinOzzieNo ratings yet
- Lifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsDocument7 pagesLifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsArcelino Farias100% (1)
- WorksheetsDocument181 pagesWorksheetscatamedellin2011No ratings yet
- Resisted ExerciseDocument29 pagesResisted ExerciseVaraNo ratings yet
- Learned Optimism ExplainedDocument8 pagesLearned Optimism ExplainedAnonymous u80JzlozSDNo ratings yet
- (Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioDocument455 pages(Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioEsteban Gonzàlez RodriguezNo ratings yet
- Case No 2 SchizoDocument8 pagesCase No 2 SchizoSarah Saqib AhmadNo ratings yet
- Review QuestionsDocument5 pagesReview Questionsjmkap13No ratings yet
- A Psychiatric CaseDocument11 pagesA Psychiatric CaseGokul PoudelNo ratings yet
- Internship - Clinical PsychDocument18 pagesInternship - Clinical PsychNEELAMNo ratings yet
- Major Depression Case 2Document14 pagesMajor Depression Case 2Mahnoor Malik100% (1)
- Nelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorDocument312 pagesNelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorFaisal MomenNo ratings yet
- AOTA Statement On Role of OT in NICUDocument9 pagesAOTA Statement On Role of OT in NICUMapi RuizNo ratings yet
- Understanding Oppositional-Defiant Disorder: What Is It?Document8 pagesUnderstanding Oppositional-Defiant Disorder: What Is It?Abhilash PaulNo ratings yet
- Narcissistic Personality Disorder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNarcissistic Personality Disorder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 3.5 out of 5 stars3.5/5 (2)
- Paranoid Personality Disorder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandParanoid Personality Disorder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- A Case Study of A Patient Suffering From Major Depressive DisorderDocument5 pagesA Case Study of A Patient Suffering From Major Depressive Disorderdennis ndegeNo ratings yet
- Ent Solved Kmu Seqs by RMC StudentsDocument68 pagesEnt Solved Kmu Seqs by RMC StudentsAamir Khan100% (1)
- Psychology 201 Exam 2Document6 pagesPsychology 201 Exam 2chang seoNo ratings yet
- Colorectal Cancer: Symptoms, Staging and ScreeningDocument65 pagesColorectal Cancer: Symptoms, Staging and ScreeningMuhammed Muzzammil Sangani50% (2)
- Depression PresentationDocument39 pagesDepression Presentationapi-290668891No ratings yet
- Case Study-1 Personality Psychology About This Assignment: Questions For DiscussionDocument6 pagesCase Study-1 Personality Psychology About This Assignment: Questions For DiscussionLakshmi NarayanaNo ratings yet
- CasesDocument9 pagesCasesAdeel AizadNo ratings yet
- Psychological DisordersDocument7 pagesPsychological Disorderskuro hanabusaNo ratings yet
- Tat ReportDocument14 pagesTat Reportmarriumemaan582No ratings yet
- Class 11 Case Studies (By Myself)Document7 pagesClass 11 Case Studies (By Myself)AnushkaGuptaNo ratings yet
- CasestudyDocument6 pagesCasestudyapi-297258832No ratings yet
- Psychological Disorders Case StudiesDocument7 pagesPsychological Disorders Case StudiesLauren OwenNo ratings yet
- Unit-1 Abn PsychDocument33 pagesUnit-1 Abn PsychNiyamath NazeerNo ratings yet
- Item AnalysisDocument15 pagesItem AnalysisKiann BuenavistaNo ratings yet
- Manali Vaze Case File Final PDFDocument11 pagesManali Vaze Case File Final PDFKinjal SanghviNo ratings yet
- SIK-SJA-035 (RamiaAlH-6024)Document11 pagesSIK-SJA-035 (RamiaAlH-6024)zawar mughalNo ratings yet
- Case Study AnalysisDocument4 pagesCase Study Analysisapi-656182395No ratings yet
- The Challenges of Middle and Late AdolescenceDocument50 pagesThe Challenges of Middle and Late AdolescenceChona BontigaoNo ratings yet
- Assessment ReportDocument6 pagesAssessment ReportHira KianiNo ratings yet
- Assessment Report HiraDocument6 pagesAssessment Report HiraHira KianiNo ratings yet
- Psychology Case StudyDocument12 pagesPsychology Case StudyVratti AgrawalNo ratings yet
- Csa Case Enuresis 2017Document5 pagesCsa Case Enuresis 2017Ahmed YoosufNo ratings yet
- Pizzo RDocument7 pagesPizzo Rapi-601562832No ratings yet
- Abpsych Intervention QuestionsDocument6 pagesAbpsych Intervention QuestionsAndrew NavarraNo ratings yet
- Case Profile PsycologyDocument11 pagesCase Profile Psycologycrazy adwaithNo ratings yet
- Psychopathology of ChildhoodDocument64 pagesPsychopathology of ChildhoodFakher KhaliliNo ratings yet
- Psychology DepressionDocument13 pagesPsychology DepressionDhanashriNo ratings yet
- Dwnload Full Abnormal Psychology An Integrative Approach 5th Edition Barlow Test Bank PDFDocument35 pagesDwnload Full Abnormal Psychology An Integrative Approach 5th Edition Barlow Test Bank PDFdrakeducuvzeve100% (17)
- Case Presentation-WilliamDocument4 pagesCase Presentation-Williamapi-220984641100% (2)
- Running Head: INTERVIEW PROFILE 1Document7 pagesRunning Head: INTERVIEW PROFILE 1mgw777No ratings yet
- OCD Case Report: "Obsessive Thoughts and RitualsDocument19 pagesOCD Case Report: "Obsessive Thoughts and Ritualsmirha fatimaNo ratings yet
- Mental Health Lesson on Identity, Grief, Anxiety, OCD, Schizophrenia, and Eating DisordersDocument2 pagesMental Health Lesson on Identity, Grief, Anxiety, OCD, Schizophrenia, and Eating DisordersKaya S75% (4)
- 04-04 SpenceDocument2 pages04-04 SpenceKaya SNo ratings yet
- Look Inside Triumph Over ShynessDocument13 pagesLook Inside Triumph Over ShynessPrabhu RamachandranNo ratings yet
- Baum StressDocument33 pagesBaum Stresslaki lakiNo ratings yet
- PM 05 18Document22 pagesPM 05 18Hira KhanNo ratings yet
- Child ProtocolDocument4 pagesChild Protocolcecilm_1No ratings yet
- 7 PTSD MS 4THDocument8 pages7 PTSD MS 4THNamra QaisNo ratings yet
- Grade 8 Health Q1Document21 pagesGrade 8 Health Q1Jayhia Malaga JarlegaNo ratings yet
- Psychodiagnostic Assessment Report for 21-Year Old Female StudentDocument5 pagesPsychodiagnostic Assessment Report for 21-Year Old Female StudentMukarla DejavuNo ratings yet
- Case Study 2 3318Document4 pagesCase Study 2 3318Sarah NwosuNo ratings yet
- Case Study WordyDocument8 pagesCase Study Wordyapi-242082997No ratings yet
- Social Phobia PresentationDocument27 pagesSocial Phobia Presentationsuper_mugginsNo ratings yet
- What Is AbnormalDocument5 pagesWhat Is AbnormalRita1976No ratings yet
- Case Study 5Document10 pagesCase Study 5josmamani6789No ratings yet
- Hidly 2023 Product CatalogDocument37 pagesHidly 2023 Product CatalogHussain FirazNo ratings yet
- Rules SSC V19-20171Document41 pagesRules SSC V19-20171Hussain FirazNo ratings yet
- Women's Day Booklet - FINALDocument10 pagesWomen's Day Booklet - FINALHussain FirazNo ratings yet
- Building BridgesDocument3 pagesBuilding BridgesHussain FirazNo ratings yet
- OBG ChapterDocument3 pagesOBG ChapterMohd IrfanNo ratings yet
- Product SelectionDocument5 pagesProduct Selectionemmanuelgk100No ratings yet
- A Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreDocument11 pagesA Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreRamasamyNagarajan100% (1)
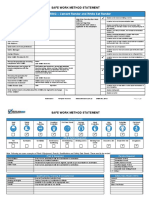
- 3075 SWMS RendererDocument13 pages3075 SWMS Renderernik KooNo ratings yet
- 1992 2007 Kpds Ilgisiz Cumle Sorulari Seyfihocacom - Pdf.pdfsifreDocument24 pages1992 2007 Kpds Ilgisiz Cumle Sorulari Seyfihocacom - Pdf.pdfsifreozgurekinsuNo ratings yet
- Amway ProductDocument9 pagesAmway ProductAbu Sayed Md. RashedNo ratings yet
- Grand Unification For World Peace Music THerapy For Integrating Healthcare PDFDocument339 pagesGrand Unification For World Peace Music THerapy For Integrating Healthcare PDFDr Suvarna NalapatNo ratings yet
- PDF Biaya MaternityDocument2 pagesPDF Biaya MaternityKurnia Yuliyanti RahayuNo ratings yet
- Penile Injection TherapyDocument4 pagesPenile Injection Therapydr NayanBharadwajNo ratings yet
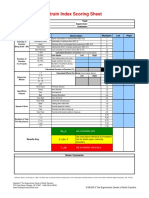
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- Connectors 2Document14 pagesConnectors 2Irene SánchezNo ratings yet
- Hospital Self Assement ToolkitDocument28 pagesHospital Self Assement ToolkitNidhi VijanNo ratings yet
- Kurukshetra University PhD Entrance Exam GuideDocument27 pagesKurukshetra University PhD Entrance Exam GuidemanojrkmNo ratings yet
- Plant Tissue Culture Media PDFDocument3 pagesPlant Tissue Culture Media PDFTitan Biotech100% (1)
- Central Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFDocument398 pagesCentral Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFRomeo-Remus RaffaiNo ratings yet
- Leopold Maneuvers Nursing ProcedureDocument3 pagesLeopold Maneuvers Nursing ProcedureDiane grace SorianoNo ratings yet
- Human Population and EnvironmentDocument4 pagesHuman Population and Environmentmonkeybike88No ratings yet
- Obamacare Ushers in New Era For The Healthcare IndustryDocument20 pagesObamacare Ushers in New Era For The Healthcare Industryvedran1980No ratings yet
- Week 15 - ONCO COURSE TASK - Breast Cancer DetectionDocument3 pagesWeek 15 - ONCO COURSE TASK - Breast Cancer DetectionGelo AlonzoNo ratings yet
- UG MaharashtraNationalLawUniversityMNLUMumbaiDocument5 pagesUG MaharashtraNationalLawUniversityMNLUMumbaiArpan KushwahaNo ratings yet