You might also like
- 2005-2010 Tacoma Bed Extender PT329-35050 Rev. A - PT329-35050Document8 pages2005-2010 Tacoma Bed Extender PT329-35050 Rev. A - PT329-35050kylemac123No ratings yet
- Review ATLS & Post TestDocument41 pagesReview ATLS & Post TestNugraha Arganda Ginting100% (2)
- My Heart Sings Praises - Line UpDocument4 pagesMy Heart Sings Praises - Line UpAnthony JimenezNo ratings yet
- Telemecanique Integral 32 Motor StarterDocument52 pagesTelemecanique Integral 32 Motor StarterJaime IxtaNo ratings yet
- Nej M Abbotts TentDocument11 pagesNej M Abbotts TentWKYC.comNo ratings yet
- An Analysis of Mechanisms of Post Stenotic DilatationDocument21 pagesAn Analysis of Mechanisms of Post Stenotic Dilatationhassenesalam18No ratings yet
- Pi Is 1522294218300734Document19 pagesPi Is 1522294218300734William MakdinataNo ratings yet
- 2022 - Anesthetic Management For Open Thoracoabdominal and Abdominal Aortic Aneurysm RepairDocument14 pages2022 - Anesthetic Management For Open Thoracoabdominal and Abdominal Aortic Aneurysm RepairLaura Camila RiveraNo ratings yet
- Clinical Anatomy - 2020 - Le Saint Grant - Arterial Anatomy of The Anterior Abdominal Wall Ultrasound Evaluation As ADocument6 pagesClinical Anatomy - 2020 - Le Saint Grant - Arterial Anatomy of The Anterior Abdominal Wall Ultrasound Evaluation As AarifNo ratings yet
- Blunt Traumatic Aortic Injury: Initial Experience With Endovascular RepairDocument6 pagesBlunt Traumatic Aortic Injury: Initial Experience With Endovascular RepairYahya AlmalkiNo ratings yet
- Resuscitativeendovascular Balloonocclusionofthe Aorta:: A Practical ReviewDocument18 pagesResuscitativeendovascular Balloonocclusionofthe Aorta:: A Practical ReviewJulian SanchezNo ratings yet
- Diamante de La Muerte 2020Document24 pagesDiamante de La Muerte 2020jonathan ruizNo ratings yet
- Embolization Hepatic TraumaDocument10 pagesEmbolization Hepatic TraumaФедір ПавукNo ratings yet
- Shock Hipo 2 FixDocument11 pagesShock Hipo 2 FixAdeliaNo ratings yet
- Open Surgical Repair of Abdominal Aortic Aneurysms Maintains A Pivotal Role in The Endovascular EraDocument10 pagesOpen Surgical Repair of Abdominal Aortic Aneurysms Maintains A Pivotal Role in The Endovascular EraAnna Sofía ParedesNo ratings yet
- 1 s2.0 S1053077022007510 MainDocument16 pages1 s2.0 S1053077022007510 MainCristhian BastidasNo ratings yet
- Dissertation Blood TransfusionDocument4 pagesDissertation Blood TransfusionAcademicPaperWritersTucson100% (1)
- PIIS0022522311007525Document10 pagesPIIS0022522311007525Enrico SquiccimarroNo ratings yet
- Histidine-Tryptophan-Ketoglutarate (HTK) Is Associated With Reduced Graft Survival in Pancreas TransplantationDocument5 pagesHistidine-Tryptophan-Ketoglutarate (HTK) Is Associated With Reduced Graft Survival in Pancreas TransplantationEduardo PalmaNo ratings yet
- Damage Control Surgery: A Staged Approach for Severely Injured PatientsDocument68 pagesDamage Control Surgery: A Staged Approach for Severely Injured PatientsMAMA LALANo ratings yet
- Evolving Science of Trauma Resus 2021-06-17 17-57-30Document22 pagesEvolving Science of Trauma Resus 2021-06-17 17-57-30Paulina CastilloNo ratings yet
- Resuscitative Endovascular Balloon Occlusion of The Aorta (REBOA) : An Updated ReviewDocument9 pagesResuscitative Endovascular Balloon Occlusion of The Aorta (REBOA) : An Updated ReviewLuis-alfredo Perez Bolde HernandezNo ratings yet
- NEJM 2 5 Mack Tavi1Document11 pagesNEJM 2 5 Mack Tavi1Mr. LNo ratings yet
- Informed Consent in Elective and Emergency LaparosDocument2 pagesInformed Consent in Elective and Emergency LaparosFadi NasrallahNo ratings yet
- Complicaciones de Ligadura de HipogastricasDocument9 pagesComplicaciones de Ligadura de Hipogastricasmanuel barrientosNo ratings yet
- Effects of Ultrasound and Ultrasound Contrast AgenDocument10 pagesEffects of Ultrasound and Ultrasound Contrast AgenWaleed sattarNo ratings yet
- GCSP 2015 04 044Document11 pagesGCSP 2015 04 044RamadhyanNo ratings yet
- Op Tech HybridDocument46 pagesOp Tech Hybridopbhi3No ratings yet
- Transcatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future DirectionsDocument22 pagesTranscatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future DirectionsgNo ratings yet
- Zone 3 REBOA EvaluationDocument7 pagesZone 3 REBOA EvaluationJean CotteNo ratings yet
- Dr. Aisha Al-Zuhair General Surgery Kfhu - Khobar - Saudi Arabia Dec 16, 2009Document75 pagesDr. Aisha Al-Zuhair General Surgery Kfhu - Khobar - Saudi Arabia Dec 16, 2009Bagus PattiwaelNo ratings yet
- Hypothermic Machine Preservation in Human Liver Transplantation: The First Clinical SeriesDocument10 pagesHypothermic Machine Preservation in Human Liver Transplantation: The First Clinical SeriesRodolpho ViégasNo ratings yet
- Minimally Invasive Direct Cardiac MassagDocument13 pagesMinimally Invasive Direct Cardiac MassagTM AnNo ratings yet
- ACO Peripro 2016Document10 pagesACO Peripro 2016Philippe Bocanegra FernándezNo ratings yet
- Hemostat 1Document6 pagesHemostat 1Derrick HartNo ratings yet
- What's New in Cardiopulmonary BypassDocument31 pagesWhat's New in Cardiopulmonary Bypass凌晓敏No ratings yet
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDocument9 pagesSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- Left Ventricular Assist DevicesDocument14 pagesLeft Ventricular Assist DevicesLuis Alberto Caneo VergaraNo ratings yet
- Aneurysm Brain and Hyperbaric Chamber AIT - Art - 37989-10Document7 pagesAneurysm Brain and Hyperbaric Chamber AIT - Art - 37989-10cooleraid884No ratings yet
- HIP ORTHOPEDICS October 2008Document4 pagesHIP ORTHOPEDICS October 2008kennice_nereaNo ratings yet
- TIMBUL D.1 Scenario 3 - Amarissa A. Tsabita - 20536 - Group 3Document4 pagesTIMBUL D.1 Scenario 3 - Amarissa A. Tsabita - 20536 - Group 3Amarissa A. TsabitaNo ratings yet
- Short - and Long-Term Outcomes at A Single InstitutionDocument7 pagesShort - and Long-Term Outcomes at A Single InstitutionJonathan Frimpong AnsahNo ratings yet
- Reconstruccion MamariaDocument9 pagesReconstruccion MamariadiogenesNo ratings yet
- Repair of Functional Tricuspid Regurgitation: Comparison Between Suture Annuloplasty and Rings AnnuloplastyDocument7 pagesRepair of Functional Tricuspid Regurgitation: Comparison Between Suture Annuloplasty and Rings AnnuloplastyKarthik RamanNo ratings yet
- A Case of Placenta Percreta With Massive Hemorrhage During Cesarean SectionDocument5 pagesA Case of Placenta Percreta With Massive Hemorrhage During Cesarean Sectiondiijah678No ratings yet
- Application Brief: Abdominal Aortic AneurysmDocument6 pagesApplication Brief: Abdominal Aortic AneurysmVisualSonicsNo ratings yet
- 2019 Journal of Thoracic and Cardiovascular SurgeryDocument10 pages2019 Journal of Thoracic and Cardiovascular SurgeryFernando ZanoniNo ratings yet
- Oral Oncology: Mark K. Wax, James AzziDocument4 pagesOral Oncology: Mark K. Wax, James Azzicr89omfNo ratings yet
- Transcatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsFrom EverandTranscatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsNo ratings yet
- 1 s2.0 S0002961011001097 MainDocument5 pages1 s2.0 S0002961011001097 Mainyacine26No ratings yet
- 1 s2.0 S1053249809009061 MainDocument1 page1 s2.0 S1053249809009061 MaincignalNo ratings yet
- Control de Daños TraumaDocument6 pagesControl de Daños TraumaOscar MerinoNo ratings yet
- AJCC 8th Edition Staging System For PathologicallyDocument3 pagesAJCC 8th Edition Staging System For Pathologicallyandynuransyah01No ratings yet
- 2010 JASE Revisión de La Seguridad Del ETE PDFDocument13 pages2010 JASE Revisión de La Seguridad Del ETE PDFmagnavlerNo ratings yet
- Microcirculatory Effects of Local and Remote Ischemic Preconditioning in Supraceliac Aortic ClampingDocument9 pagesMicrocirculatory Effects of Local and Remote Ischemic Preconditioning in Supraceliac Aortic ClampingFernando ZanoniNo ratings yet
- The Shortfall in Long-Term Survival of Patients With Repaired Thoracic Orabdominal Aortic Aneurysms Retrospective CaseeControl Analysis Ofhospital Episode StatisticsDocument9 pagesThe Shortfall in Long-Term Survival of Patients With Repaired Thoracic Orabdominal Aortic Aneurysms Retrospective CaseeControl Analysis Ofhospital Episode StatisticsJeffery TaylorNo ratings yet
- Hypovolemic Shock ResuscitationDocument21 pagesHypovolemic Shock ResuscitationM Lutfi FananiNo ratings yet
- Swanson 2007Document5 pagesSwanson 2007Giancarlo Maruri MunarettoNo ratings yet
- Reduction in Deep Sternal Wound Infection With Use of A Peristernal Cable-Tie Closure System: A Retrospective Case SeriesDocument7 pagesReduction in Deep Sternal Wound Infection With Use of A Peristernal Cable-Tie Closure System: A Retrospective Case SeriesRafailiaNo ratings yet
- ResucitacionhemostaticaclinicascirugiaDocument15 pagesResucitacionhemostaticaclinicascirugiaEdwin AlvarezNo ratings yet
- Mormont - Marked 24-h Rest Activity Rhythms Are Associated With Better Quality of LifeDocument9 pagesMormont - Marked 24-h Rest Activity Rhythms Are Associated With Better Quality of LifeFernandoNo ratings yet
- Damage Control Resuscitation: Identification and Treatment of Life-Threatening HemorrhageFrom EverandDamage Control Resuscitation: Identification and Treatment of Life-Threatening HemorrhagePhilip C. SpinellaNo ratings yet
- Clinical Handbook of Cardiac ElectrophysiologyFrom EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverNo ratings yet
- 1991 CuminsDocument14 pages1991 CuminsScience BrasilNo ratings yet
- The European Guideline On Management of Major Bleeding and Coagulopathy Following Trauma: Fifth EditionDocument74 pagesThe European Guideline On Management of Major Bleeding and Coagulopathy Following Trauma: Fifth EditionScience BrasilNo ratings yet
- Jewish Voice For InclusionDocument1 pageJewish Voice For InclusionScience BrasilNo ratings yet
- Appropriate Tourniquet Types in The Pediatric Population: A Systematic ReviewDocument9 pagesAppropriate Tourniquet Types in The Pediatric Population: A Systematic ReviewScience BrasilNo ratings yet
- NEJM Defibrilation Strategies For Refractory VFDocument10 pagesNEJM Defibrilation Strategies For Refractory VFScience BrasilNo ratings yet
- SPSY Course Registration FormDocument1 pageSPSY Course Registration FormScience BrasilNo ratings yet
- Dorot 2022Document167 pagesDorot 2022Science BrasilNo ratings yet
- Trigger ElementDocument3 pagesTrigger ElementScience BrasilNo ratings yet
- Fire Dept TIMA DemobilizationDocument1 pageFire Dept TIMA DemobilizationScience BrasilNo ratings yet
- Despiece Motor Briggs 14hp 400707122102Document58 pagesDespiece Motor Briggs 14hp 400707122102leinadNo ratings yet
- Solid Free Form:: Quilt Flatten Quilt QuiltDocument3 pagesSolid Free Form:: Quilt Flatten Quilt QuiltNaganthrakumar RamaswamyNo ratings yet
- Vegan Starter KitDocument53 pagesVegan Starter KitGabriela GarciaNo ratings yet
- 201 CH 8 Roadmap AnswersDocument2 pages201 CH 8 Roadmap AnswersdraggedfromthemoonNo ratings yet
- LG Rotary Compressor GuideDocument32 pagesLG Rotary Compressor Guideวรศิษฐ์ อ๋อง33% (3)
- Humidity Chamber Tek For Fruiting BRF Cakes - Mushroom Cultivation - Shroomery Message BoardDocument15 pagesHumidity Chamber Tek For Fruiting BRF Cakes - Mushroom Cultivation - Shroomery Message BoardABIYA UNIVERSENo ratings yet
- Roland RD-800 Manuale Stage PianoDocument64 pagesRoland RD-800 Manuale Stage PianoAlberto FicheraNo ratings yet
- Tips On Fatigue - NAVWEPS 00-25-559Document123 pagesTips On Fatigue - NAVWEPS 00-25-559Mark Evan SalutinNo ratings yet
- 28 ElectroplatingElectronicsDocument100 pages28 ElectroplatingElectronicsLaboratorium KIESOWNo ratings yet
- Astronomy at The Frontiers of ScienceDocument380 pagesAstronomy at The Frontiers of ScienceΜαρια100% (1)
- Master Drive 6RA70 Parameter ListDocument186 pagesMaster Drive 6RA70 Parameter Listsanjaya srivastava100% (3)
- Computer Integrated ManufacturingDocument7 pagesComputer Integrated ManufacturingNarendra PalacharlaNo ratings yet
- Concepts of ProbabilityDocument32 pagesConcepts of ProbabilityRushina SinghiNo ratings yet
- Diagram PLTA SLJDocument4 pagesDiagram PLTA SLJMEi Cuiet Luph-LuPhNo ratings yet
- Guitar SetupDocument1 pageGuitar SetupEduardo Maia CardosoNo ratings yet
- Module 6 PDFDocument10 pagesModule 6 PDFTazbir AntuNo ratings yet
- Plant Toxicology, Fourth Edition (Books in Soils, Plants, and The Environment) PDFDocument664 pagesPlant Toxicology, Fourth Edition (Books in Soils, Plants, and The Environment) PDFFahad JavedNo ratings yet
- ConMed v. Cosmescu Et. Al.Document28 pagesConMed v. Cosmescu Et. Al.PriorSmartNo ratings yet
- Agilent DSO5014A Oscilloscope Tutorial: EE105 Lab ExperimentsDocument6 pagesAgilent DSO5014A Oscilloscope Tutorial: EE105 Lab ExperimentshendraprimaNo ratings yet
- Desing Criteria For A Controlled DemolitionDocument12 pagesDesing Criteria For A Controlled Demolitionajmc1No ratings yet
- Internship ReportDocument33 pagesInternship Reportstreamingmedia786No ratings yet
- Week 3 Ipe Review ModuleDocument2 pagesWeek 3 Ipe Review ModuleDarren Ian MaalihanNo ratings yet
- IOA Annual Report 2005Document18 pagesIOA Annual Report 2005matt30911No ratings yet
- 1.master Techniques in Surgery - Esophageal Surgery, 1E (2014)Document456 pages1.master Techniques in Surgery - Esophageal Surgery, 1E (2014)Raul Micu ChisNo ratings yet
- Mineral Resources: Earth ScienceDocument20 pagesMineral Resources: Earth ScienceRegina Mae Narciso NazarenoNo ratings yet
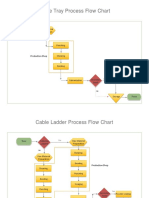
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- BST Chapter 3 Business Environment NotesDocument7 pagesBST Chapter 3 Business Environment NotesAaditi VNo ratings yet