You might also like
- 2022 Camping ReportDocument14 pages2022 Camping ReportIshaNo ratings yet
- TensionersDocument20 pagesTensionersSuresh KumarNo ratings yet
- Big Data Analytics in Healthcare - Promise and PotentialDocument10 pagesBig Data Analytics in Healthcare - Promise and PotentialMohd Otibi100% (1)
- IT Code 402 Notes: CBSE Class 10Document6 pagesIT Code 402 Notes: CBSE Class 10Ritu Aryan0% (1)
- CYPECAD - User's Manual PDFDocument141 pagesCYPECAD - User's Manual PDFBelak1No ratings yet
- SQL HandbookDocument26 pagesSQL HandbookkjhlkNo ratings yet
- Writing The Proposal For A Qualitative Research Methodology ProjectDocument41 pagesWriting The Proposal For A Qualitative Research Methodology Projectrcaba100% (1)
- Data for Nurses: Understanding and Using Data to Optimize Care Delivery in Hospitals and Health SystemsFrom EverandData for Nurses: Understanding and Using Data to Optimize Care Delivery in Hospitals and Health SystemsMolly McNettNo ratings yet
- Assignment 5Document4 pagesAssignment 5WaqasNo ratings yet
- Assessing Needs-Based Supply of Physicians - A Criteria-Led Methodological Review of International Studies in High-Resource SettingsDocument19 pagesAssessing Needs-Based Supply of Physicians - A Criteria-Led Methodological Review of International Studies in High-Resource SettingsPatri BarberNo ratings yet
- s12913 023 09612 3Document15 pagess12913 023 09612 3imidazolaNo ratings yet
- 2004 Beyond RCT - AjphDocument6 pages2004 Beyond RCT - AjphSamuel Andrés AriasNo ratings yet
- A Qualitative Study of Perspectives On The AcceptaDocument11 pagesA Qualitative Study of Perspectives On The Acceptapg8.adoboNo ratings yet
- SSRN Id4302002Document37 pagesSSRN Id4302002Simon fishNo ratings yet
- PublicDocument12 pagesPublicJayapriya jayaramanNo ratings yet
- Applications of Business Analytics in HealthcareDocument13 pagesApplications of Business Analytics in Healthcareshahul kNo ratings yet
- Experiences of Hospital Care For People With Multiple Long-Term Conditions: A Scoping Review of Qualitative ResearchDocument23 pagesExperiences of Hospital Care For People With Multiple Long-Term Conditions: A Scoping Review of Qualitative ResearchBulat StalnoffNo ratings yet
- Lyles Et Al 2020 Using Electronic Health Record Portals To Improve Patient Engagement Research Priorities and BestDocument15 pagesLyles Et Al 2020 Using Electronic Health Record Portals To Improve Patient Engagement Research Priorities and Besttylermichael912No ratings yet
- The Transdiagnostic Intervention For Sleep and CirDocument16 pagesThe Transdiagnostic Intervention For Sleep and CirSimonia CoutinhoNo ratings yet
- The Concept of Access: Definition and Relationship To Consumer SatisfactionDocument15 pagesThe Concept of Access: Definition and Relationship To Consumer SatisfactionTate SimbaNo ratings yet
- Literature Review BMJDocument8 pagesLiterature Review BMJc5qwqy8v100% (1)
- How Can Clinical Epidemiology Better Support Evidence-Based Guidelines and Policies in Low-Income CountriesDocument3 pagesHow Can Clinical Epidemiology Better Support Evidence-Based Guidelines and Policies in Low-Income CountriesEko Wahyu AgustinNo ratings yet
- Articulos 12022Document13 pagesArticulos 12022john jeanfranco melendres velascoNo ratings yet
- Large Language Models For Generating Medical Examinations Systematic reviewBMC Medical EducationDocument11 pagesLarge Language Models For Generating Medical Examinations Systematic reviewBMC Medical Educationalbertus tuhuNo ratings yet
- Interventions To Drive Uptake of VoluntaDocument6 pagesInterventions To Drive Uptake of VoluntaMalkit SinghNo ratings yet
- Times Series and Risk Adjusted Control ChartsDocument2 pagesTimes Series and Risk Adjusted Control Chartselo ochoa coronaNo ratings yet
- Decision Support System Literature ReviewDocument6 pagesDecision Support System Literature Reviewc5j2ksrg100% (1)
- 2020 - Quality and Women's Satisfaction With Referral System Systematic ReviewDocument16 pages2020 - Quality and Women's Satisfaction With Referral System Systematic ReviewTaklu Marama M. BaatiiNo ratings yet
- Peer Review - COMPLETE - EDITEDDocument4 pagesPeer Review - COMPLETE - EDITEDDavid KaranuNo ratings yet
- Lizarondo 2014 PerformanceEvalDocument13 pagesLizarondo 2014 PerformanceEvalKamila AmmarNo ratings yet
- qt5j15k0nf NosplashDocument2 pagesqt5j15k0nf NosplashsinayaphetNo ratings yet
- Literature Review On HmisDocument7 pagesLiterature Review On Hmisea219sww100% (1)
- Navigation Programs To Support Community-Dwelling Individuals With Life-Limiting Illness: Determinants of ImplementationDocument11 pagesNavigation Programs To Support Community-Dwelling Individuals With Life-Limiting Illness: Determinants of ImplementationarysiaNo ratings yet
- Privett and Gonsalvez (2014) The Top Ten Global Health Supply Chain Issues - Perspectives From The Field (ORHC)Document6 pagesPrivett and Gonsalvez (2014) The Top Ten Global Health Supply Chain Issues - Perspectives From The Field (ORHC)Damonda PradiptaNo ratings yet
- Healthcare Logistics and Supply Chain Issues and Future ChallengesDocument4 pagesHealthcare Logistics and Supply Chain Issues and Future Challengespallavi mehraNo ratings yet
- Applications of Business Analytics in Healthcare: SciencedirectDocument12 pagesApplications of Business Analytics in Healthcare: SciencedirectSujay ShahNo ratings yet
- The Impact of Hospital Accreditation On The QualitDocument13 pagesThe Impact of Hospital Accreditation On The QualitRai Riska Resty WasitaNo ratings yet
- 2008a Sanhueza Leiva BalakrishnanDocument27 pages2008a Sanhueza Leiva BalakrishnanMych BogdanNo ratings yet
- The Impact of Hospital Accreditation On The Quality of Healthcare A Systematic Literature ReviewDocument12 pagesThe Impact of Hospital Accreditation On The Quality of Healthcare A Systematic Literature Reviewners edisapNo ratings yet
- Classification and Regression Tree Analy PDFDocument10 pagesClassification and Regression Tree Analy PDFEduard MacoveiNo ratings yet
- s12913 022 08783 9Document23 pagess12913 022 08783 9Shuai ShaoNo ratings yet
- Lectura en InglésDocument8 pagesLectura en InglésReev KatsNo ratings yet
- Hrm&a Group AssignmentDocument8 pagesHrm&a Group AssignmentDivya ParmarNo ratings yet
- Maya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewDocument18 pagesMaya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewsukmarahastriNo ratings yet
- Nurses' Utilization and Perception of The Community/Public Health Nursing CredentialDocument6 pagesNurses' Utilization and Perception of The Community/Public Health Nursing CredentialViolin Irene NinefNo ratings yet
- Electronic Med Rec AOMDocument25 pagesElectronic Med Rec AOMfatiisaadatNo ratings yet
- How Do Health Systems Improve Patient Flow When Services Are Misaligned With Population Needs? A Qualitative StudyDocument11 pagesHow Do Health Systems Improve Patient Flow When Services Are Misaligned With Population Needs? A Qualitative StudySara Adi KreindlerNo ratings yet
- Geostatistical Linkage of National Demographic and Health Survey Data: A Case Study of TanzaniaDocument14 pagesGeostatistical Linkage of National Demographic and Health Survey Data: A Case Study of Tanzaniaobaidur.slghnNo ratings yet
- Running Head: Health Information Technology 1Document12 pagesRunning Head: Health Information Technology 1api-469824583No ratings yet
- Investigating Discrete Event Simulation Method To Assess The Effectiveness of Wearable Health Monitoring Devices 2014 Procedia Economics and FinanceDocument19 pagesInvestigating Discrete Event Simulation Method To Assess The Effectiveness of Wearable Health Monitoring Devices 2014 Procedia Economics and FinanceRupaliNo ratings yet
- 01 Kruse 2016Document7 pages01 Kruse 2016Claudio PinuerNo ratings yet
- Guidance To Best Tools and Practices ForDocument33 pagesGuidance To Best Tools and Practices Forcvdk8dc8sbNo ratings yet
- 2023 Article 6059Document12 pages2023 Article 6059Chloe BujuoirNo ratings yet
- Literature Review On Clinical Decision Support System Reducing Medical ErrorDocument7 pagesLiterature Review On Clinical Decision Support System Reducing Medical Errorgvzwyd4nNo ratings yet
- Systematic Quantitative Literature Review MethodDocument7 pagesSystematic Quantitative Literature Review Methodc5qdk8jnNo ratings yet
- Performing A Literature Review BMJDocument8 pagesPerforming A Literature Review BMJfvgrsm8r100% (1)
- Capturing Patients Needs in CaDocument18 pagesCapturing Patients Needs in CaAnissa ResianaNo ratings yet
- Trachoma Survey Methods A Literature ReviewDocument5 pagesTrachoma Survey Methods A Literature Reviewiiaxjkwgf100% (1)
- Literature Review of Decision Support SystemDocument11 pagesLiterature Review of Decision Support Systemafmzmqwdglhzex100% (1)
- 10.1108@jhom 06 2018 0176Document19 pages10.1108@jhom 06 2018 0176Karenziitah Katiuska Sosa RamirezNo ratings yet
- Symposium: Challenges in Targeting Nutrition Programs: Discussion: Targeting Is Making Trade-OffsDocument4 pagesSymposium: Challenges in Targeting Nutrition Programs: Discussion: Targeting Is Making Trade-OffsMukhlidahHanunSiregarNo ratings yet
- Assignment 3Document6 pagesAssignment 3WaqasNo ratings yet
- Literature Review Developing Competencies For Health Promotion Deliverable 3bDocument10 pagesLiterature Review Developing Competencies For Health Promotion Deliverable 3bxfeivdsifNo ratings yet
- 53Document10 pages53Steve GannabanNo ratings yet
- Osteoarthritis Physical Activity Care Pathway (OA-PCP) : Results of A Feasibility TrialDocument11 pagesOsteoarthritis Physical Activity Care Pathway (OA-PCP) : Results of A Feasibility TrialrahmarahmatNo ratings yet
- 4.3.3.4 Packet Tracer - Configuring VPN Tunnel ModeDocument3 pages4.3.3.4 Packet Tracer - Configuring VPN Tunnel ModeFahadNo ratings yet
- Revision Status History For F-70H Compressor - 04-23-15Document3 pagesRevision Status History For F-70H Compressor - 04-23-15Daniel Martinez CollazoNo ratings yet
- TRS SMCDocument8 pagesTRS SMCSeverino NetoNo ratings yet
- MongoDB Update RemoveDocument6 pagesMongoDB Update RemovePreeti SinghNo ratings yet
- The Student Manage Their Time Using TechnologyDocument2 pagesThe Student Manage Their Time Using TechnologyJed Andrei RubioNo ratings yet
- s11423 018 9598 6 PDFDocument17 pagess11423 018 9598 6 PDFJoy PascoNo ratings yet
- Er DiagramDocument3 pagesEr Diagramرهيب صادق النظيفNo ratings yet
- 1st AssignmentDocument3 pages1st AssignmentM10r SidhuNo ratings yet
- Drivability GuideDocument144 pagesDrivability GuideSuciu Florin100% (1)
- Samsung A330Document48 pagesSamsung A330cipcozianu_297765774No ratings yet
- Led Performance Highbay 150 W 6500 K Gen2: Product DatasheetDocument3 pagesLed Performance Highbay 150 W 6500 K Gen2: Product DatasheetTerry wei shengNo ratings yet
- 1. pH计 pH Meters 24.3.6Document27 pages1. pH计 pH Meters 24.3.6Valentine MalamaNo ratings yet
- Placement Code of Conduct PDFDocument13 pagesPlacement Code of Conduct PDFEdwinNo ratings yet
- Decidability & Rice's Theorem: Arjun Suresh For GATE Overflow Helped by Subarna and SukanyaDocument47 pagesDecidability & Rice's Theorem: Arjun Suresh For GATE Overflow Helped by Subarna and SukanyaAbhishek JainNo ratings yet
- CYNOSUREDocument49 pagesCYNOSUREMadge FordNo ratings yet
- AEPC Annual Report 2019-20Document100 pagesAEPC Annual Report 2019-20Parvez khanNo ratings yet
- Pool Control Prof IDocument2 pagesPool Control Prof IskromenNo ratings yet
- Abb Utilities GMBH: ApplicationDocument2 pagesAbb Utilities GMBH: Applicationantlsm733No ratings yet
- English For Career DevelopmentDocument5 pagesEnglish For Career DevelopmentJuan Daniel Vargas PerdomoNo ratings yet
- Tenant Management: Signup-Login Upload Property Details My AccountDocument14 pagesTenant Management: Signup-Login Upload Property Details My AccountANIRUDDH MAKWANANo ratings yet
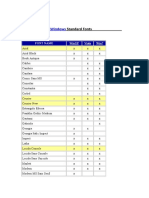
- Microsoft Windows Standard FontsDocument2 pagesMicrosoft Windows Standard FontscrosupermanNo ratings yet
- CHUANGYI CatalogueDocument13 pagesCHUANGYI CataloguebereketNo ratings yet
- CFD Project - Jan 2022Document2 pagesCFD Project - Jan 2022Aqil ZainieNo ratings yet
- Electronics Coaching Notes 5Document6 pagesElectronics Coaching Notes 5Jojo TakatoNo ratings yet