You might also like
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- 09 Living On The FrontlineDocument5 pages09 Living On The FrontlineAjitkumar PulagurthaNo ratings yet
- Serology Report: Test Units Normal RangeDocument1 pageSerology Report: Test Units Normal RangeKrishna Shrestha100% (2)
- The Plot Against Asthma and Allergy PatientsDocument422 pagesThe Plot Against Asthma and Allergy PatientsAngelo100% (1)
- Occupational Therapy Initial EvaluationDocument10 pagesOccupational Therapy Initial EvaluationNerissa BanguiNo ratings yet
- Degenerative Diseases NCMB316 SEC1 AMENINDocument4 pagesDegenerative Diseases NCMB316 SEC1 AMENINHermin TorresNo ratings yet
- COURSE TASK 6 - Degenerative Table SummaryDocument2 pagesCOURSE TASK 6 - Degenerative Table SummaryJordz PlaciNo ratings yet
- Revalida Review NotesDocument14 pagesRevalida Review NotesBryan Lloyd RayatNo ratings yet
- Degenerative and Demyelinating Disorders - Dr. WongDocument7 pagesDegenerative and Demyelinating Disorders - Dr. WongMonique BorresNo ratings yet
- Pathology of Peripheral Nerve and Skeletal Muscle - DADocument46 pagesPathology of Peripheral Nerve and Skeletal Muscle - DASinta Dewi AdityaniNo ratings yet
- MS PD ALS Table W23Document7 pagesMS PD ALS Table W23romaisahaghdoostNo ratings yet
- Common Diseases That Can Affect Our Nervous SystemDocument1 pageCommon Diseases That Can Affect Our Nervous SystemJhe-An PilapilNo ratings yet
- GuillainDocument4 pagesGuillainanime listNo ratings yet
- PDF DocumentDocument95 pagesPDF DocumentHannah AmerolNo ratings yet
- Peripheral NeuropathiesDocument10 pagesPeripheral NeuropathiesFergieNo ratings yet
- Growth and DevelopmentDocument2 pagesGrowth and DevelopmentbugogiNo ratings yet
- 10 - Disorders of Consciousness and Language I (Coma and Confusional States) LectureDocument119 pages10 - Disorders of Consciousness and Language I (Coma and Confusional States) LectureRanjit SharmaNo ratings yet
- Unit Xi: Neural Regulation (Motor Disturbances) - Upper Motor Neuron DisorderDocument4 pagesUnit Xi: Neural Regulation (Motor Disturbances) - Upper Motor Neuron DisorderCindy MariscotesNo ratings yet
- Neurophatic PainDocument4 pagesNeurophatic PainicoanamareNo ratings yet
- Management of Patients With Neurologic Infections, Autoimmune Disorders & NeuropathiesDocument92 pagesManagement of Patients With Neurologic Infections, Autoimmune Disorders & NeuropathiesejarnmdNo ratings yet
- Management of Patients With Neurologic Infections Autoimmune Disorders NeuropathiesDocument92 pagesManagement of Patients With Neurologic Infections Autoimmune Disorders Neuropathiesضياء عمارنهNo ratings yet
- Alzheimers DiseaseDocument11 pagesAlzheimers DiseaseCHRISTIAN RAY ALPAS PASILIAONo ratings yet
- Dementia Recentupdates 130920080812 Phpapp01Document58 pagesDementia Recentupdates 130920080812 Phpapp01SantanuNo ratings yet
- PD Als GBS MGDocument9 pagesPD Als GBS MGadd.bdrcNo ratings yet
- Differential Diagnosis (Neuro, Peads)Document1 pageDifferential Diagnosis (Neuro, Peads)manar180406No ratings yet
- Diagnosis, pathogenesis and treatment of primary episodic ataxiasDocument10 pagesDiagnosis, pathogenesis and treatment of primary episodic ataxiasthelegend 2022No ratings yet
- DPW (GBS VS TM)Document29 pagesDPW (GBS VS TM)Muhammad HerryNo ratings yet
- 19 Neuromuscular DisordersDocument39 pages19 Neuromuscular DisordersSara 'Yaa SaraaNo ratings yet
- Etiology: Molecular Mimicry - Myelin-ReactiveDocument2 pagesEtiology: Molecular Mimicry - Myelin-ReactiveJulia SalvioNo ratings yet
- Seizure PathophysiologyDocument3 pagesSeizure PathophysiologyPaula Nantes Nazareth55% (11)
- Pathophysiology of Spongy Degeneration of The Brain: Precipitating FactorsDocument4 pagesPathophysiology of Spongy Degeneration of The Brain: Precipitating FactorsCleobebs AgustinNo ratings yet
- Where Da Lesion atDocument5 pagesWhere Da Lesion atDeeWallyNo ratings yet
- Steven Angelo E. Cruz, PTRPDocument130 pagesSteven Angelo E. Cruz, PTRPJoeNo ratings yet
- GB Syndrome..Document13 pagesGB Syndrome..Shitaljit Irom100% (1)
- Risk Factors:: Pathophysiology of Alzheimer'S DiseaseDocument2 pagesRisk Factors:: Pathophysiology of Alzheimer'S DiseaseJordz PlaciNo ratings yet
- Childhood Epilepsy Etiology, Epidemiology & ManagementDocument6 pagesChildhood Epilepsy Etiology, Epidemiology & ManagementJosh RoshalNo ratings yet
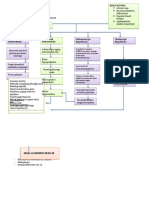
- Pa Tho Physiology of Guillain Barre SyndromeDocument4 pagesPa Tho Physiology of Guillain Barre Syndromenaman24No ratings yet
- Dementia 2005Document46 pagesDementia 2005sankethNo ratings yet
- Causes and Characteristics of Onset of Weakness in ExtremitiesDocument2 pagesCauses and Characteristics of Onset of Weakness in ExtremitiesYulyani PratiwiNo ratings yet
- CipaDocument5 pagesCipakomal nanavatiNo ratings yet
- Head Injury Diagnosis and ManagementDocument41 pagesHead Injury Diagnosis and ManagementChristian Dave EndinoNo ratings yet
- Requirement in PathophysiologyDocument38 pagesRequirement in PathophysiologyckathreenahNo ratings yet
- Skeletal Muscle & Nerve Pathology GuideDocument221 pagesSkeletal Muscle & Nerve Pathology GuideGenepol Dente100% (2)
- 6 Multiple SclerosisDocument86 pages6 Multiple SclerosismuhammadridhwanNo ratings yet
- Acute Manifestations of Neuromuscular DiseaseDocument10 pagesAcute Manifestations of Neuromuscular DiseasetsyrahmaniNo ratings yet
- Sudheimer Week 10 Schizophrenia Parkinsons AlzheimersDocument27 pagesSudheimer Week 10 Schizophrenia Parkinsons Alzheimersdaedalusx99No ratings yet
- Understanding the basic mechanisms of neurodegenerative disordersDocument107 pagesUnderstanding the basic mechanisms of neurodegenerative disordersPRONTO DIAGNOSTICNo ratings yet
- Neurology: Apprauching and Localizing Neurological LesionDocument53 pagesNeurology: Apprauching and Localizing Neurological LesionMahad IbrahemNo ratings yet
- Neurological disorders affect 1 in 6 peopleDocument2 pagesNeurological disorders affect 1 in 6 people박우진No ratings yet
- Biology of Parkinson S Disease Pathogenesis and Pathophysiology of A Multisystem Neurodegenerative DisorderDocument23 pagesBiology of Parkinson S Disease Pathogenesis and Pathophysiology of A Multisystem Neurodegenerative DisorderNelly LeónNo ratings yet
- Multiple Sclerosis: Paola Viñé OrtegaDocument21 pagesMultiple Sclerosis: Paola Viñé OrtegaPaola ViñéNo ratings yet
- Paraneoplastic Disorders of the Central Nervous SystemDocument71 pagesParaneoplastic Disorders of the Central Nervous Systempreeti sharmaNo ratings yet
- Neurology - Weakness PatternsDocument2 pagesNeurology - Weakness PatternsAnisah AliNo ratings yet
- PP MorbidityDocument65 pagesPP MorbidityRaymart MacasaetNo ratings yet
- Aortic StenosisDocument10 pagesAortic Stenosisjudith dela cruzNo ratings yet
- Understanding Anf Managing VertigoDocument67 pagesUnderstanding Anf Managing VertigoGede SuputraNo ratings yet
- Neuronal Response To InjuryDocument37 pagesNeuronal Response To InjuryShems AlmusawiNo ratings yet
- NEUROLOGY Genetics of the Heredodegenerative Ataxias: Differential Diagnosis and SyndromesDocument13 pagesNEUROLOGY Genetics of the Heredodegenerative Ataxias: Differential Diagnosis and SyndromesJerome ReyNo ratings yet
- Nervous SystemDocument2 pagesNervous SystemBianca Ysabelle RegalaNo ratings yet
- Neurology and Special Senses ' Neurology and Special Senses ' Section IiiDocument20 pagesNeurology and Special Senses ' Neurology and Special Senses ' Section IiiLuis Jose VelazquezNo ratings yet
- Module 2 - Acute Non Traumatic WeaknessDocument55 pagesModule 2 - Acute Non Traumatic WeaknessRick RanitNo ratings yet
- Cefalea Por Hipotensión.Document8 pagesCefalea Por Hipotensión.Farid Santiago Abedrabbo LombeydaNo ratings yet
- Musculoskeletal ChartsDocument27 pagesMusculoskeletal Chartssurviving nursing school100% (3)
- W3 - MEDSURG Neurologic Disorders (MS, MG, and Parkisons's)Document11 pagesW3 - MEDSURG Neurologic Disorders (MS, MG, and Parkisons's)Kyla L. MadjadNo ratings yet
- Nosodes in Homeopathy - Dr. David LittleDocument9 pagesNosodes in Homeopathy - Dr. David LittleNOOKALA UMA SHANKAR0% (1)
- Asepsis 1Document52 pagesAsepsis 1严子明 Renz Ryan SevillenoNo ratings yet
- Name of DrugDocument10 pagesName of DrugBianx PradoNo ratings yet
- Out 7 PDFDocument8 pagesOut 7 PDFAfif Al FatihNo ratings yet
- CPH SIM Week 1-3Document23 pagesCPH SIM Week 1-3Vine OrtegaNo ratings yet
- Acute Tubular Necrosis 2Document19 pagesAcute Tubular Necrosis 2Sangeeta BSRNo ratings yet
- Anthony J. Destefano, PHD: Growing ThreatsDocument23 pagesAnthony J. Destefano, PHD: Growing Threatstamuno7No ratings yet
- Thoracic Surgery: Cervical, Thoracic and Abdominal ApproachesDocument1,068 pagesThoracic Surgery: Cervical, Thoracic and Abdominal ApproachesAlexandru GibuNo ratings yet
- DR Amaefula, E. Temple MBBS, Fwacs, Faoi,: Inflamation, Infection, and Use of Antibiotics in SurgeryDocument40 pagesDR Amaefula, E. Temple MBBS, Fwacs, Faoi,: Inflamation, Infection, and Use of Antibiotics in SurgeryPrincewill SeiyefaNo ratings yet
- Nature: Home Per Request Discharge Against Medical AdviceDocument5 pagesNature: Home Per Request Discharge Against Medical AdviceJeroham CoNo ratings yet
- BVU Fellowship in Pediatric Critical CareDocument1 pageBVU Fellowship in Pediatric Critical CareSuman MondalNo ratings yet
- 4 Curs Osteomielita Engl BunDocument41 pages4 Curs Osteomielita Engl BunCatalin PaulNo ratings yet
- Osteoporosis: Causes, Incidence, and Risk FactorsDocument5 pagesOsteoporosis: Causes, Incidence, and Risk FactorsEmeka JusticeNo ratings yet
- Modern Nursing StoryboardDocument3 pagesModern Nursing StoryboardALIFIA NUR SELINANo ratings yet
- Ayushman Bharat hospitals in BangaloreDocument163 pagesAyushman Bharat hospitals in BangaloreShreedhar KadkolNo ratings yet
- FDA Warning Letter 3 2010Document2 pagesFDA Warning Letter 3 2010Nalini RajamannanNo ratings yet
- Femto-Lasik laser eye surgery explainedDocument4 pagesFemto-Lasik laser eye surgery explainedvrlftrNo ratings yet
- FC Rad Onc (SA) Part II Past Papers - 2012 Mar 6-5-2014Document4 pagesFC Rad Onc (SA) Part II Past Papers - 2012 Mar 6-5-2014matentenNo ratings yet
- Mongolian SpotsDocument9 pagesMongolian SpotsiekafzNo ratings yet
- Plantar Fascitis PDFDocument19 pagesPlantar Fascitis PDFDSouza Dominic RoyNo ratings yet
- Hydrocephalus 9Document9 pagesHydrocephalus 9Shesly PhilominaNo ratings yet
- Clinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDocument4 pagesClinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDesi AdiyatiNo ratings yet
- Eye MCQDocument1 pageEye MCQLoveKumarNo ratings yet
- Animals Research DebateDocument2 pagesAnimals Research DebateearlzyNo ratings yet
- 340B Drug Discounts WPDocument20 pages340B Drug Discounts WPScott McClallenNo ratings yet
- Micp Lec (Week - 4) Host Response To InfectionDocument15 pagesMicp Lec (Week - 4) Host Response To Infectioncaitie miracleNo ratings yet