You might also like
- Oncologic EmergenciesDocument3 pagesOncologic EmergenciesMiguel Cuevas DolotNo ratings yet
- Bariatric GuidelinesDocument83 pagesBariatric Guidelinessavvy_as_98100% (1)
- Tumors of The Head and NeckDocument5 pagesTumors of The Head and NeckMiguel CuevasNo ratings yet
- Scanning Technique of KidneysDocument103 pagesScanning Technique of KidneysPhuntsho OngmoNo ratings yet
- Surgical Site InfectionsDocument52 pagesSurgical Site Infectionssahabatsalam07100% (5)
- Renal Ultrasound BMUS Study Day: Rosie ConlonDocument72 pagesRenal Ultrasound BMUS Study Day: Rosie ConlonlllorellleiNo ratings yet
- Renal Ultrasound: Diana Pancu, MDDocument76 pagesRenal Ultrasound: Diana Pancu, MDYoungFanjiens100% (1)
- Renal Ultrasound: Diana Pancu, MDDocument55 pagesRenal Ultrasound: Diana Pancu, MDawansurfNo ratings yet
- Emergency in Urology - Edit241021Document76 pagesEmergency in Urology - Edit241021Alverina Ode Nifaki100% (1)
- ASSIGNMENT Surgical Instruments (On-Going)Document5 pagesASSIGNMENT Surgical Instruments (On-Going)Wyen Cabatbat100% (4)
- Emergency UrologyDocument56 pagesEmergency UrologyayususantinaNo ratings yet
- Clinical PelvimetryDocument3 pagesClinical PelvimetryValerie Gonzaga-Carandang0% (1)
- Leopold's ManeuverDocument3 pagesLeopold's ManeuverKristine Marie de MesaNo ratings yet
- Perioperative Nursing CareDocument17 pagesPerioperative Nursing CareMisikir Eyob100% (1)
- Urogenital Imaging: A Problem-Oriented ApproachFrom EverandUrogenital Imaging: A Problem-Oriented ApproachS. MorcosRating: 3 out of 5 stars3/5 (1)
- 10 1016@j Chest 2020 09 269Document29 pages10 1016@j Chest 2020 09 269Wanderson100% (1)
- 08 TV Quistes Renales Por TCDocument10 pages08 TV Quistes Renales Por TCDonaldo ReleyNo ratings yet
- Kidneys: PGI Tricia Mae J. BatohanonDocument23 pagesKidneys: PGI Tricia Mae J. BatohanonTrishie BatohanonNo ratings yet
- Renal CystsDocument28 pagesRenal CystsAliyah Tofani PawelloiNo ratings yet
- 01 CT Anatomia RiñonDocument16 pages01 CT Anatomia RiñonDonaldo ReleyNo ratings yet
- Pyelonephritis 2018Document2 pagesPyelonephritis 2018greskpremium8No ratings yet
- 03 CT Absceso Piogeno HepaticoDocument4 pages03 CT Absceso Piogeno HepaticoPablo TalamantesNo ratings yet
- Kidneys Focal Lesions, Degeneration and InflammationDocument31 pagesKidneys Focal Lesions, Degeneration and Inflammationivan KeshariNo ratings yet
- AB-M02-CH2.3-LIVER PATH-Focal AbnormalitiesDocument20 pagesAB-M02-CH2.3-LIVER PATH-Focal AbnormalitiesThomas AndersonNo ratings yet
- Kidney & Urinary Tract USDocument62 pagesKidney & Urinary Tract USBayarbaatar BoldNo ratings yet
- The Kidneys & Ureters - NEWDocument12 pagesThe Kidneys & Ureters - NEWnasir iqbalNo ratings yet
- Patofosiologi Gangguan GinjalDocument43 pagesPatofosiologi Gangguan GinjalKazami KurootsukiNo ratings yet
- Cystic Diseases of The KidneyDocument14 pagesCystic Diseases of The KidneyBarda GulanNo ratings yet
- Bilateral: Etiology Manifestations Diagnosis Management, Prognosis, Prevention ComplicationsDocument8 pagesBilateral: Etiology Manifestations Diagnosis Management, Prognosis, Prevention ComplicationsJayesh MahajanNo ratings yet
- Review - Acute Care Surgery Part 1Document63 pagesReview - Acute Care Surgery Part 1Loveknot BG BoripbinNo ratings yet
- Congenitalrenalanomalies 161209072225Document68 pagesCongenitalrenalanomalies 161209072225Ali SlimaniNo ratings yet
- Aortic Aneurysm-: NUR2744 Test 3 OutlineDocument10 pagesAortic Aneurysm-: NUR2744 Test 3 Outlinemara5140No ratings yet
- Urogenital Imejing: DR - Ali Imran Lubis SP - RadDocument16 pagesUrogenital Imejing: DR - Ali Imran Lubis SP - RadMuhammad AL Farisi SutrisnoNo ratings yet
- Emergency Radiology Urinary Tract - 240227 - 073849Document126 pagesEmergency Radiology Urinary Tract - 240227 - 073849dr.tonichenNo ratings yet
- 03 US Alteraciones Congenitas RiñonDocument7 pages03 US Alteraciones Congenitas RiñonDonaldo ReleyNo ratings yet
- Renal FailureDocument60 pagesRenal Failuredr_shamimrNo ratings yet
- 990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用Document77 pages990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用juice119100% (2)
- Toronto Notes Nephrology 2015 32Document1 pageToronto Notes Nephrology 2015 32JUSASBNo ratings yet
- DR - Shamim Rima MBBS, FCGP, Dmu M.Phil Radiology & ImagingDocument154 pagesDR - Shamim Rima MBBS, FCGP, Dmu M.Phil Radiology & Imagingdr_shamimrNo ratings yet
- Clinical Course Discussion: Oregon Health & Science University, Portland, OregonDocument1 pageClinical Course Discussion: Oregon Health & Science University, Portland, OregonperjadanutNo ratings yet
- Renal Final 3Document48 pagesRenal Final 3IqraNo ratings yet
- Degenerative Pathology of The Spine NewDocument42 pagesDegenerative Pathology of The Spine NewA SNo ratings yet
- L. Genitourinary ImagingDocument36 pagesL. Genitourinary ImagingkamariahsamahNo ratings yet
- Laboratory Skills Session On RadiologyDocument7 pagesLaboratory Skills Session On Radiologyupcm2014blockANo ratings yet
- Pato Semester 2Document7 pagesPato Semester 2Muhammad AminNo ratings yet
- 6 SURGERY II 6 - Pediatric UrologyDocument6 pages6 SURGERY II 6 - Pediatric UrologyDeann RoscomNo ratings yet
- 1 Urine Sediments For The Diagnosis of Kidney Disease Prof AdelDocument64 pages1 Urine Sediments For The Diagnosis of Kidney Disease Prof AdelNEsreNo ratings yet
- Surgery of Kidney: Presented To: Dr. Faisal Kayanni Presented byDocument10 pagesSurgery of Kidney: Presented To: Dr. Faisal Kayanni Presented byMr. AlphaNo ratings yet
- 4.3 Skenario 4 Sasbel 2Document9 pages4.3 Skenario 4 Sasbel 2ahmadNo ratings yet
- Seminar 15 - UTIDocument41 pagesSeminar 15 - UTIBONG AIKCHINGNo ratings yet
- IVU - DR Juned A AnsariDocument50 pagesIVU - DR Juned A AnsariJuned A AnsariNo ratings yet
- Peritonitis Sek UnderDocument2 pagesPeritonitis Sek UnderAnonymous eF8cmVvJaNo ratings yet
- AneurysmsDocument18 pagesAneurysmsSaad Anwar GujjarNo ratings yet
- History and Physical Exam UrologyDocument25 pagesHistory and Physical Exam UrologyAnas HamadNo ratings yet
- Colic RenalDocument21 pagesColic RenalJoyaa ShaloomNo ratings yet
- Bladder MassDocument1 pageBladder MassMatthew Lagu TatayeNo ratings yet
- 15 - Genitourinary RadiologyDocument9 pages15 - Genitourinary RadiologyAbhijith J PuttananickalNo ratings yet
- Genitourinary Emergency: Prof. Dr. Mostafa Sakr Genitourinary SurgeryDocument83 pagesGenitourinary Emergency: Prof. Dr. Mostafa Sakr Genitourinary SurgeryDr. NasrumminallahNo ratings yet
- The Renal Sinus - Pathologic Spectrum and Multimodality Imaging Approach - RGDocument15 pagesThe Renal Sinus - Pathologic Spectrum and Multimodality Imaging Approach - RGVan PhamNo ratings yet
- Anomalies of Rotation To CDDocument3 pagesAnomalies of Rotation To CDGren May Angeli MagsakayNo ratings yet
- UroradiologyAUA 2012Document142 pagesUroradiologyAUA 2012Andro GalaxNo ratings yet
- Estudios de Imagen RenalDocument7 pagesEstudios de Imagen RenalVanessa MartinezNo ratings yet
- Kidney DisordersDocument14 pagesKidney Disordershussain AltaherNo ratings yet
- Barium Procedures of GIT and GUT ImagingDocument73 pagesBarium Procedures of GIT and GUT ImagingAnshul VarshneyNo ratings yet
- Modern Management of Renal Colic: 14 Urology SeminarDocument4 pagesModern Management of Renal Colic: 14 Urology SeminarAliNo ratings yet
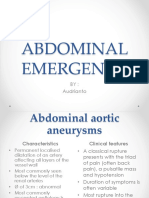
- Abdominal Emergency: BY: AudriantoDocument109 pagesAbdominal Emergency: BY: AudriantoNisa Thayalisha HadiNo ratings yet
- 12 TV Trauma RenalDocument9 pages12 TV Trauma RenalDonaldo ReleyNo ratings yet
- 03 US Alteraciones Congenitas RiñonDocument7 pages03 US Alteraciones Congenitas RiñonDonaldo ReleyNo ratings yet
- UrografiaDocument68 pagesUrografiaDonaldo ReleyNo ratings yet
- 03 CT Alteraciones Congenitas RiñonDocument8 pages03 CT Alteraciones Congenitas RiñonDonaldo ReleyNo ratings yet
- Expo Us Anatomia RiñonDocument32 pagesExpo Us Anatomia RiñonDonaldo ReleyNo ratings yet
- 07 TM Genitourinary Radiology - Kidney, Bladder and Urethra (2013, Springer)Document19 pages07 TM Genitourinary Radiology - Kidney, Bladder and Urethra (2013, Springer)Donaldo ReleyNo ratings yet
- 09 TM CA Celulas Renales Por USDocument6 pages09 TM CA Celulas Renales Por USDonaldo ReleyNo ratings yet
- 4 RX Tórax TEXTO AtelectasiaDocument8 pages4 RX Tórax TEXTO AtelectasiaDonaldo ReleyNo ratings yet
- 5 RX Tórax TEXTO NeumotoraxDocument8 pages5 RX Tórax TEXTO NeumotoraxDonaldo ReleyNo ratings yet
- 5 RX Tórax TEXTO Derrame PleuralDocument10 pages5 RX Tórax TEXTO Derrame PleuralDonaldo ReleyNo ratings yet
- 10 TM Ca Celulas TransicionalesDocument19 pages10 TM Ca Celulas TransicionalesDonaldo ReleyNo ratings yet
- 11 TM AngiomiolipomaDocument9 pages11 TM AngiomiolipomaDonaldo ReleyNo ratings yet
- 10 TV Ca Cel TrasnsicionalesDocument19 pages10 TV Ca Cel TrasnsicionalesDonaldo ReleyNo ratings yet
- Hemostasis: Mechanisms of Blood CoagulationDocument2 pagesHemostasis: Mechanisms of Blood CoagulationAshish SrivastavaNo ratings yet
- Lumbar PunctureDocument1 pageLumbar Puncturemoath qadourahNo ratings yet
- PKT0019 Paket Tonsilektomi One Day Care Kamar Bedah 1 (Satu) TahunDocument2 pagesPKT0019 Paket Tonsilektomi One Day Care Kamar Bedah 1 (Satu) Tahunria rusmawatiNo ratings yet
- Sameh Doss Lower Limb Computer Version 9bs DR NotesDocument139 pagesSameh Doss Lower Limb Computer Version 9bs DR Noteslama.lamis.kharbechNo ratings yet
- Periodontal SurgeryDocument4 pagesPeriodontal SurgeryRinisha SinhaNo ratings yet
- Pcso Mam Program Services and RequirementsDocument12 pagesPcso Mam Program Services and RequirementsJen UmlanoNo ratings yet
- DialysisDocument6 pagesDialysisPrincess Joy Torrijas Factora0% (1)
- Central Hemangioma A Case Report and Review of Lit PDFDocument5 pagesCentral Hemangioma A Case Report and Review of Lit PDFHamba AllahNo ratings yet
- Sir Yahaya Memorial Hospital Birnin Kebbi: Nursing DepartmentDocument7 pagesSir Yahaya Memorial Hospital Birnin Kebbi: Nursing DepartmentyusufNo ratings yet
- Guideline Evaluation Adult LT 4UFb 2015Document98 pagesGuideline Evaluation Adult LT 4UFb 2015Andrei CemîrtanNo ratings yet
- Medtronic Off Pump Training Technique - Event AnnoucementDocument2 pagesMedtronic Off Pump Training Technique - Event AnnoucementTodd SvanoeNo ratings yet
- Forcep DeliveryDocument32 pagesForcep DeliverybbaltazarjaniceNo ratings yet
- Phinma University of PangasinanDocument5 pagesPhinma University of PangasinanLovely CervantesNo ratings yet
- Clinical Spectrum of Atherosclerotic Heart DiseaseDocument50 pagesClinical Spectrum of Atherosclerotic Heart Diseaseadamu mohammadNo ratings yet
- Orientation Jaw RelationDocument31 pagesOrientation Jaw RelationAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Inventaris AlKesDocument46 pagesInventaris AlKesMuhammad AliNo ratings yet
- Equipment Supply List For Problem Mares CSUDocument2 pagesEquipment Supply List For Problem Mares CSUAgnelo DouglasNo ratings yet
- CASE STUDY - ColectomyDocument8 pagesCASE STUDY - ColectomyROSHANNEDANICA VERGARANo ratings yet
- Unit 6 Engineering Perspective Part 1Document8 pagesUnit 6 Engineering Perspective Part 1irakool2014No ratings yet
- Anatomy and Physiology of The Marginal PeriodontiumDocument58 pagesAnatomy and Physiology of The Marginal PeriodontiumTal ShvetsNo ratings yet
- Introduction of Magic Rose UpDocument21 pagesIntroduction of Magic Rose UpanggrainiNo ratings yet
- Cleft Lip and Palate: Protocol For Orthodontics Treatment: October 2021Document13 pagesCleft Lip and Palate: Protocol For Orthodontics Treatment: October 2021Aditya RamadhanNo ratings yet
- Prontosan Wound Irrigation Solution: With Kci V.A.C. VerafloDocument1 pageProntosan Wound Irrigation Solution: With Kci V.A.C. VerafloTiiensKeyNo ratings yet