You might also like
- CVV CashoutDocument4 pagesCVV CashoutGisèle HAGNON75% (4)
- Zubair FarooquiDocument7 pagesZubair FarooquiSakila SNo ratings yet
- الرخصة التجارية 2024Document1 pageالرخصة التجارية 2024AL MASSA CONTRACTINGNo ratings yet
- 937 PDFDocument5 pages937 PDFRavi SNo ratings yet
- Business Credit ApplicationDocument1 pageBusiness Credit ApplicationGURMUKH SINGHNo ratings yet
- Final Settlement FormDocument1 pageFinal Settlement FormNauman AmjadNo ratings yet
- Vendor Registration Form APMDocument2 pagesVendor Registration Form APMnaseefardNo ratings yet
- Adobe Scan 24 Nov 2023Document4 pagesAdobe Scan 24 Nov 2023kmahlaba23No ratings yet
- WPS Registration Booklet - Al Ansari ExchangeDocument17 pagesWPS Registration Booklet - Al Ansari Exchangeinfo.almanzoomaNo ratings yet
- Pre Qualfication VillaDocument140 pagesPre Qualfication VillaHishmat EzzelarabNo ratings yet
- Proposal For Setup of CompanyDocument2 pagesProposal For Setup of CompanyMPS AtcoNo ratings yet
- Updated Business Unlimited FormDocument7 pagesUpdated Business Unlimited FormDiane SNo ratings yet
- Trade Name Reservation ReceiptDocument1 pageTrade Name Reservation ReceiptHORUS TYPING & P.R.O SERVICESNo ratings yet
- Annex A1 - SME Packages - Service Supplement Form - Egov DirectDocument1 pageAnnex A1 - SME Packages - Service Supplement Form - Egov DirectlibraryNo ratings yet
- Certificate CR 4914532Document1 pageCertificate CR 4914532fairoosmoosaNo ratings yet
- Customer Information SheetDocument2 pagesCustomer Information SheetSouleyemane DiongueNo ratings yet
- Partnership - Contract KsaDocument9 pagesPartnership - Contract KsaMuhammad BilalNo ratings yet
- Refund Application FormDocument1 pageRefund Application FormtammymahlanguNo ratings yet
- Al Batin Advanced - Pre-QualificationDocument43 pagesAl Batin Advanced - Pre-QualificationFo MuNo ratings yet
- MIE Background Screening FormDocument1 pageMIE Background Screening FormTumi MatlouNo ratings yet
- Commercial License: No. / Owners / Partners Nationality RoleDocument1 pageCommercial License: No. / Owners / Partners Nationality Rolelimudee023No ratings yet
- Prequalification QuestionnaireDocument4 pagesPrequalification Questionnaireشاز إياسNo ratings yet
- Insurance PolicyDocument3 pagesInsurance PolicyJafar APNo ratings yet
- ALkhalidiya Water Proofing Trade License 2024 UpdateDocument1 pageALkhalidiya Water Proofing Trade License 2024 UpdatehazelNo ratings yet
- تعريف بالراتب الراجحي م.الشعراني محمد المباركDocument1 pageتعريف بالراتب الراجحي م.الشعراني محمد المباركElsharaani MohammedNo ratings yet
- CF CD CDApplicationPDFDocument9 pagesCF CD CDApplicationPDFNeena kushwahaNo ratings yet
- Canada Contract Letter Abobaker 1Document5 pagesCanada Contract Letter Abobaker 1abobaker959553No ratings yet
- Application FormDocument2 pagesApplication FormAikakamalNo ratings yet
- Handset Form - Device Installment Plan - English (Roadshows)Document3 pagesHandset Form - Device Installment Plan - English (Roadshows)faizalpsNo ratings yet
- Commercial License: No. / Owners / Partners Nationality RoleDocument2 pagesCommercial License: No. / Owners / Partners Nationality Roleزيد القدورNo ratings yet
- Payaid Agreement V1 2Document12 pagesPayaid Agreement V1 2Kanchan PatilNo ratings yet
- Personnel ManagerDocument1 pagePersonnel ManagerShafie ZubierNo ratings yet
- VAT Registration Certificate 3D CONCEPTSDocument2 pagesVAT Registration Certificate 3D CONCEPTSLahiru Supun SamaraweeraNo ratings yet
- Trade License 2019-20Document1 pageTrade License 2019-20Ayaan Vlogs and GamingNo ratings yet
- Indian HR Convention: & 15 December 2017, DelhiDocument10 pagesIndian HR Convention: & 15 December 2017, DelhiTaleesJRizviNo ratings yet
- Credit Facility ApplicationDocument2 pagesCredit Facility ApplicationRenny M PNo ratings yet
- Red Sea License 2021-2025Document1 pageRed Sea License 2021-2025irshadkhanusiyaNo ratings yet
- Contract - Nandar Win 1Document19 pagesContract - Nandar Win 1qntpyvtym8No ratings yet
- JAIBP Application PDFDocument3 pagesJAIBP Application PDFMuhammadShoaibNo ratings yet
- عقد جوال لمارDocument3 pagesعقد جوال لمارwajdi777No ratings yet
- Business Credit Application - Charly USA: Name/AddressDocument2 pagesBusiness Credit Application - Charly USA: Name/Addressjose luis anguloNo ratings yet
- Loan Application v.2Document2 pagesLoan Application v.2Jose Rico ColigadoNo ratings yet
- Business Credit Application 02Document1 pageBusiness Credit Application 02raj dosNo ratings yet
- Business Credit Application TemplateDocument1 pageBusiness Credit Application Templatemygst0108No ratings yet
- Credit Application Form 01Document1 pageCredit Application Form 01loganathan owNo ratings yet
- Alabidvisa PlatformDocument2 pagesAlabidvisa Platformma.shehlaintNo ratings yet
- 10194924179Document8 pages10194924179tsd377464No ratings yet
- Reimbursement Claim FormDocument1 pageReimbursement Claim FormmoinuNo ratings yet
- CertificateDocument1 pageCertificateKhalied RedaNo ratings yet
- Akuntansi Piutang 2215654085 22Document23 pagesAkuntansi Piutang 2215654085 22085ANANDASURYAAPNo ratings yet
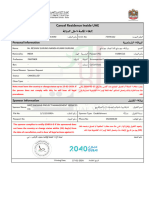
- Cancel Residence Inside UAE : Personal InformationDocument1 pageCancel Residence Inside UAE : Personal Informationworkgg247No ratings yet
- Creditor Application Form (New)Document2 pagesCreditor Application Form (New)Elaine LauNo ratings yet
- Processing Notification - Background Screening Request: Company DetailsDocument2 pagesProcessing Notification - Background Screening Request: Company DetailsmusaNo ratings yet
- Evo Merchant Application 2014Document6 pagesEvo Merchant Application 2014api-257017808No ratings yet
- ContractDocument3 pagesContractrakansalh39No ratings yet
- BusinessLicense - CN-1993103 LG DesignDocument1 pageBusinessLicense - CN-1993103 LG Designamanirfan641No ratings yet
- MIE Personal Credential Disclosure Form 2021Document1 pageMIE Personal Credential Disclosure Form 2021naledi.mantlala05No ratings yet
- MIE Consent FormDocument1 pageMIE Consent FormSibongiseni NtuliNo ratings yet
- Fit 247 Plus Training DDRDocument2 pagesFit 247 Plus Training DDRDigiwhizNo ratings yet
- Deviceinvoice 935712 1Document3 pagesDeviceinvoice 935712 1Anoop JangraNo ratings yet
- How To Structure Your Business For Success: Everything You Need To Know To Get Started Building Business CreditFrom EverandHow To Structure Your Business For Success: Everything You Need To Know To Get Started Building Business CreditNo ratings yet
- CATALOGUE Digital-Version March2021-1Document6 pagesCATALOGUE Digital-Version March2021-1Gisèle HAGNONNo ratings yet
- DocumentDocument4 pagesDocumentGisèle HAGNONNo ratings yet
- Interview Form - Couche-TardDocument2 pagesInterview Form - Couche-TardGisèle HAGNONNo ratings yet
- Eli $ 1Document2 pagesEli $ 1Gisèle HAGNONNo ratings yet
- Soutien No 11 - Calcul Litteral Developpement Et FactorisationDocument3 pagesSoutien No 11 - Calcul Litteral Developpement Et FactorisationGisèle HAGNONNo ratings yet