You might also like
- The Stigma of Mental IllnessDocument15 pagesThe Stigma of Mental IllnessJulie HechanovaNo ratings yet
- SNLE Applicant Guide 2020Document14 pagesSNLE Applicant Guide 2020Tati MaryatiNo ratings yet
- NCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsFrom EverandNCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsNo ratings yet
- Lesson plan on non-communicable diseases (NCDsDocument2 pagesLesson plan on non-communicable diseases (NCDsCherryn Dorotayo Quiminsao86% (29)
- Schizotypal Personality DisorderDocument5 pagesSchizotypal Personality DisorderFeraNovianti100% (1)
- Patient Centered CareDocument10 pagesPatient Centered CareAgatha PradanaNo ratings yet
- Objectives May Be Used To Support Student Reflection, Although The List of Indicators Is NotDocument14 pagesObjectives May Be Used To Support Student Reflection, Although The List of Indicators Is Notapi-456466614No ratings yet
- Physical Therapy Clinical Management.9 PDFDocument24 pagesPhysical Therapy Clinical Management.9 PDFClaudia MicuNo ratings yet
- DSC BookDocument52 pagesDSC BookPriti Khemka60% (5)
- NCM 109 LP RLE On HIGH RISK FOR PEDIATRIC CASE 1Document7 pagesNCM 109 LP RLE On HIGH RISK FOR PEDIATRIC CASE 1Melinda Cariño BallonNo ratings yet
- Handbook of Specialist Training in Paediatric Nephrology in MalaysiaDocument57 pagesHandbook of Specialist Training in Paediatric Nephrology in MalaysiaPICU HTJSNo ratings yet
- Competency Based Training Programme: Dnb-NeonatologyDocument62 pagesCompetency Based Training Programme: Dnb-NeonatologySonu AntonyNo ratings yet
- Paediatric and Paediatric Nursing IDocument541 pagesPaediatric and Paediatric Nursing ILUAMFULA RHC100% (1)
- Competency1. Patient Care: The Neonatal Intensive Care UnitDocument8 pagesCompetency1. Patient Care: The Neonatal Intensive Care UnitChristopher TibuleNo ratings yet
- Adherence To Long-Term Therapies Evidence of Action 1Document16 pagesAdherence To Long-Term Therapies Evidence of Action 1Anonymous so6ZnlKywNo ratings yet
- Assessing Neuromotor Readiness for Learning: The INPP Developmental Screening Test and School Intervention ProgrammeFrom EverandAssessing Neuromotor Readiness for Learning: The INPP Developmental Screening Test and School Intervention ProgrammeRating: 5 out of 5 stars5/5 (1)
- Paediatric Podiatry Clinical Framework 2019 FinalDocument23 pagesPaediatric Podiatry Clinical Framework 2019 FinalMahmoud A KhatabNo ratings yet
- Objectives May Be Used To Support Student Reflection, Although The List of Indicators Is NotDocument14 pagesObjectives May Be Used To Support Student Reflection, Although The List of Indicators Is Notapi-456466614No ratings yet
- Physical Therapy Clinical ManagementDocument24 pagesPhysical Therapy Clinical ManagementClaudia MicuNo ratings yet
- THC 123 - Risk Management As Applied To Safety, Security, and SanitationDocument94 pagesTHC 123 - Risk Management As Applied To Safety, Security, and SanitationJanry Bantiles90% (10)
- DC10637 APP Paediatric Emergency Medicine Syllabus 75637504Document22 pagesDC10637 APP Paediatric Emergency Medicine Syllabus 75637504Essam HassanNo ratings yet
- Appendix 4M - Paediatric Emergency MedicineDocument21 pagesAppendix 4M - Paediatric Emergency MedicineEssam HassanNo ratings yet
- Neonatal Guideline Quick Reference and Implementation GuideDocument12 pagesNeonatal Guideline Quick Reference and Implementation GuidepepiNo ratings yet
- Follow Up High Risk NBDocument36 pagesFollow Up High Risk NBinggrit anggrainiNo ratings yet
- Paediatric Nephrology Syllabus FinalDocument13 pagesPaediatric Nephrology Syllabus FinalClever BarbieNo ratings yet
- Progressplus Emergency Medicine Syllabus 2023Document21 pagesProgressplus Emergency Medicine Syllabus 2023dr.gergely.halaszNo ratings yet
- MD Peadiatrics NMC CURRICULUMDocument67 pagesMD Peadiatrics NMC CURRICULUMraghava mbbs100% (1)
- Guidelines For Training in Developmental and Behavioral Pediatrics 012012 1 PDFDocument5 pagesGuidelines For Training in Developmental and Behavioral Pediatrics 012012 1 PDFStarlet Rhonadez Bito-onon OrielNo ratings yet
- Foundation Doctor Resources GuideDocument4 pagesFoundation Doctor Resources GuideSarina PromthongNo ratings yet
- BSC in Neonatal NursingDocument14 pagesBSC in Neonatal NursingsmsmdsdsffNo ratings yet
- Individualized Developmental Care For High Risk NBDocument10 pagesIndividualized Developmental Care For High Risk NBLily Mtz MNo ratings yet
- Advanced paediatric training specificationDocument12 pagesAdvanced paediatric training specificationNorhafizah AhmadNo ratings yet
- Clinical Objectives PDFDocument4 pagesClinical Objectives PDFYhuhan James TejadaNo ratings yet
- Fy2 in GP Guide - April 2018 PDFDocument28 pagesFy2 in GP Guide - April 2018 PDFTirtha TaposhNo ratings yet
- 1377 FullDocument23 pages1377 FullPutri Wahyuni AllfazmyNo ratings yet
- Educational Perspectives: Educational Strategies To Improve Outcomes From Neonatal ResuscitationDocument13 pagesEducational Perspectives: Educational Strategies To Improve Outcomes From Neonatal ResuscitationDian RahmawatiNo ratings yet
- UC San Francisco Previously Published WorksDocument10 pagesUC San Francisco Previously Published WorksTessa CruzNo ratings yet
- MRCPCH Newcomer's Guide Dec 09Document12 pagesMRCPCH Newcomer's Guide Dec 09Franzil MirandaNo ratings yet
- Pediatric Nephrology Content OutlineDocument8 pagesPediatric Nephrology Content OutlineAbdifitah Husein osmanNo ratings yet
- Paediatric Guidance Checklist: Specialty: Level 1Document4 pagesPaediatric Guidance Checklist: Specialty: Level 1Snehal PatilNo ratings yet
- Guia Basada en La Evidencia Canguro 2019Document8 pagesGuia Basada en La Evidencia Canguro 2019luzhelanapaezNo ratings yet
- NAH-Nursing-Adult HealthDocument2 pagesNAH-Nursing-Adult HealthFERL KAILA SANTOSNo ratings yet
- PAPER WORKPaediatricsDocument22 pagesPAPER WORKPaediatricsIzzati OthmanNo ratings yet
- Ojsadmin, 369 PDFDocument8 pagesOjsadmin, 369 PDFNabila FirgyNo ratings yet
- NBE Guidelines High-Risk-Pregnancy-PerinatologyDocument23 pagesNBE Guidelines High-Risk-Pregnancy-PerinatologyATUL178No ratings yet
- Paediatric eLearning Certification CourseDocument11 pagesPaediatric eLearning Certification CourseNurToyibahNo ratings yet
- Obs & GynDocument121 pagesObs & GynSaya K. AkremNo ratings yet
- NZREX Bridging Programme OverviewDocument12 pagesNZREX Bridging Programme OverviewGus LionsNo ratings yet
- At AddictionMedicine CurriculaDocument37 pagesAt AddictionMedicine Curriculaastral055356No ratings yet
- Rough Guide To Curriculum - Doc - FINALDocument22 pagesRough Guide To Curriculum - Doc - FINALniki jijiNo ratings yet
- Clinical ObjectivesDocument1 pageClinical ObjectivesMuhammad AdilNo ratings yet
- NEUROLOGY SYLLABUSDocument73 pagesNEUROLOGY SYLLABUSkriskris12345No ratings yet
- Evidencias VojtaDocument9 pagesEvidencias VojtaRommel AndresNo ratings yet
- EPA 3and4 WorkbookDocument15 pagesEPA 3and4 Workbookjames.a.blairNo ratings yet
- Adult Health Nursing Course Grid - Yr II Sem IIDocument43 pagesAdult Health Nursing Course Grid - Yr II Sem IIHamayun Khan100% (2)
- ILP Acute 2007Document52 pagesILP Acute 2007Thanh HuynhNo ratings yet
- Rcpi Diploma in Paediatrics BrochureDocument4 pagesRcpi Diploma in Paediatrics Brochureanitn2020No ratings yet
- Unit Proposal PresentationDocument29 pagesUnit Proposal PresentationRachel CortezNo ratings yet
- NBNS3224 Learning KitDocument54 pagesNBNS3224 Learning KitShaa ShaamalaahNo ratings yet
- Media 194791 SMXX PDFDocument4 pagesMedia 194791 SMXX PDFMoises Eduardo Pacheco ChambiNo ratings yet
- 2022 NMC DM NeonatologyDocument30 pages2022 NMC DM NeonatologySutirtha RoyNo ratings yet
- Guideline 10 2 Advanced Life Support Als Training 231Document19 pagesGuideline 10 2 Advanced Life Support Als Training 231cknihilnewNo ratings yet
- Draft National Standards For Paediatric Critical Care Jan 2013Document16 pagesDraft National Standards For Paediatric Critical Care Jan 2013sarasNo ratings yet
- Saudi Council for Health Specialties oversees Pediatric Surgery FellowshipDocument17 pagesSaudi Council for Health Specialties oversees Pediatric Surgery FellowshipmdbahaNo ratings yet
- Under Graduate Academic Record - Department of OphthalmologyDocument123 pagesUnder Graduate Academic Record - Department of OphthalmologyRamesh BabuNo ratings yet
- Iv. National Nursing Career Progression Program: Baguio City APRIL 25, 2014Document13 pagesIv. National Nursing Career Progression Program: Baguio City APRIL 25, 2014louradelNo ratings yet
- Fitness Activity Declaration Form (Par-Q)Document1 pageFitness Activity Declaration Form (Par-Q)etbyersaol.comNo ratings yet
- School Health ServicesDocument23 pagesSchool Health ServicesNeethu Vincent50% (2)
- Reading Test - 19 Part - A: TIME: 15 MinutesDocument17 pagesReading Test - 19 Part - A: TIME: 15 MinutesKelvin KanengoniNo ratings yet
- KNGF Guideline For Physical Therapy in Patients With ParkinsDocument89 pagesKNGF Guideline For Physical Therapy in Patients With ParkinsSrđan ŠarenacNo ratings yet
- Syphilitic Miasm ExploredDocument20 pagesSyphilitic Miasm Exploredpanniyin selvanNo ratings yet
- EpidemiologyDocument61 pagesEpidemiologyPrathik RaiNo ratings yet
- Proceeding Book 28th Jakarta Diabates Meeting 2019Document19 pagesProceeding Book 28th Jakarta Diabates Meeting 2019David DwiputeraNo ratings yet
- Psychosomatic 1Document15 pagesPsychosomatic 1Jaiprakash AgrawalNo ratings yet
- Disgrasya: By: Conrado de QuirosDocument6 pagesDisgrasya: By: Conrado de QuirosEmmanuel Linguaje Managbanag IINo ratings yet
- Ben's Trevo Presentation SlideDocument69 pagesBen's Trevo Presentation SlideBenNo ratings yet
- SHIATSUDocument5 pagesSHIATSUAndrea PeriguaNo ratings yet
- S C R S C: Ymptom Lusters Elated To Pecific AncersDocument6 pagesS C R S C: Ymptom Lusters Elated To Pecific AncersDip Ayan MNo ratings yet
- MedievalDocument2 pagesMedievalGrace Marie TadeoNo ratings yet
- 9 Department of Health - Diabetes Mellitus Prevention and Control Program - 2011-12-23Document2 pages9 Department of Health - Diabetes Mellitus Prevention and Control Program - 2011-12-23Evelyn Chu Nevado67% (3)
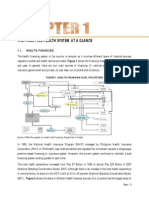
- Philippines health system overview: financing, facilities, human resourcesDocument15 pagesPhilippines health system overview: financing, facilities, human resourcesYL LYNo ratings yet
- A. Main Idea: Our Body Reacts Similarly With Our State of Mind. DetailsDocument3 pagesA. Main Idea: Our Body Reacts Similarly With Our State of Mind. DetailsNor AinaNo ratings yet
- 89-Article Text-248-3-10-20191208Document16 pages89-Article Text-248-3-10-20191208Rizal MantovaniNo ratings yet
- Boost Your Immune System in 40 WordsDocument4 pagesBoost Your Immune System in 40 WordsDemaunic DemonNo ratings yet
- TAX - SSS BenefitsDocument10 pagesTAX - SSS BenefitsGinaNo ratings yet
- Biodiversity and Human HealthDocument32 pagesBiodiversity and Human HealthMarygrace BroñolaNo ratings yet
- Advance Care Plan BlankDocument3 pagesAdvance Care Plan BlankJanine Anderson100% (1)
- Physical Assessment ToolDocument21 pagesPhysical Assessment ToolAmal LR100% (1)
- Diabetic Prevention AppDocument33 pagesDiabetic Prevention AppASLAMIA UKOMNo ratings yet
- HealthspanDocument8 pagesHealthspanAlberdiNo ratings yet