You might also like
- Case Study For Pleural-EffusionDocument10 pagesCase Study For Pleural-EffusionGabbii CincoNo ratings yet
- Clinical Neurophysiology of The Vestibular System (001-057) PDFDocument57 pagesClinical Neurophysiology of The Vestibular System (001-057) PDFAriel CarterNo ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- Sheet 4 (Bone Pathology)Document206 pagesSheet 4 (Bone Pathology)ardesh abdilleNo ratings yet
- Elderly HandbookDocument95 pagesElderly HandbookJojo ChuaNo ratings yet
- Oncology Oite Review 2012 120920125342 Phpapp02Document738 pagesOncology Oite Review 2012 120920125342 Phpapp02Stephen James100% (1)
- BoneDocument68 pagesBonedr_asaleh100% (2)
- Bone Tumors: Prepared by DR Pgr.2 Ortho Unit 3 BMCHDocument47 pagesBone Tumors: Prepared by DR Pgr.2 Ortho Unit 3 BMCHMohamed Al-zichrawyNo ratings yet
- Bone TumorDocument36 pagesBone TumorMoch NizamNo ratings yet
- Term 3 Rationale Pharmacology and MCNDocument35 pagesTerm 3 Rationale Pharmacology and MCNKing KongNo ratings yet
- Update Anesthesia 2009Document72 pagesUpdate Anesthesia 2009Oscar David Ramirez ArbelaezNo ratings yet
- Module 6 Dr. AlbertoDocument10 pagesModule 6 Dr. AlbertoJASTHER LLOYD TOMANENGNo ratings yet
- Benign Bone TumorsDocument31 pagesBenign Bone TumorsDr Afsar KhanNo ratings yet
- Bone Tumors and Tumorlike Conditions: Analysis With Conventional RadiographyDocument73 pagesBone Tumors and Tumorlike Conditions: Analysis With Conventional RadiographyViskaNo ratings yet
- BenignOsseousTumorsofBoneOsteoblastomaandOsteoid OsteDocument203 pagesBenignOsseousTumorsofBoneOsteoblastomaandOsteoid OstechikkisaurusNo ratings yet
- Bone Tumors: Osteoma, Osteosarcoma, and MoreDocument12 pagesBone Tumors: Osteoma, Osteosarcoma, and MoreAyushi GoelNo ratings yet
- DOC-20240413-WA0027.Document29 pagesDOC-20240413-WA0027.apdallahyousef11No ratings yet
- Cystak Diagnosztikája AngolDocument36 pagesCystak Diagnosztikája AngolErdeli StefaniaNo ratings yet
- DOC-20240413-WA0027.Document31 pagesDOC-20240413-WA0027.apdallahyousef11No ratings yet
- Benign Bone Tumors - AMBOSSDocument1 pageBenign Bone Tumors - AMBOSSMohammedNo ratings yet
- PathologyDocument12 pagesPathologyKetmia ZamoraNo ratings yet
- Disorders of The Bone2Document46 pagesDisorders of The Bone2AyeshaNo ratings yet
- Oral Pathology Lec6a81fe1b A65f 4c85 9e9d 4f9e299f7ba5 - 1Document10 pagesOral Pathology Lec6a81fe1b A65f 4c85 9e9d 4f9e299f7ba5 - 1مصطفى محمدNo ratings yet
- الهامDocument18 pagesالهامmoh.ahm3040No ratings yet
- 13-Benign Bone TumorsDocument18 pages13-Benign Bone Tumorsفراس الموسويNo ratings yet
- Lecture 3 MuskDocument8 pagesLecture 3 MuskElgilani zaherNo ratings yet
- Diseases of Bone & OsteodystrophiesDocument54 pagesDiseases of Bone & OsteodystrophiesShreya singhNo ratings yet
- Benign Nonodontogenic TumorsDocument20 pagesBenign Nonodontogenic TumorsEuginia YosephineNo ratings yet
- Seminar W4 - Bone & Soft Tissue TumoursDocument123 pagesSeminar W4 - Bone & Soft Tissue TumoursUN EPNo ratings yet
- jnu bone tumors - 複本Document130 pagesjnu bone tumors - 複本Wai Kwong ChiuNo ratings yet
- Disease of Bone Manifested in The JawsDocument35 pagesDisease of Bone Manifested in The Jawsyongky100% (1)
- Compare Osteosarcoma and OsteoclastomaDocument14 pagesCompare Osteosarcoma and OsteoclastomaMOHAMED AMINNo ratings yet
- Screenshot 2022-11-12 at 7.36.53 AMDocument62 pagesScreenshot 2022-11-12 at 7.36.53 AMeman.ta3labNo ratings yet
- Benign Bone TumoursDocument13 pagesBenign Bone TumoursAnisah MahmudahNo ratings yet
- Seminar 1 OrthoDocument139 pagesSeminar 1 OrthoEng Kian NgNo ratings yet
- Classification Diagnosis and Clinical Manifestatio PDFDocument20 pagesClassification Diagnosis and Clinical Manifestatio PDFdzakki saragihNo ratings yet
- Benign Odontogenic Tumou1rDocument67 pagesBenign Odontogenic Tumou1rVISHAL DHIMANNo ratings yet
- Benign Bone Tumours Lecture - PpsDocument11 pagesBenign Bone Tumours Lecture - Ppsnickmirad2No ratings yet
- Radiology Revision 2Document6 pagesRadiology Revision 2Yusnida RahmawatiNo ratings yet
- Infection of The JawDocument51 pagesInfection of The JawMutia Safitri0% (1)
- Diagnosis of Bone Tumours: 1. Age of Patient 2. Location of Tumour 3. Radiological Appearance 4. Histological FeaturesDocument69 pagesDiagnosis of Bone Tumours: 1. Age of Patient 2. Location of Tumour 3. Radiological Appearance 4. Histological FeaturesMochammad Fariz AmsalNo ratings yet
- OsteomyelitisDocument32 pagesOsteomyelitisyogeshNo ratings yet
- Benign Non-Odontogenic Tumors IIDocument1 pageBenign Non-Odontogenic Tumors IIa.ahmed4922No ratings yet
- Disorders of The Bone1Document51 pagesDisorders of The Bone1AyeshaNo ratings yet
- Patho Notes PDFDocument6 pagesPatho Notes PDFAlvin Karl ValenciaNo ratings yet
- Ohns 3 182Document8 pagesOhns 3 182kalixinNo ratings yet
- Osteomyelitis: Oral Pathology 4 Stage DR - Hemn M.Sharif (B.D.S, MSC, O.Medicine) 2-4-2020Document18 pagesOsteomyelitis: Oral Pathology 4 Stage DR - Hemn M.Sharif (B.D.S, MSC, O.Medicine) 2-4-2020محمد عبدالهادي إسماعيلNo ratings yet
- Diaphyseal AclasisDocument1 pageDiaphyseal AclasisABCNo ratings yet
- Fibro OsseousDocument25 pagesFibro OsseoussadiaNo ratings yet
- Mixed Tumors of Odontogenic Origin WordDocument31 pagesMixed Tumors of Odontogenic Origin WordAshimNo ratings yet
- 4.benign Odontogenic and Non-Odontogenic Tumors of The Jaws - SlidesDocument45 pages4.benign Odontogenic and Non-Odontogenic Tumors of The Jaws - SlidesTarlan FarhadiNo ratings yet
- OdontomasDocument4 pagesOdontomasArafat Masud Niloy100% (1)
- Fibrous Dysplasia: DR Bareerah Idrees Resident OMFS 08 May 2021Document37 pagesFibrous Dysplasia: DR Bareerah Idrees Resident OMFS 08 May 2021biaidreesNo ratings yet
- Lumps and Swellings in The Jaws: Aneurysmal Bone CystDocument4 pagesLumps and Swellings in The Jaws: Aneurysmal Bone CystGokul SivaNo ratings yet
- Oral MedicineDocument75 pagesOral MedicineAyush SoniNo ratings yet
- Benign Tumors of Epithelial and Mesenchymal Origin inDocument41 pagesBenign Tumors of Epithelial and Mesenchymal Origin inMladen PazinNo ratings yet
- Osteochondroma: Dr. Mahesh Chaudhary Phase-A Resident Radiology & Imaging BsmmuDocument36 pagesOsteochondroma: Dr. Mahesh Chaudhary Phase-A Resident Radiology & Imaging BsmmubucculuNo ratings yet
- Developmental Disorders and Skeletal ConditionsDocument33 pagesDevelopmental Disorders and Skeletal ConditionsRahul SarkarNo ratings yet
- Bones JointsDocument11 pagesBones JointszeeathrNo ratings yet
- RCSD or RCCD Peripheral WITHDocument2 pagesRCSD or RCCD Peripheral WITHEmma LiamNo ratings yet
- Odontogenic Tumors IIDocument24 pagesOdontogenic Tumors IIIbn HabibNo ratings yet
- Zebra XX, Part 2 PDFDocument3 pagesZebra XX, Part 2 PDFRamona MateiNo ratings yet
- BONE TUMOR ANALYSIS WITH X-RAYDocument73 pagesBONE TUMOR ANALYSIS WITH X-RAYAulia AlmiraNo ratings yet
- Diseases of The Bone and Soft TissuesDocument8 pagesDiseases of The Bone and Soft TissuesMarieCrisNo ratings yet
- DIFFERENTIAL DIAGNOSIS OF FIBRO-OSSEOUS LESIONDocument66 pagesDIFFERENTIAL DIAGNOSIS OF FIBRO-OSSEOUS LESIONBhupinder KaushalNo ratings yet
- Disfagia JPGN 2023Document8 pagesDisfagia JPGN 2023monicarodriguezsalas82No ratings yet
- Predictive Homeopathy Course Review, Part I: Susanne Saltzman, MDDocument5 pagesPredictive Homeopathy Course Review, Part I: Susanne Saltzman, MDdr TotoNo ratings yet
- Assignmen 1 AnswersDocument3 pagesAssignmen 1 AnswersAlasl BobyNo ratings yet
- Clarithromycin: Navigation SearchDocument15 pagesClarithromycin: Navigation SearchMayank ShankhwarNo ratings yet
- Clinical Case Report of Upper GI BleedDocument44 pagesClinical Case Report of Upper GI Bleedjoanna fitzmorrisNo ratings yet
- Rough Draft Coffee ConsumptionDocument5 pagesRough Draft Coffee ConsumptionMariana Cedeño RamosNo ratings yet
- (CC) Case Study 1 and 2Document11 pages(CC) Case Study 1 and 2Alyssa Nicole BarrettoNo ratings yet
- Wu Et Al. - 2013 - Phenytoin A Guide To Therapeutic Drug MonitoringDocument5 pagesWu Et Al. - 2013 - Phenytoin A Guide To Therapeutic Drug MonitoringfachriybalafifNo ratings yet
- A Case Report of Aphallia With Urorectal Septum Malformation Sequence in A Newborn: A Very Rarely Seen ConditionDocument4 pagesA Case Report of Aphallia With Urorectal Septum Malformation Sequence in A Newborn: A Very Rarely Seen ConditionRon Java FantillanNo ratings yet
- Surgical Treatment of Severe LaryngomalaciaDocument7 pagesSurgical Treatment of Severe LaryngomalaciaPutri HakimNo ratings yet
- Drug Study Mechanism of Action Indication/ Contraindication Adverse Effects Nursing Responsibilities Generic Name: Indication: Before: DuringDocument1 pageDrug Study Mechanism of Action Indication/ Contraindication Adverse Effects Nursing Responsibilities Generic Name: Indication: Before: DuringAubrie StellarNo ratings yet
- Brain DeathDocument6 pagesBrain DeathmohamedelsayedelmenyawyNo ratings yet
- A Chronic Obstructive Pulmonary Disease (COPD) Patient Case Scenario - EditedDocument4 pagesA Chronic Obstructive Pulmonary Disease (COPD) Patient Case Scenario - Editedbenson gathuaNo ratings yet
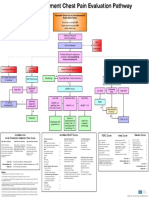
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Pocket guide for antimicrobial use in horsesDocument4 pagesPocket guide for antimicrobial use in horsesMd NoumanNo ratings yet
- Marjo S. Van Der Knaap MD, PHD, Jacob Valk MD, PHD Auth. Magnetic Resonance of Myelin, Myelination, and Myelin DisordersDocument570 pagesMarjo S. Van Der Knaap MD, PHD, Jacob Valk MD, PHD Auth. Magnetic Resonance of Myelin, Myelination, and Myelin Disordersali tidaNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument4 pagesAnnals of Medicine and Surgery: SciencedirectLee제노No ratings yet
- Kode Icd 10 Isna TerbaruDocument43 pagesKode Icd 10 Isna Terbarulisna ginawatiNo ratings yet
- Lecturer of Neurology Mansoura Faculty of Medicine: Ashraf El-Mitwalli, MDDocument122 pagesLecturer of Neurology Mansoura Faculty of Medicine: Ashraf El-Mitwalli, MDCarolina TulanNo ratings yet
- Covid19-Drug StudyDocument7 pagesCovid19-Drug StudynicoleNo ratings yet
- BS Nursing Program OutcomesDocument20 pagesBS Nursing Program Outcomesۦۦ JamesNo ratings yet
- Detection of Pulmonary Blastomycosis Using Conventional and Molecular MethodsDocument13 pagesDetection of Pulmonary Blastomycosis Using Conventional and Molecular MethodsIkha UdmalasariNo ratings yet
- MDS-6-Mock-exam-QAE - Unlocked FINALDocument70 pagesMDS-6-Mock-exam-QAE - Unlocked FINALSubhashNo ratings yet
- Pathophysiology of AllDocument1 pagePathophysiology of AllBGHMC PEDIAHONo ratings yet
- Down's Syndrome GP GuideDocument6 pagesDown's Syndrome GP GuideElison J PanggaloNo ratings yet