You might also like
- Primary Care Case Studies for Nurse PractitionersFrom EverandPrimary Care Case Studies for Nurse PractitionersRating: 5 out of 5 stars5/5 (3)
- Hyposkillia: Guest EditorialDocument3 pagesHyposkillia: Guest EditorialRenan BragaNo ratings yet
- HYPOSKILIADocument2 pagesHYPOSKILIAMohammad Abid100% (1)
- 1 Delivering Bad NewsDocument11 pages1 Delivering Bad NewsLo peña moNo ratings yet
- NFDN 2005Document2 pagesNFDN 2005api-302133133No ratings yet
- Bedside Teaching of Medical StudentsDocument2 pagesBedside Teaching of Medical StudentsRafi Ullah HaleemNo ratings yet
- Propedeutik 2 3 Dental FacultyDocument214 pagesPropedeutik 2 3 Dental FacultyVimal SuseeNo ratings yet
- Geriatric Syndromes: How To Treat: ReviewDocument9 pagesGeriatric Syndromes: How To Treat: ReviewAdrian TambunNo ratings yet
- Murtaghs Patient EducationDocument3 pagesMurtaghs Patient Educationrohancomet100100% (1)
- Medu 13934Document12 pagesMedu 13934erine5995No ratings yet
- 31200753: Sepsis Personalization V ProtocolizationDocument6 pages31200753: Sepsis Personalization V ProtocolizationLuis Enrique Caceres AlavrezNo ratings yet
- Clinical Teaching 101 For Web 2014Document56 pagesClinical Teaching 101 For Web 2014Talari JyothiNo ratings yet
- Research Paper On DeliriumDocument8 pagesResearch Paper On Deliriumhyzypif0gif3100% (1)
- MKs Internal MedicineDocument995 pagesMKs Internal Medicinejhqmpzg7sjNo ratings yet
- 2017 Embracing Uncertainty To Advance Diagnosis inDocument2 pages2017 Embracing Uncertainty To Advance Diagnosis inpainfree888No ratings yet
- Murtagh S Patient EducationDocument3 pagesMurtagh S Patient EducationMAYNo ratings yet
- Clinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentDocument18 pagesClinical Decision Making in The ICU Dysphagia Screening Assesment and TreatmentΜαρία ΧανιωτάκηNo ratings yet
- Sepsis y Choque Sep Reconocimiento Temprano y Tto de Emergencia ING BuenoDocument8 pagesSepsis y Choque Sep Reconocimiento Temprano y Tto de Emergencia ING BuenoNayra Nieves Sanchez AyalaNo ratings yet
- 1 MeuDocument3 pages1 MeuAnonymous iEGRcEp2VjNo ratings yet
- Blueprint For UG Students For Working On Case ReportsDocument4 pagesBlueprint For UG Students For Working On Case ReportsNeeta KocharNo ratings yet
- Annals of Delirium October 2012Document7 pagesAnnals of Delirium October 2012tony_jameson-allenNo ratings yet
- Bedell 04 Words That HarmDocument4 pagesBedell 04 Words That HarmR.L. BandaNo ratings yet
- Primer of EpiDocument26 pagesPrimer of EpiRaywat DeonandanNo ratings yet
- Research Paper DementiaDocument8 pagesResearch Paper Dementiaaflbqtfvh100% (1)
- The Developing Physician - Becoming A Professional: Review ArticleDocument6 pagesThe Developing Physician - Becoming A Professional: Review ArticleLinda MaylianaNo ratings yet
- Cognitive Bias in Clinical MedicineDocument8 pagesCognitive Bias in Clinical MedicineRajuNo ratings yet
- Seminar For Educators: Teaching at The BedsideDocument4 pagesSeminar For Educators: Teaching at The Bedsidestarskyhutch0000No ratings yet
- Compiled Osce - R&C IIDocument73 pagesCompiled Osce - R&C IIFaisal MakkiNo ratings yet
- Peabody ParadoxDocument5 pagesPeabody ParadoxmorjdanaNo ratings yet
- Caring For Elderly Patients With Dementia Nursing PDFDocument11 pagesCaring For Elderly Patients With Dementia Nursing PDFAhmed MasoudNo ratings yet
- Caring For Elderly Patients With Dementia Nursing PDFDocument11 pagesCaring For Elderly Patients With Dementia Nursing PDFElla OrtizNo ratings yet
- Strategies To Promote Clinical Diagnostic Reasoning PDFDocument9 pagesStrategies To Promote Clinical Diagnostic Reasoning PDFflavia0% (1)
- Delivering Bad News ArticleDocument22 pagesDelivering Bad News ArticleNguyễn Hoàng Hương LyNo ratings yet
- Attitude Is A Little Thing That Makes A Big DifferenceDocument12 pagesAttitude Is A Little Thing That Makes A Big DifferenceKeyser Dagiw-aNo ratings yet
- BMJ Present Clinical CasesDocument4 pagesBMJ Present Clinical CasesmehdNo ratings yet
- Do Not Copy: Diagnosis and Management of Allergic Conjunctivitis in Pediatric PatientsDocument12 pagesDo Not Copy: Diagnosis and Management of Allergic Conjunctivitis in Pediatric PatientsAngel LimNo ratings yet
- Journal ReadingDocument3 pagesJournal ReadingRachelle Anne LetranNo ratings yet
- Depression in Medical Students Current InsightsDocument11 pagesDepression in Medical Students Current InsightsKoas HAYUU 2022No ratings yet
- Activity 3 - BoloyDocument3 pagesActivity 3 - BoloyAngelica BernalesNo ratings yet
- Professional DevelopmentDocument31 pagesProfessional DevelopmentLharra Cagulada-PostranoNo ratings yet
- NatureDP 2020 DeliriumDocument26 pagesNatureDP 2020 DeliriumPaloma GBNo ratings yet
- Nurs 3021 - Midterm Evaluation - AkDocument9 pagesNurs 3021 - Midterm Evaluation - Akapi-240864098No ratings yet
- Update-35 Teaching Clin Environ WFSA D 21 0004-FinalDocument5 pagesUpdate-35 Teaching Clin Environ WFSA D 21 0004-Finalhastings mwabaNo ratings yet
- Final Evaluation: NURS 3021H Clinical Practice Focused On Chronic Disease ManagementDocument14 pagesFinal Evaluation: NURS 3021H Clinical Practice Focused On Chronic Disease Managementapi-271855323No ratings yet
- Use of Antimicrobials at The End of LifeDocument10 pagesUse of Antimicrobials at The End of Lifeeddy puquio chavezNo ratings yet
- Brief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk InfantsDocument34 pagesBrief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk InfantsCarlos CuadrosNo ratings yet
- Ethical and Professional Conduct of Medical Students: Review of Current Assessment Measures and ControversiesDocument6 pagesEthical and Professional Conduct of Medical Students: Review of Current Assessment Measures and ControversieslamyaaNo ratings yet
- "Comorbidity or MultimorbidityDocument3 pages"Comorbidity or MultimorbidityRuben ValenteNo ratings yet
- Course Guide: Year 3Document52 pagesCourse Guide: Year 3Elise ChuaNo ratings yet
- College of Nursing Allied Health SciencesDocument38 pagesCollege of Nursing Allied Health SciencesLemuel GuevarraNo ratings yet
- Evaluation of Neck MassDocument17 pagesEvaluation of Neck MassMuammar Aqib MuftiNo ratings yet
- Educational Strategies To Promote Clinical Diagnostic Reasoning. N Engl J Med. 2006Document13 pagesEducational Strategies To Promote Clinical Diagnostic Reasoning. N Engl J Med. 2006Julio CidNo ratings yet
- HascvdDocument92 pagesHascvdbatangas_ynad_29900% (1)
- Nursing Dissertation SepsisDocument4 pagesNursing Dissertation SepsisPaperHelpWritingCanada100% (1)
- MedicineDocument4 pagesMedicineالهاشميNo ratings yet
- Multiple Sclerosis Diagnosis and The Management ofDocument8 pagesMultiple Sclerosis Diagnosis and The Management ofScafNo ratings yet
- A New Leadership Curriculum: The Multiplication of IntelligenceDocument4 pagesA New Leadership Curriculum: The Multiplication of IntelligenceGisele PhaloNo ratings yet
- The Role of Evidence Based Medicine As A Complementary Tool in The Medical PracticeDocument9 pagesThe Role of Evidence Based Medicine As A Complementary Tool in The Medical PracticeBruna LatrônicoNo ratings yet
- Carte SemioDocument279 pagesCarte SemioJoão Vitor LacerdaNo ratings yet
- Shazia Kazi UpdatedDocument4 pagesShazia Kazi Updatedshazia kazi100% (1)
- Elc.121.reading Task Question - Dec.2017 Set 1Document9 pagesElc.121.reading Task Question - Dec.2017 Set 1AHMAD MUKHRIZ ROSMINo ratings yet
- Bacteria Viruses Lesson PlanDocument7 pagesBacteria Viruses Lesson Planapi-665322772No ratings yet
- Tutorial Skin Pekan 4 Kelompok 15 Blok Skin FixedDocument17 pagesTutorial Skin Pekan 4 Kelompok 15 Blok Skin Fixedkiki tuanaya1No ratings yet
- Identification of Basic Patterns - Skin - Peri-Infundibulitis and PerifolliculitisDocument24 pagesIdentification of Basic Patterns - Skin - Peri-Infundibulitis and PerifolliculitisBogdan CarabasNo ratings yet
- Impacto PS Del Cancer Apoyo FamiliarDocument22 pagesImpacto PS Del Cancer Apoyo FamiliarNAYELY YAZMIN DORITA SANCHEZ CASTREJONNo ratings yet
- A Case Report: Hypersensitivity Reaction To DrugsDocument5 pagesA Case Report: Hypersensitivity Reaction To DrugsGNNo ratings yet
- Avmed Quiz 2Document3 pagesAvmed Quiz 2Mulyantara MPNo ratings yet
- Nutrition LectureDocument30 pagesNutrition LectureJovelle Sto.domingoNo ratings yet
- Resumen Article IcDocument4 pagesResumen Article Icapi-689165620No ratings yet
- What Is Physiatry 2022Document2 pagesWhat Is Physiatry 2022Victoria GonzalezNo ratings yet
- The New FIGO StagingDocument4 pagesThe New FIGO StagingDr.MohanNo ratings yet
- Menopause and HRTDocument35 pagesMenopause and HRTMelNo ratings yet
- Chapter 5 ExercisesDocument10 pagesChapter 5 Exercisesshafilcr07No ratings yet
- Pil 2425Document6 pagesPil 2425Gabriela ChiritoiuNo ratings yet
- Ncbi Ascorbic AcidDocument7 pagesNcbi Ascorbic AcidOsunlola GabrielNo ratings yet
- 2.orthognathic Surgery - Lower JawDocument4 pages2.orthognathic Surgery - Lower JawPaul MathaiNo ratings yet
- CS Form 86 Physical and Medical Health and RecordDocument1 pageCS Form 86 Physical and Medical Health and RecordHONEY JADE OMAROLNo ratings yet
- Pharmacology of Free RadicalsDocument27 pagesPharmacology of Free RadicalsRavi DhimanNo ratings yet
- Neurosis VS PsychosisDocument1 pageNeurosis VS Psychosissisiner09 DascăluNo ratings yet
- The Mental HealthDocument3 pagesThe Mental HealthDency Mae AbreNo ratings yet
- Pediatrics QuestionsDocument22 pagesPediatrics QuestionsShaik AmreenNo ratings yet
- Perry2008 2Document12 pagesPerry2008 2luis castroNo ratings yet
- HCC Case 2 PresentationDocument25 pagesHCC Case 2 Presentationdamion clarkeNo ratings yet
- Pharmacology Assessment No.9 Drug InformationDocument2 pagesPharmacology Assessment No.9 Drug InformationJoy GarciaNo ratings yet
- Connect Core Concepts in Health Big 14th Edition Insel Test BankDocument30 pagesConnect Core Concepts in Health Big 14th Edition Insel Test Banktylerayalaardbgfjzym100% (33)
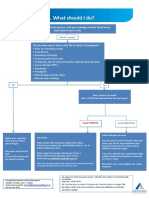
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Day 1. Mohd Sami 1Document67 pagesDay 1. Mohd Sami 1Baebee LouNo ratings yet
- 2023 CC Full WorkbookDocument988 pages2023 CC Full WorkbookZahra Ahmed AlzaherNo ratings yet
- Protocol SIOP 2001Document171 pagesProtocol SIOP 2001Omar Bendriss AlamiNo ratings yet