You might also like
- Implant Treatment 1Document1 pageImplant Treatment 1Hussien A. Abu OlbaNo ratings yet
- To Implant Treatment 1Document1 pageTo Implant Treatment 1Hussien A. Abu OlbaNo ratings yet
- Contraindications To Implant Treatment 1Document1 pageContraindications To Implant Treatment 1Hussien A. Abu OlbaNo ratings yet
- Management of Completely Edentulous MaxillaryDocument4 pagesManagement of Completely Edentulous MaxillaryDeasireeNo ratings yet
- Preprosthetic Surgery 1Document10 pagesPreprosthetic Surgery 1وليد خالدNo ratings yet
- Lecture 5Document53 pagesLecture 5Haneen Al-HajjNo ratings yet
- Os SEO IntegrationDocument7 pagesOs SEO IntegrationAkshay GajakoshNo ratings yet
- The Role of Diagnosis and Treatment LanningDocument4 pagesThe Role of Diagnosis and Treatment Lanningpasser byNo ratings yet
- Occlusal Splint (Autosaved)Document69 pagesOcclusal Splint (Autosaved)Hatem Ibrahim Ahmed AburiaNo ratings yet
- Tissue ManagementDocument16 pagesTissue ManagementSaleh AlsadiNo ratings yet
- Distraction OsteogenesisDocument30 pagesDistraction OsteogenesisMohd ZahiNo ratings yet
- Contemporary Implant Dentistry: Chapter 14 of Contemporary Oral and Maxillofacial Surgery By: DrarashkhojastehDocument65 pagesContemporary Implant Dentistry: Chapter 14 of Contemporary Oral and Maxillofacial Surgery By: DrarashkhojastehRawa Omar100% (1)
- Vdocuments - MX Dental Implant 592632ae09497Document27 pagesVdocuments - MX Dental Implant 592632ae09497ZaraNo ratings yet
- Horizontal Ridge Augmentation Using Particulate BoneDocument12 pagesHorizontal Ridge Augmentation Using Particulate Bonecmfvaldesr7No ratings yet
- Preprosthetic Surgery MADE EASYDocument14 pagesPreprosthetic Surgery MADE EASYMohammedNo ratings yet
- Scopus 3Document5 pagesScopus 3Shinta rahma MansyurNo ratings yet
- Soft Tissues Remodeling Technique As A N PDFDocument12 pagesSoft Tissues Remodeling Technique As A N PDFjorgeNo ratings yet
- Zygoma ImplantDocument63 pagesZygoma ImplantKristina Robles100% (2)
- Articulo en Inglés 2Document8 pagesArticulo en Inglés 2Luis Ramirez BenaventeNo ratings yet
- Doc. en IngleesDocument6 pagesDoc. en IngleesLina MoralesNo ratings yet
- Reconstrução de Severa Reabsorção Maxilar Com Distração OsteogenicaDocument7 pagesReconstrução de Severa Reabsorção Maxilar Com Distração OsteogenicaNelson UzunNo ratings yet
- Uided Tissue RegenerationDocument22 pagesUided Tissue RegenerationFarheen FatimaNo ratings yet
- 1 s2.0 S0011853222001604 MainDocument20 pages1 s2.0 S0011853222001604 MainDANTE DELEGUERYNo ratings yet
- Direct Maxillary Sinus Lift For Single Tooth Implant A Clinical StudyDocument4 pagesDirect Maxillary Sinus Lift For Single Tooth Implant A Clinical StudyRadita Dwihaning PutriNo ratings yet
- Tissue Preservation and Maintenance of Optimum Esthetics: A Clinical ReportDocument7 pagesTissue Preservation and Maintenance of Optimum Esthetics: A Clinical ReportBagis Emre GulNo ratings yet
- Alveolar Ridge AugmentationDocument23 pagesAlveolar Ridge AugmentationA ZNo ratings yet
- 1 s2.0 S0011853220300823 MainDocument11 pages1 s2.0 S0011853220300823 Mainctbmfhcpf3No ratings yet
- Case SeriesDocument7 pagesCase Seriesemi_alaNo ratings yet
- Prosthodontic Rehabilitation of A Patient With Maxillary Flabby Ridge - A Case ReportDocument4 pagesProsthodontic Rehabilitation of A Patient With Maxillary Flabby Ridge - A Case ReportdedeNo ratings yet
- Aoi Delhi 2010 Final 2Document54 pagesAoi Delhi 2010 Final 2dean qpNo ratings yet
- Koutouzisetal 2013IJOMIAbutmentdisconnectionClinicalDocument8 pagesKoutouzisetal 2013IJOMIAbutmentdisconnectionClinicalKyoko CPNo ratings yet
- Complications of Exodontics: Mary Cris P EstandarteDocument49 pagesComplications of Exodontics: Mary Cris P EstandarteRealyn D. BerderaNo ratings yet
- Bone Ring 1Document6 pagesBone Ring 1Pradusha RevuruNo ratings yet
- SplitDocument10 pagesSplitSusan Mallqui De la Cruz100% (1)
- Three-Dimensional Vertical Alveolar Ridge Augmentation in The Posterior Maxilla: A 10-Year Clinical StudyDocument10 pagesThree-Dimensional Vertical Alveolar Ridge Augmentation in The Posterior Maxilla: A 10-Year Clinical StudyFabian Sanabria100% (1)
- Dental Implant Placement and Loading Protocols: BY Prof. Dr. Osama BarakaDocument25 pagesDental Implant Placement and Loading Protocols: BY Prof. Dr. Osama BarakaEsmail Ahmed100% (1)
- Experimental Alveolar Ridge Augmentation by Distraction Osteogenesis Using A Simple Device That Permits Secondary Implant PlacementDocument8 pagesExperimental Alveolar Ridge Augmentation by Distraction Osteogenesis Using A Simple Device That Permits Secondary Implant PlacementBagis Emre GulNo ratings yet
- Advanced Surgical TechniquesDocument25 pagesAdvanced Surgical TechniquesHaneen Al-HajjNo ratings yet
- Aaid Joi D 12 00028Document9 pagesAaid Joi D 12 00028NancyLiaoNo ratings yet
- Twelve-Month Evaluation of A Novel Mineral-Organic Adhesive Material Used To Stabilize Dental Implants Placed in Oversized Osteotomies in Vivo in An Animal ModelDocument14 pagesTwelve-Month Evaluation of A Novel Mineral-Organic Adhesive Material Used To Stabilize Dental Implants Placed in Oversized Osteotomies in Vivo in An Animal ModelAlan PollackNo ratings yet
- Generic Root FormDocument9 pagesGeneric Root FormLAKSHMI ARORANo ratings yet
- Immediate Vs Delayed Implant PlacementDocument60 pagesImmediate Vs Delayed Implant PlacementYashica KalyaniNo ratings yet
- LectureDocument8 pagesLectureMohamedAtefNo ratings yet
- Immedite Placement Makkahnew PDFDocument30 pagesImmedite Placement Makkahnew PDFaymanNo ratings yet
- Block Bone Grafts: Guided by DR Athiban I Presented by Yogitha K SriherDocument39 pagesBlock Bone Grafts: Guided by DR Athiban I Presented by Yogitha K SriherArun Thathi100% (1)
- Periodontal RegenerationDocument140 pagesPeriodontal Regenerationhtetmyat553419No ratings yet
- AJDSM Volume 22 Issue 3 Pages 247-251Document5 pagesAJDSM Volume 22 Issue 3 Pages 247-251MarisbebelaNo ratings yet
- Preprosthetic SurgeryDocument4 pagesPreprosthetic SurgeryVero AngelNo ratings yet
- Optimal Methods For Preparation and Immunostaining of Iris, Ciliary Body, and Choroidal WholemountsDocument6 pagesOptimal Methods For Preparation and Immunostaining of Iris, Ciliary Body, and Choroidal WholemountsIlalang GurunNo ratings yet
- Alveolar Ridge PreservationDocument15 pagesAlveolar Ridge PreservationSaman MohammadzadehNo ratings yet
- Australian Dental Journal - 2018 - Spencer - Implant Based Rehabilitation Options For The Atrophic Edentulous JawDocument8 pagesAustralian Dental Journal - 2018 - Spencer - Implant Based Rehabilitation Options For The Atrophic Edentulous JawAswathi RaghuthamanNo ratings yet
- Research Article: Osseointegrated Transcutaneous Device For Amputees: A Pilot Large Animal ModelDocument10 pagesResearch Article: Osseointegrated Transcutaneous Device For Amputees: A Pilot Large Animal Modelpoorva shahNo ratings yet
- Pre Prosthetic SurgeryDocument35 pagesPre Prosthetic SurgerydrkodatiNo ratings yet
- Pre Prosthetic Surgery Lec. 9&10Document7 pagesPre Prosthetic Surgery Lec. 9&10Hassan BotaniNo ratings yet
- Pre-Prosthetic SurgeryDocument5 pagesPre-Prosthetic SurgeryŽäíñäb ÄljaÑabìNo ratings yet
- Materials: A Modified Ridge Splitting Technique Using Autogenous Bone Blocks-A Case SeriesDocument10 pagesMaterials: A Modified Ridge Splitting Technique Using Autogenous Bone Blocks-A Case SeriesLouis HutahaeanNo ratings yet
- Distraction Osteogenesis SeminarDocument126 pagesDistraction Osteogenesis SeminarkeerthanNo ratings yet
- Maxillary Sinus AugmentationDocument67 pagesMaxillary Sinus Augmentationahmed bisoNo ratings yet
- Corrective Phase of Periodontal Therapy (Surgical Phase)Document12 pagesCorrective Phase of Periodontal Therapy (Surgical Phase)Hassan MohamedNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Cannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientDocument7 pagesCannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientCTV CalgaryNo ratings yet
- Psychological Communication Barriers PosterDocument1 pagePsychological Communication Barriers PostereliyaziyaNo ratings yet
- Aliza Updated ResumeDocument2 pagesAliza Updated Resumeapi-359939852No ratings yet
- Comparing and Contrasting Lady Macbeth and Ophelia From HamletDocument5 pagesComparing and Contrasting Lady Macbeth and Ophelia From HamletYashika MalhotraNo ratings yet
- Telescopic Handler Student ManualDocument41 pagesTelescopic Handler Student ManualingcalderonNo ratings yet
- Data Legacy InsuranceCos SourceRSDocument48 pagesData Legacy InsuranceCos SourceRSrishu1527No ratings yet
- Microbial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Document7 pagesMicrobial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Jai MurugeshNo ratings yet
- Dental Informatics PlusDocument1 pageDental Informatics PlusNagendra TyagiNo ratings yet
- Whitesboro Isd - 1995 TEXAS SCHOOL SURVEY OF DRUG AND ALCOHOL USEDocument6 pagesWhitesboro Isd - 1995 TEXAS SCHOOL SURVEY OF DRUG AND ALCOHOL USETexas School Survey of Drug and Alcohol UseNo ratings yet
- Bromine Water - Saturated MSDS: Section 1: Chemical Product and Company IdentificationDocument5 pagesBromine Water - Saturated MSDS: Section 1: Chemical Product and Company IdentificationWinonaNo ratings yet
- Pengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseDocument9 pagesPengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseTjatur SurantullohNo ratings yet
- Gases Toxicos Irritantes PDFDocument6 pagesGases Toxicos Irritantes PDFLUIS ANDRES JUAREZ CALLENo ratings yet
- Acetic AnhydrideDocument8 pagesAcetic AnhydrideAsyraf SabriNo ratings yet
- Neurobic Excersise Impact On Cognative FunctionDocument8 pagesNeurobic Excersise Impact On Cognative FunctionZalinah Mohd YusofNo ratings yet
- Peri Quiz Board 219Document2 pagesPeri Quiz Board 219Melody Barredo50% (2)
- (S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFDocument8 pages(S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFVenom VerdinNo ratings yet
- Wastemanagement 161028065024Document80 pagesWastemanagement 161028065024Atharva MansabdarNo ratings yet
- Responsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFDocument64 pagesResponsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFPyae PyaeNo ratings yet
- MAPEH Activity Sheet Q2-Week1Document7 pagesMAPEH Activity Sheet Q2-Week1John King johnking.monderinNo ratings yet
- PMDC Community Medicine Mcqs PDFDocument280 pagesPMDC Community Medicine Mcqs PDFJay KNo ratings yet
- Bajaj Allianz General Insurance Company LTD.: Declaration by The InsuredDocument1 pageBajaj Allianz General Insurance Company LTD.: Declaration by The InsuredArtiNo ratings yet
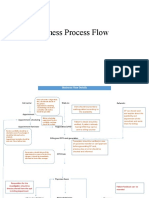
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- Policy That Implemented in Kota SamarahanDocument9 pagesPolicy That Implemented in Kota SamarahanIskandar IskandarNo ratings yet
- Direct Black 22Document4 pagesDirect Black 22DHRUVNo ratings yet
- Are You Planning To Buy or Rent A Home Built Before 1978?Document60 pagesAre You Planning To Buy or Rent A Home Built Before 1978?Maria FloresNo ratings yet
- Curriculum Vitae - Aditya Pratama PutraDocument3 pagesCurriculum Vitae - Aditya Pratama PutraIan SeptiantoNo ratings yet
- Minimizing The Risk of Alzheimer S DiseaseDocument328 pagesMinimizing The Risk of Alzheimer S DiseaseLuis Raudales100% (1)
- BioassayDocument38 pagesBioassayMuhammad Masoom AkhtarNo ratings yet
- Sugar Free Shopping ListDocument4 pagesSugar Free Shopping Listhsquiers100% (3)
- Class XII Syllabus PDFDocument60 pagesClass XII Syllabus PDFAman SinghNo ratings yet