Volume 8, Issue 5, May – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
An Interventional Prospective Study of Combined
Steroid and Lignocaine Injection for Tennis Elbow
Dr. Shubhranshu Choudhary*, Dr. Altaf Ahmad Kawoosa
Department of Orthopaedics, Government Medical College, Srinagar, Jammu & Kashmir
Abstract:- epicondyle, elevated substance P receptor levels, and
elevated glutamate levels have all been suggested as
Background potential sources of pain.[4,5,6,7,8] Nevertheless, steroid
Tennis elbow, also known as lateral epicondylitis, is injections only provide temporary symptom alleviation, and
a persistent painful condition that frequently responds after a year, the results are no better or worse than those of
poorly to traditional treatment. In tennis elbow cases, we waiting it out or receiving physiotherapy.[9,10] Through the
assessed the advantages of a steroid and lignocaine application of inflammatory cells to the affected area,
injection given together. several therapeutic approaches are suggested to promote the
repair of the sick tendon. A study on extracorporeal
Materials and Methods: shockwave (ECSW) therapy showed that it can significantly
In our prospective, interventional trial, we reduce pain in people as well as induce an inflammatory
recruited patients with lateral epicondylitis who were response in rabbit tendons.[11,12,13] Both platelet-rich
resistant to analgesics and physical treatment. A visual plasma and autologous blood injections have been
analog scale (VAS) was used to measure pain, and investigated as interventions to provide inflammatory
patients with a baseline VAS of >4 were included. By mediators to initiate a healing cascade, and both methods
using the peppering approach, triamcinolone 40mg (1ml) have been demonstrated to reduce patient discomfort.[14,15]
and lignocaine 2% (1ml) were applied locally to each We are aware of no prior evaluations of combination steroid
patient's sore area. The change in VAS from the baseline and anaesthetic drugs. We, therefore, conducted this
at 7 and 42 days was the primary result. Depending on experiment to evaluate the response of local infiltration of
whether the VAS score has decreased by 3, 2, or 1, steroids and lidocaine in lateral epicondylitis.
respectively, the improvement is categorized as good,
moderate, or mild. The data were analyzed using II. MATERIAL AND METHODS
descriptive statistics and applicable tests.
Study Setting
Results: Between January 2022 and December 2022, the
The study population (n = 48; male: female 27:21) Department of Orthopaedics at Government Medical
was 37.4 ± 8.3 years and the duration of illness was 17.9 College, Srinagar, undertook this prospective, interventional
± 4.2 weeks. In the first week, 40 patients showed good study. Patients with tennis elbow who were older than 20
improvement, 4 showed moderate improvement, 2 years old, had the condition for longer than four months, and
showed mild improvement, and 2 did not show any had a VAS baseline pain level greater than four were
improvement. The improvement persisted till 42 days in included in the study. Patients who had experienced
all the patients. localized trauma, neoplastic lesions, or previous local
steroid injection therapy were all disqualified. Every patient
Conclusion: underwent a VAS on a scale of 0 to 10, and those who had a
The local infiltrations of steroids and lignocaine score of at least 4 were included in the study. The change in
positively impacted the tennis elbow. VAS at the conclusion of 7 and 42 days was our study's
main finding. Within 42 days, no patient in our research
I. INTRODUCTION received a second injection. Prior to receiving parenteral
therapy, all patients provided written informed permission
Tennis elbow, also known as lateral epicondylitis, is a that was authorized by the local ethical committee.
severe rheumatic disease that has a high morbidity rate in its
victims. One of the most prevalent painful illnesses that Study Interventions
family doctors see in clinical practice is this one [1]. Though Triamcinolone 40 mg and lignocaine 2% were
virtually little is known about its natural history, it is topically administered to the patient's tendon location. In
associated with overusing the forearm extensor tendons.[2] order to generate the greatest amount of effective local
Tenderness at the epicondyle is a symptom of the condition. infiltration, the peppering technique was adopted, in which
The pathophysiological underpinnings, which include the numerous injections were administered at the most painful
degenerative process, damage, inflammation, and healing part of the elbow after changing directions.[16] After the
mechanisms, iarepoorly understood.[3] Free nerve endings procedure, the patient underwent a 60-minute observation
in the aponeurosis, granulation tissue around the lateral period before being allowed to leave the hospital. To
IJISRT23MAY2623 www.ijisrt.com 3124
Volume 8, Issue 5, May – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
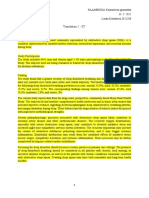
minimize personal differences in injection technique, one Fig 1: improvement at the 7 and 42nd day
th
researcher performed a tendon infiltration procedure. We
kept a watchful eye out for any systemic side effects, V. DISCUSSION
especially fainting and dizziness. All patients received oral
NSAIDS for 72 hours following the treatment and were Our study showed that combination therapy was
instructed to utilize an elbow brace and rest their elbow. effective in treating lateral epicondylitis, one of the most
Based on how much the VAS score had changed, the degree perplexing musculoskeletal conditions. In the first week
of pain improvement was assessed. 3 was considered a good following injection, the majority of patients displayed
reduction, 2 was considered moderate, and 1 was considered improvement, which lasted for 6 weeks. Previous research
a slight improvement. If the VAS score did not change from demonstrated that corticosteroid injections provided
the starting point or indicated an increase in severity, there effective pain relief but also had a significant recurrence
was a lack of progress. rate. [17,18] We demonstrated a decrease in relapse utilizing
a combination of an anaesthetic drug and a corticosteroid in
III. STATISTICS the sparse follow-up data of our trial. After a local injection,
steroids provide good pain relief, which leads to misuse of
A signed Wilcoxon rank, a non-parametric test was the arm.[19] In actuality, this is one of the primary causes of
used to compare the data before and after the intervention. the increased rates of recurrence after steroid use.[20] Thus,
Data are reported as mean standard deviation. IBM SPSS all patients are advised to rest the arm in a sling at least for
Statistics for Windows version 21.0, IBM Corp., Armonk, 24-48 hours after the procedure.
New York. was used for the statistical analysis, which was
completed when p 0.05 was deemed statistically significant. Family doctors are typically the initial point of contact
for persons with lateral epicondylitis.[21] They are expected
IV. RESULTS to comprehend the causes of the disease, select the most
effective treatment plan, and immediately refer difficult
The average age of the study population was 37.4 ± 8.3 cases for professional assistance.[22] This helps to reduce
years, and the average length of sickness was 17.9 ± 4.2 morbidity caused by conditions. Additionally, lignocaine,
weeks (n = 48; male: female 27:21). None of the patients the local anaesthetic used in our experiment, has a number
had bilateral atypia, and the right-to-left-sided ratio was 2:1. of benefits that make the combo therapy interesting.
The baseline VAS score was 5.8 ± 0.9, and all follow-ups Together, they boost the steroid's effects and lengthen their
showed a substantial decrease in VAS (p 0.0001). 40 duration.[23] The lignocaine injection has also been used as
patients exhibited good improvement in the first week, 4 a diagnostic marker before steroid administration.[24] An
showed moderate improvement, 2 showed modest effective response to the subsequent steroid injection is
improvement, and 2 showed no improvement at all. The rate predicted by a significant decrease in pain following the
of improvement in all patients at 42 days is shown in Figure lignocaine injection. The researchers have also tested with
1. None of the patients suffered any significant post- growth hormones, PRP, and botulinum toxin. [25-28] The
procedure problems, and they all ceased taking their ideal treatment for chronic lateral epicondylitis has not been
analgesic prescriptions within 72 hours after the procedure. identified by any published trials or meta-analyses. [28] The
All patients were advised to have a sling for 24 hours after controversy is further brought on by the lack of a clear
injection to support the elbow. pathogenic mechanism that might be used to identify tennis
elbow. Recent literature has prioritized a degenerative
process above an inflammatory process. [29] This is
established despite the fact that the majority of steroid-
related research have shown immediate and long-lasting
benefits in the condition. Recent literature is flooded with
studies showing the advantages of growth factors, PRP, or
whole blood. The key mediators of the beneficial effects of
blood and blood products are the growth factors produced
by the platelets, which help with tissue repair and
regeneration. [30] Our study, which demonstrated the value
of combination therapy, had some drawbacks, including
limited sample size, the use of patients from a single ethnic
group, and the absence of a placebo group for comparison.
VI. CONCLUSION
We demonstrated that the local infiltrations of
lignocaine and steroids had a beneficial effect on the tennis
elbow. Our study is particularly relevant to underdeveloped
countries because they have more limited access to and
higher costs for ultrasonic therapy and botulinum toxin.
Additional randomized studies with many patients are
IJISRT23MAY2623 www.ijisrt.com 3125
Volume 8, Issue 5, May – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
required to determine the best course of treatment for lateral [13]. Rompe JD, Kirkpatrick CJ, Küllmer K, et al. Dose-
epicondylitis. related effects of shock waves on rabbit tendo Achillis.
Financial support and sponsorship A sonographic and histological study. J Bone Joint
Nil Surg Br. 1998;80(3):546-552.
[14]. Connell DA, Ali KE, Ahmad M, et al. Ultrasound-
Conflicts of interest guided autologous blood injection for tennis
There aren't any competing interests. elbow. Skeletal Radiol. 2006;35(6):371-377.
[15]. Mishra AK, Skrepnik NV, Edwards SG, et al. Efficacy
REFERENCES of platelet-rich plasma for chronic tennis elbow: a
double-blind, prospective, multicenter, randomized
[1]. Behrens SB, Deren ME, Matson AP, Bruce B, Green controlled trial of 230 patients. Am J Sports Med.
A. A review of modern management of lateral 2014;42(2):463-471.
epicondylitis. Phys Sportsmed 2012;40:34-40. [16]. Okçu G, Erkan S, Sentürk M, Ozalp RT, Yercan HS.
[2]. Zeisig E. Natural course in tennis elbow – Lateral Evaluation of injection techniques in the treatment of
epicondylitis after all? Knee Surg Sports Traumatol lateral epicondylitis: A prospective randomized clinical
Arthrosc 2012;20:2549-52. trial. Acta Orthop Traumatol Turc 2012;46:26-9.
[3]. Nirschl RP. Tennis elbow tendinosis: Pathoanatomy, [17]. Tonks JH, Pai SK, Murali SR. Steroid injection therapy
nonsurgical and surgical management. In: Gordon SL, is the best conservative treatment for lateral
Blair SJ, Fine LJ, editors. Repetitive Motion Disorders epicondylitis: A prospective randomised controlled
of the Upper Extremity. Rosemont, IL: American trial. Int J Clin Pract 2007;61:240-6.
Academy of Orthopaedic Surgeons; 1995. p. 467-79. [18]. Kazemi M, Azma K, Tavana B, Rezaiee Moghaddam
[4]. Alfredson H, Ljung BO, Thorsen K, et al. In vivo F, Panahi A. Autologous blood versus corticosteroid
investigation of ECRB tendons with microdialysis local injection in the short-term treatment of lateral
technique—no signs of inflammation but high amounts elbow tendinopathy: A randomized clinical trial of
of glutamate in tennis elbow. Acta Orthop Scand. efficacy. Am J Phys Med Rehabil 2010;89:660-7.
2000;71:475-479. [19]. Wolf JM, Ozer K, Scott F, Gordon MJ, Williams AE.
[5]. Goldie I. Epicondylitis lateralis humeri (epicondylalgia Comparison of autologous blood, corticosteroid, and
or tennis elbow): a pathogenetical study. Acta Chir saline injection in the treatment of lateral epicondylitis:
Scand Suppl. 1964;57(suppl 339). A prospective, randomized, controlled multicenter
[6]. Kraushaar B, Nirschl R. Tendinosis of the elbow study. J Hand Surg Am 2011;36:1269-72.
(tennis elbow): clinical features and findings of [20]. Lewis M, Hay EM, Paterson SM, Croft P. Local
histological, immunohistochemical, and electron steroid injections for tennis elbow: Does the pain get
microscopy studies. J Bone Joint Surg Am. worse before it gets better?: Results from a randomized
1999;81:259-285. controlled trial. Clin J Pain 2005;21:330-4.
[7]. Ljung BO, Alfredson H, Forsgren S. Neurokinin 1- [21]. Johnson GW, Cadwallader K, Scheffel SB, Epperly
receptors and sensory neuropeptides in tendon TD. Treatment of lateral epicondylitis. Am Fam
insertions at the medial and lateral epicondyles of the Physician 2007;76:843-8.
humerus: studies on tennis elbow and medial [22]. American Academy of Family Physicians. Information
epicondylalgia. J Orthop Res. 2004;22:321-327. from your family doctor. Tennis elbow: What you
[8]. Nirschl RP, Pettrone FA. Tennis elbow: the surgical should know. Am Fam Physician 2007;76:853.
treatment of lateral epicondylitis. J Bone Joint Surg [23]. Yarrobino TE, Kalbfleisch JH, Ferslew KE, Panus PC.
Am. 1979;61:832-839. Lidocaine iontophoresis mediates analgesia in lateral
[9]. Bisset L, Beller E, Jull G, et al. Mobilisation with epicondylalgia treatment. Physiother Res Int
movement and exercise, corticosteroid injection, or 2006;11:152-60.
wait and see for tennis elbow: randomised trial. BMJ. [24]. Mehra A, Zaman T, Jenkin AI. The use of a mobile
2006;333(7575):939. lithotripter in the treatment of tennis elbow and plantar
[10]. midt N, van der Windt DAWM, Assendelft WJJ, et fasciitis. Surgeon 2003;1:290-2
al. Corticosteroid injections, physiotherapy, or a wait- [25]. Maffulli N, Longo UG, Denaro V. Novel approaches
and-see policy for lateral epicondylitis: a randomised for the management of tendinopathy. J Bone Joint Surg
controlled trial. Lancet. 2002;359:657-662. Am 2010;92:2604-13.
[11]. Lee SS, Kang S, Park NK, et al. Effectiveness of initial [26]. Mishra A, Pavelko T. Treatment of chronic elbow
extracorporeal shock wave therapy on the newly tendinosis with buffered platelet-rich plasma. Am J
diagnosed lateral or medial epicondylitis. Ann Rehabil Sports Med 2006;34:1774-8.
Med. 2012;36(5):681-687 [27]. Lin YC, Tu YK, Chen SS, Lin IL, Chen SC, Guo HR.
[12]. Pettrone FA, McCall BR. Extracorporeal shock wave Comparison between botulinum toxin and
therapy without local anesthesia for chronic lateral corticosteroid injection in the treatment of acute and
epicondylitis. J Bone Joint Surg Am. 2005;87(6):1297- subacute tennis elbow: A prospective, randomized,
1304. double-blind, active drug-controlled pilot study. Am J
Phys Med Rehabil 2010;89:653-9.
IJISRT23MAY2623 www.ijisrt.com 3126
Volume 8, Issue 5, May – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[28]. Labelle H, Guibert R, Joncas J, Newman N, Fallaha M,
Rivard CH. Lack of scientific evidence for the
treatment of lateral epicondylitis of the elbow. An
attempted meta-analysis. J Bone Joint Surg Br
1992;74:646-51.
[29]. NirschlRP, AshmanES. Tennis elbow
tendinosis(epicondylitis). Instr Course Lect
2004;53:587-98.
[30]. Molloy T, Wang Y, Murrell G. The roles of growth
factors in tendon and ligament healing. Sports Med
2003;33:381-94
IJISRT23MAY2623 www.ijisrt.com 3127
You might also like
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Intradiscal injections reduce chronic low back painDocument7 pagesIntradiscal injections reduce chronic low back painNura Eky VNo ratings yet
- Ly Pen 2012 Steroidinjectionvssurgeryin CTS2 YearsfolloupDocument9 pagesLy Pen 2012 Steroidinjectionvssurgeryin CTS2 YearsfolloupElPejelagartoNo ratings yet
- Full TextDocument7 pagesFull TextJuan Pablo Casanova AnguloNo ratings yet
- (Repetido) Sirve Pudmedvalera-Garrido2014Document10 pages(Repetido) Sirve Pudmedvalera-Garrido2014Franco Suazo MoralesNo ratings yet
- Medicine: Treatment of Lateral Epicondylitis With Acupuncture and GlucocorticoidDocument3 pagesMedicine: Treatment of Lateral Epicondylitis With Acupuncture and Glucocorticoidindra coolNo ratings yet
- Efficacy of Intermittent Epidural Dexamethasone Bolus For Zoster-Associated Pain Beyond The Acute PhaseDocument8 pagesEfficacy of Intermittent Epidural Dexamethasone Bolus For Zoster-Associated Pain Beyond The Acute PhaseRoyNo ratings yet
- Comparison of Subacromial Ketorolac Injection Versus Corticosteroid Injection in The Treatment of Shoulder Impingement SyndromeDocument5 pagesComparison of Subacromial Ketorolac Injection Versus Corticosteroid Injection in The Treatment of Shoulder Impingement SyndromeDiego RodríguezNo ratings yet
- Back Pain, Mechanical Musculoskeletal Problems, Local Soft Tissue DisordersDocument1 pageBack Pain, Mechanical Musculoskeletal Problems, Local Soft Tissue DisordersPaoloLansangNo ratings yet
- TNF TreatmentDocument9 pagesTNF Treatmentachal12No ratings yet
- SMW 10163 PDFDocument9 pagesSMW 10163 PDFAngela PagliusoNo ratings yet
- Lignocaine 5 DayDocument12 pagesLignocaine 5 DayroboNo ratings yet
- Discectomy Compared With Standardized Nonoperative Care For Chronic Sciatica Due To A Lumbar Disc HerniationDocument9 pagesDiscectomy Compared With Standardized Nonoperative Care For Chronic Sciatica Due To A Lumbar Disc HerniationJosé Alberto RMNo ratings yet
- Assessing Pain Relief Following Medical and Surgical Interventions For Lumbar Disc HerniationDocument4 pagesAssessing Pain Relief Following Medical and Surgical Interventions For Lumbar Disc HerniationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Lopez 2021Document9 pagesLopez 2021toaldoNo ratings yet
- A Prospective Comparative Study of Local Steroid Injection Vs Dry Needling For Plantar Fasciitis - January - 2022 - 4974165287 - 9014391Document5 pagesA Prospective Comparative Study of Local Steroid Injection Vs Dry Needling For Plantar Fasciitis - January - 2022 - 4974165287 - 9014391Shivalingaiah GirishNo ratings yet
- Hypertonic Dextrose (Prolotherapy)Document8 pagesHypertonic Dextrose (Prolotherapy)RensoBerlangaNo ratings yet
- Effect Observation of Electro Acupunctute AnesthesiaDocument7 pagesEffect Observation of Electro Acupunctute Anesthesiaadink mochammadNo ratings yet
- Original Research: Epidural Steroids, Etanercept, or Saline in Subacute SciaticaDocument10 pagesOriginal Research: Epidural Steroids, Etanercept, or Saline in Subacute SciaticaHarshoi KrishannaNo ratings yet
- Assessment of The Effect of Epidural Steroid Injection in Patient Having Lumbar RadiculopathyDocument5 pagesAssessment of The Effect of Epidural Steroid Injection in Patient Having Lumbar RadiculopathyIJAR JOURNALNo ratings yet
- Art - LDocument10 pagesArt - LCarlos TorresNo ratings yet
- Kraus 2021Document7 pagesKraus 2021翁嘉聰No ratings yet
- 2yearfolllowupblock PDFDocument12 pages2yearfolllowupblock PDFElena Casado PinedaNo ratings yet
- Analgesic Efficacy of Erector Spinae Plane BlocksDocument7 pagesAnalgesic Efficacy of Erector Spinae Plane BlocksAlejandra SanchezNo ratings yet
- Therapeutic Effect of Cocktail VS Prolotherapy Injection in Chronic Plantar Fasciitis, A Prospective Controlled Randomized Clinical StudyDocument9 pagesTherapeutic Effect of Cocktail VS Prolotherapy Injection in Chronic Plantar Fasciitis, A Prospective Controlled Randomized Clinical StudyIJAR JOURNALNo ratings yet
- Local Steroid Injection Versus Wrist Splinting For Carpal Tunnel Syndrome: A Randomized Clinical TrialDocument6 pagesLocal Steroid Injection Versus Wrist Splinting For Carpal Tunnel Syndrome: A Randomized Clinical Trialsamsara vrindaNo ratings yet
- The Determination of The Efficacy of Neural Therapy in Conservative Treatment Resistant Patients With Chronic Low Back PainDocument8 pagesThe Determination of The Efficacy of Neural Therapy in Conservative Treatment Resistant Patients With Chronic Low Back PainfalmvenNo ratings yet
- Open Patellar Tendon Debridement For Treatment of Recalcitrant Patellar Tendinopathy: Indications, Technique, and Clinical Outcomes After A 2-Year Minimum Follow-UpDocument5 pagesOpen Patellar Tendon Debridement For Treatment of Recalcitrant Patellar Tendinopathy: Indications, Technique, and Clinical Outcomes After A 2-Year Minimum Follow-Upbustyeva77No ratings yet
- HarmacologyonlineDocument8 pagesHarmacologyonlineHisyam MuzakkiNo ratings yet
- Treatment of Lateral EpicondylitisDocument6 pagesTreatment of Lateral EpicondylitisaimanshalpyNo ratings yet
- LSM 22522Document7 pagesLSM 22522Noura RoseNo ratings yet
- Article 8Document4 pagesArticle 8umair muqriNo ratings yet
- DOR_FENOL_Chemical-Ablation-of-Genicular-Nerve-with-Phenol-for-Pain-Relief-in-Patients-with-Knee-Osteoarthritis-A-Prospective-Study_compressedDocument7 pagesDOR_FENOL_Chemical-Ablation-of-Genicular-Nerve-with-Phenol-for-Pain-Relief-in-Patients-with-Knee-Osteoarthritis-A-Prospective-Study_compressedGustavo FredericoNo ratings yet
- Effectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryDocument6 pagesEffectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2013 Knee Prolotherapy RCTDocument9 pages2013 Knee Prolotherapy RCTReyn JohnsonNo ratings yet
- Does Ultrasonography Guided Steroid Injections Provide Better Outcome in Shoulder Impingement Syndrome? A Prospective StudyDocument12 pagesDoes Ultrasonography Guided Steroid Injections Provide Better Outcome in Shoulder Impingement Syndrome? A Prospective StudyIJAR JOURNALNo ratings yet
- Research ArticleDocument8 pagesResearch ArticlesefhilaputriNo ratings yet
- A Comparative Study of Effectiveness Between Topical Insulin Versus Normal Saline Dressings in Management of Diabetic Foot UlcersDocument13 pagesA Comparative Study of Effectiveness Between Topical Insulin Versus Normal Saline Dressings in Management of Diabetic Foot UlcersIJAR JOURNALNo ratings yet
- Analgesia en Apendicitis AgudaDocument3 pagesAnalgesia en Apendicitis Agudasilvia barbosaNo ratings yet
- Keywords:-Anaesthetics, Bupivacaine, Impaction, InferiorDocument8 pagesKeywords:-Anaesthetics, Bupivacaine, Impaction, InferiorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Local Injection Treatment For Lateral Epicondylitis: T. Altay, MD I. Günal, MD and H. Öztürk, MDDocument4 pagesLocal Injection Treatment For Lateral Epicondylitis: T. Altay, MD I. Günal, MD and H. Öztürk, MDPankaj VatsaNo ratings yet
- Bmjsem 2020 000760Document19 pagesBmjsem 2020 000760Ines Riera MoyaNo ratings yet
- Corticosteroids For Herpes Zoster Are They AccompalishDocument9 pagesCorticosteroids For Herpes Zoster Are They AccompalishMerliana DebyantiNo ratings yet
- The Impact of Novel Inflammation-Preserving TreatmDocument11 pagesThe Impact of Novel Inflammation-Preserving TreatmlalyphyocentroNo ratings yet
- Maddalozzo 2018Document8 pagesMaddalozzo 2018Rolando TijerinaNo ratings yet
- Tens HNPDocument6 pagesTens HNPUniquaNo ratings yet
- 1495 PDFDocument8 pages1495 PDFSusan Wulandari ApriLiaNo ratings yet
- TEnsDocument10 pagesTEnsmarcelogascon.oNo ratings yet
- NiceDocument7 pagesNiceRisky Ilona SaputraNo ratings yet
- Medi 96 E6490Document4 pagesMedi 96 E6490TheEdgeNo ratings yet
- International Journal of Anesthetics and Anesthesiology Ijaa 7 118Document7 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 7 118Ferdy RahadiyanNo ratings yet
- Wu 2019Document8 pagesWu 2019Cristobal Concha GiesenNo ratings yet
- Ultrasound TerapyDocument4 pagesUltrasound TerapykarolndNo ratings yet
- Giray 2019Document13 pagesGiray 2019Felix LoaizaNo ratings yet
- Effects of Heavy Slow Resistance Training Combined With Corticosteroid Injections or Tendon Needling in Patients With Lateral Elbow TendinopathyDocument10 pagesEffects of Heavy Slow Resistance Training Combined With Corticosteroid Injections or Tendon Needling in Patients With Lateral Elbow TendinopathyaaNo ratings yet
- CyrotherapyDocument6 pagesCyrotherapyapi-302507867No ratings yet
- Tangtiphaiboontana 2021Document8 pagesTangtiphaiboontana 2021翁嘉聰No ratings yet
- IJHSRUN CaseReportDocument5 pagesIJHSRUN CaseReportIndah YulantariNo ratings yet
- Tennis Elbow Brace and Wrist Cock-Up Splint in The Management of Tennis Elbow: A Comparative StudyDocument4 pagesTennis Elbow Brace and Wrist Cock-Up Splint in The Management of Tennis Elbow: A Comparative StudyAjayNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing the Use of Improved Maize Seed and Participation in the Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing the Use of Improved Maize Seed and Participation in the Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain based Decentralized ApplicationDocument7 pagesBlockchain based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power for the Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power for the Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry that Capitalizes off of Women’s Insecurities?Document8 pagesAn Industry that Capitalizes off of Women’s Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Visual Water: An Integration of App and Web to Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web to Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson’s Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson’s Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in a Stenosed Artery under the Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in a Sten. Art. Under the Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in a Stenosed Artery under the Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in a Sten. Art. Under the Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System for Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System for Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction using Bi-LSTMDocument8 pagesAir Quality Index Prediction using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict the Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict the Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolDocument31 pagesThe Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis on Mental Health Issues among IndividualsDocument6 pagesAn Analysis on Mental Health Issues among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget’s Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget’s Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation for Translating Global Languages into Indian LanuagesDocument7 pagesHarnessing Open Innovation for Translating Global Languages into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Exploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractDocument7 pagesExploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions on Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions on Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonDocument14 pagesTerracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- SALTAPSDocument24 pagesSALTAPSFatima Tu ZahraNo ratings yet
- Lifestyle Diseases: Consequences, Characteristics, Causes and ControlDocument4 pagesLifestyle Diseases: Consequences, Characteristics, Causes and Controlmelbe5jane5quiamcoNo ratings yet
- Panic Ch. Clark & Salkvoskis.2009Document87 pagesPanic Ch. Clark & Salkvoskis.2009Dana CojocaruNo ratings yet
- Protein Energy MalnutritionDocument24 pagesProtein Energy Malnutritionapi-312933466100% (1)
- DepEd Health FormDocument1 pageDepEd Health Formrufino delacruzNo ratings yet
- Guidelines For The Surgical Treatment of Esophageal Achalasia PDFDocument24 pagesGuidelines For The Surgical Treatment of Esophageal Achalasia PDFInomy ClaudiaNo ratings yet
- Laporan Bulanan Data Kesakitan 145 Penyakit Di Puskesmas Batuan Bulan Agustus Tahun 2017Document26 pagesLaporan Bulanan Data Kesakitan 145 Penyakit Di Puskesmas Batuan Bulan Agustus Tahun 2017Pkm BatuanNo ratings yet
- Use of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyDocument5 pagesUse of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyRafael MartinsNo ratings yet
- PDF JnFmyW1qOR70whlpf4M2Document2 pagesPDF JnFmyW1qOR70whlpf4M2SAI SMARAN INTURINo ratings yet
- KOGA AnalysisDocument6 pagesKOGA AnalysisLenka KořínkováNo ratings yet
- Cancer InnovationsDocument60 pagesCancer Innovationseustaquiocajaenpena100% (2)
- Metabolic Syndrome: Risk Factors and Lifestyle ChangesDocument3 pagesMetabolic Syndrome: Risk Factors and Lifestyle ChangesYudha SavestilaNo ratings yet
- Kondiloma AkuminataDocument4 pagesKondiloma AkuminataIntan PermataNo ratings yet
- Colegio de San Juan de Letran: College of Liberal Arts and SciencesDocument7 pagesColegio de San Juan de Letran: College of Liberal Arts and SciencesMaria Elena AquinoNo ratings yet
- Diams PDFDocument80 pagesDiams PDFDr.Mohammed Mustafa Iqbal100% (3)
- Urn - Isbn - 978 952 61 2713 2Document136 pagesUrn - Isbn - 978 952 61 2713 2dewi najiraNo ratings yet
- Anatomi Tenggorokan Dan Penerapan Klinisnya: Dr. Adi Arianto, M. BiomedDocument39 pagesAnatomi Tenggorokan Dan Penerapan Klinisnya: Dr. Adi Arianto, M. BiomedAl AdinNo ratings yet
- Benign Ovarian TumorsDocument5 pagesBenign Ovarian Tumorsraissametasari100% (1)
- Emergency Surgical Service1Document11 pagesEmergency Surgical Service1Afkar30No ratings yet
- Parasitology (Lect #6) TransDocument3 pagesParasitology (Lect #6) TransAndrea Galang CruzNo ratings yet
- Case Study - Nephrotic SyndromeDocument42 pagesCase Study - Nephrotic Syndromefarmasi rsud cilincingNo ratings yet
- Covid ArticleDocument5 pagesCovid ArticleAnisulHaqueNo ratings yet
- Oral Medicine and Radiology MCQDocument7 pagesOral Medicine and Radiology MCQsamhita100% (1)
- Articulo Manejo Paciente IrcDocument8 pagesArticulo Manejo Paciente IrcJUAN FONSECANo ratings yet
- DOH Approved Herbal Medicines for Skin DiseasesDocument5 pagesDOH Approved Herbal Medicines for Skin DiseasesYohan NahoNo ratings yet
- Dengue DOHDocument16 pagesDengue DOHGehlatin Tumanan100% (1)
- Guideline Trombositosis 2004Document18 pagesGuideline Trombositosis 2004Jicko Street HooligansNo ratings yet
- Pathogenesis of Nephrotic SyndromeDocument33 pagesPathogenesis of Nephrotic SyndromeHari Mukti100% (1)
- Arrythmias 2-3Document4 pagesArrythmias 2-3cayla mae carlosNo ratings yet
- Revised Monthly Reporting Format - HWCDocument8 pagesRevised Monthly Reporting Format - HWCChanmari West Sub-Centre50% (2)