You might also like
- Antiplatelet and Anticoagulation GuideDocument31 pagesAntiplatelet and Anticoagulation GuideMarcelliaNo ratings yet
- WECOC - Management of NSTEMI and Invasive StrategyDocument42 pagesWECOC - Management of NSTEMI and Invasive StrategyAdiyanto DidietNo ratings yet
- CCU 2017 AntiplateletDocument22 pagesCCU 2017 AntiplateletDhinie NovianiNo ratings yet
- Strokeaha 120 033033Document7 pagesStrokeaha 120 033033MarisolCamposNo ratings yet
- Management of Stroke Prevention in Atrial Fibrillation Patients with Multimorbid: Focus on Elderly and Renal ImpairmentDocument33 pagesManagement of Stroke Prevention in Atrial Fibrillation Patients with Multimorbid: Focus on Elderly and Renal ImpairmentSofia KusumadewiNo ratings yet
- PrintDocument6 pagesPrintjihan ulNo ratings yet
- Strokeaha 120 033033Document7 pagesStrokeaha 120 033033AudryaNo ratings yet
- Paradise TrialDocument26 pagesParadise TrialMiguel Martinez DuranNo ratings yet
- Curriculum Vitae: Nama: Dr. I B Kusuma P, SP.S TGL Lahir: 27 Maret 1964 Riwayat PendidikanDocument31 pagesCurriculum Vitae: Nama: Dr. I B Kusuma P, SP.S TGL Lahir: 27 Maret 1964 Riwayat PendidikanJuliana sieNo ratings yet
- Su 2015Document7 pagesSu 2015carolin enjelin rumaikewiNo ratings yet
- Advanced The Anticoagulant Co-Therapy in STE-ACS Patients Role of Enoxaparine REVISIDocument24 pagesAdvanced The Anticoagulant Co-Therapy in STE-ACS Patients Role of Enoxaparine REVISIArniNo ratings yet
- Exanple Re-Ly-Trial-DabigatranDocument5 pagesExanple Re-Ly-Trial-DabigatranPollaRxsu RuenroengboonNo ratings yet
- FFR NurturingaFunctionalPerspectiveinAngioplastyDocument30 pagesFFR NurturingaFunctionalPerspectiveinAngioplastyTakhleeq AkhterNo ratings yet
- Atorvastatin Statin in CVD ManagementDocument37 pagesAtorvastatin Statin in CVD ManagementSriNo ratings yet
- Statins in CVD Management: Is Just Lipid Lowering Enough?Document37 pagesStatins in CVD Management: Is Just Lipid Lowering Enough?SriNo ratings yet
- Ehf2 7 1125Document5 pagesEhf2 7 1125Pranvera ApostoliNo ratings yet
- Iacta 2011 Janak Mehta Award Winning PresentationDocument56 pagesIacta 2011 Janak Mehta Award Winning PresentationDr.Sandeep Kumar KarNo ratings yet
- The Results of The Study of Heart and Renal Protection (SHARP)Document19 pagesThe Results of The Study of Heart and Renal Protection (SHARP)Surya MahardikaNo ratings yet
- Statins Reduce Risk of Post-Stroke Seizures & Epilepsy in Several StudiesDocument12 pagesStatins Reduce Risk of Post-Stroke Seizures & Epilepsy in Several Studiesallyssa rahmadittaNo ratings yet
- 09.30 Professor John Townend, Chest Pain and Troponins On The Acute TakeDocument39 pages09.30 Professor John Townend, Chest Pain and Troponins On The Acute Takeamir ahmadNo ratings yet
- Sca 2019Document69 pagesSca 2019PLIFNo ratings yet
- Scottish Medicines Consortium (1) .Dabigatran - Pradaxa - FINAL - August - 2011 - Amended - 05.09.11 - For - WebsiteDocument13 pagesScottish Medicines Consortium (1) .Dabigatran - Pradaxa - FINAL - August - 2011 - Amended - 05.09.11 - For - WebsiteMarcelo UGNo ratings yet
- Anti Platlet and StrokeDocument25 pagesAnti Platlet and StrokeSurat TanprawateNo ratings yet
- Activase Rt-PA (Acute Ischemic Stroke)Document11 pagesActivase Rt-PA (Acute Ischemic Stroke)bishoy.youssef.cpiNo ratings yet
- HYVET ResultsDocument21 pagesHYVET Resultsjejus100% (4)
- 080630 고혈압최신지견 (조장현 과장님)Document46 pages080630 고혈압최신지견 (조장현 과장님)hongmyongNo ratings yet
- Angiotensin Receptor Neprilysin Inhibition (ARNI) Following Acute Myocardial Infarction: Primary Results of The PARADISE-MI TrialDocument26 pagesAngiotensin Receptor Neprilysin Inhibition (ARNI) Following Acute Myocardial Infarction: Primary Results of The PARADISE-MI TrialsumaNo ratings yet
- Treatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlideDocument31 pagesTreatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlidejoshuaNo ratings yet
- Fsurg 10 1285553Document11 pagesFsurg 10 1285553William ChokNo ratings yet
- Blockade R A SDocument20 pagesBlockade R A SAlaa KhazalehNo ratings yet
- Management of CADDocument99 pagesManagement of CADUmesh BabuNo ratings yet
- Yashwanth - IHD HFrEfDocument16 pagesYashwanth - IHD HFrEfYashwanth N BNo ratings yet
- Antiplatelet Therapy September 2013Document31 pagesAntiplatelet Therapy September 2013Randilufti SantosoNo ratings yet
- RidkerJUPITERslides - MPT - sld1Document12 pagesRidkerJUPITERslides - MPT - sld1Nawel BenNo ratings yet
- "Adjunctive Therapy" Non ST Segment Elevation ACS: DR M R Thomas King's College Hospital. Advanced Angioplasty 2002Document42 pages"Adjunctive Therapy" Non ST Segment Elevation ACS: DR M R Thomas King's College Hospital. Advanced Angioplasty 2002usfcardsNo ratings yet
- PlavixDocument80 pagesPlavixFatahillah NazarNo ratings yet
- Cerebrovascular Diseases: Global Burden and Prevention StrategiesDocument28 pagesCerebrovascular Diseases: Global Burden and Prevention StrategiesbagussofianNo ratings yet
- Angel Yudiakristi - Praktikum 5Document10 pagesAngel Yudiakristi - Praktikum 5Angel MaharaniNo ratings yet
- Health Aging and The Top 10 Things To Ask - Dr.-William-DalzielDocument54 pagesHealth Aging and The Top 10 Things To Ask - Dr.-William-DalzielJason WongNo ratings yet
- Arni PPT 2 PDFDocument19 pagesArni PPT 2 PDFKumarsai Durusoju100% (1)
- Hennekens Cardio Aspirin Past To FutureDocument20 pagesHennekens Cardio Aspirin Past To FutureLona LetwarNo ratings yet
- Merec Bulletin Vol15 No6Document4 pagesMerec Bulletin Vol15 No6n4dn4dNo ratings yet
- Slide WS 2 Dr. Junior, SP - JP (K)Document18 pagesSlide WS 2 Dr. Junior, SP - JP (K)Luh Leni AriniNo ratings yet
- SIMPO 1.2 DR WIZA - The Practicality of Enoxaparin Across ACS Spectrum - 2022Document23 pagesSIMPO 1.2 DR WIZA - The Practicality of Enoxaparin Across ACS Spectrum - 2022yan salviantoNo ratings yet
- Biomedik 3 Rational TherapyDocument51 pagesBiomedik 3 Rational TherapyMarissaMatinahoruNo ratings yet
- Topic - ADocument4 pagesTopic - Aapi-549451092No ratings yet
- PC Slides Packer - EMPEROR-ReducedDocument6 pagesPC Slides Packer - EMPEROR-ReducedSaul RuizNo ratings yet
- Drug Class Overviews Angiotensin Converting Enzyme ACE Inhibitors Clinical PharmacologyDocument12 pagesDrug Class Overviews Angiotensin Converting Enzyme ACE Inhibitors Clinical PharmacologyMichael KeenanNo ratings yet
- CYP450 System and Not BeingDocument5 pagesCYP450 System and Not BeingArfa'i LaksamanaNo ratings yet
- TWILIGHTDocument24 pagesTWILIGHTRodrigo MartinNo ratings yet
- Resurgence of Beta Blocker-Focus On HTDocument47 pagesResurgence of Beta Blocker-Focus On HTAkhil SharmaNo ratings yet
- Doac Vs AvkDocument32 pagesDoac Vs AvkOlga BabiiNo ratings yet
- The Role of Lung Impedance Monitoring in The Outpatient Clinic For Predicting and Preventing of Hospitalizations of Patients With Chronic Heart FailureDocument19 pagesThe Role of Lung Impedance Monitoring in The Outpatient Clinic For Predicting and Preventing of Hospitalizations of Patients With Chronic Heart FailureAmanda TeacaNo ratings yet
- Atrial-Fibrillation-finalDocument67 pagesAtrial-Fibrillation-finalHafiz Wajid SadiqNo ratings yet
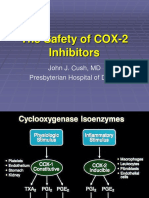
- The Safety of COX-2 Inhibitors: A Review of Clinical Trial DataDocument29 pagesThe Safety of COX-2 Inhibitors: A Review of Clinical Trial DataHerry HendrayadiNo ratings yet
- Prof Kiking Ritarwan - STROKE-KRTDocument64 pagesProf Kiking Ritarwan - STROKE-KRTBernard Fernandes PanjaitanNo ratings yet
- Prevention of Stroke and Myocardial Infarction by Amlodipine and Angiotensin Receptor BlockersDocument9 pagesPrevention of Stroke and Myocardial Infarction by Amlodipine and Angiotensin Receptor BlockersSabrina MarisaNo ratings yet
- JCN 10 189 PDFDocument8 pagesJCN 10 189 PDFMeilinda SihiteNo ratings yet
- Chem 123 Problem Set 1Document4 pagesChem 123 Problem Set 1Stuart BrookesNo ratings yet
- Determine Earth's Magnetic Field Using Tangent GalvanometerDocument26 pagesDetermine Earth's Magnetic Field Using Tangent GalvanometerKusum SukhijaNo ratings yet
- In 2 PostDocument4 pagesIn 2 PostHarsha SubbarayappaNo ratings yet
- Impact of Massive MIMO Antennas on 5G Network CapacityDocument10 pagesImpact of Massive MIMO Antennas on 5G Network CapacitykamelNo ratings yet
- 3.01.01 - Acetaldehyde Determination by Enzymatic AnalysisDocument9 pages3.01.01 - Acetaldehyde Determination by Enzymatic AnalysisRiyanNo ratings yet
- Tyre Curing GuideDocument6 pagesTyre Curing GuideMALAY GUPTANo ratings yet
- Manual Swan Quad CrowDocument2 pagesManual Swan Quad CrowApex PredatorNo ratings yet
- MVC Architecture and Sales Order Entry (P42101)Document10 pagesMVC Architecture and Sales Order Entry (P42101)ashish007d100% (1)
- AutopilotDocument76 pagesAutopilotAnthony Steve LomilloNo ratings yet
- Cutnell7e TB Ch01Document10 pagesCutnell7e TB Ch01Clara LiuNo ratings yet
- PRACH Planning in LTEDocument14 pagesPRACH Planning in LTElikamele100% (1)
- Casio AT 1 Service ManualDocument28 pagesCasio AT 1 Service ManualMario Gabriel MoralliNo ratings yet
- Time Value of Money Answer KeysDocument22 pagesTime Value of Money Answer KeysrhlvajpayeeNo ratings yet
- Python Interactive Mode: Anaconda Navigator SpyderDocument5 pagesPython Interactive Mode: Anaconda Navigator SpyderDeeshpreet Kaur sonaNo ratings yet
- Step by Step To Building A Computer LabDocument7 pagesStep by Step To Building A Computer LabRaiyan RahmanNo ratings yet
- Komodo-Ide-6 1 2Document414 pagesKomodo-Ide-6 1 2Maria Josefa Vilar EstévezNo ratings yet
- PracticeProblems 4315 SolutionsDocument9 pagesPracticeProblems 4315 SolutionsKashifRizwanNo ratings yet
- High Voletage Lithium Batteries - LNMODocument2 pagesHigh Voletage Lithium Batteries - LNMOajunkie17No ratings yet
- Final Report - HVACDocument10 pagesFinal Report - HVACBenny BennyNo ratings yet
- Comparative analysis of pressure vessel cylindrical shell calculation and resultsDocument5 pagesComparative analysis of pressure vessel cylindrical shell calculation and resultszajednosexNo ratings yet
- Mensuration: Area of A TrapeziumDocument61 pagesMensuration: Area of A TrapeziumSahil EduNo ratings yet
- LQ 310 PDFDocument2 pagesLQ 310 PDFRana WahyudiNo ratings yet
- Manual de Operación de Herramientas 3116 Y 26Document29 pagesManual de Operación de Herramientas 3116 Y 26israelh4100% (6)
- DIGOO-DG-XME Digital NVR - 1215Document2 pagesDIGOO-DG-XME Digital NVR - 1215Marcelo J SolanoNo ratings yet
- 12 Bar Blues EssayDocument3 pages12 Bar Blues EssayblondieajbNo ratings yet
- Johan Sundberg. Intonation in Singing.Document15 pagesJohan Sundberg. Intonation in Singing.Юрий СемёновNo ratings yet
- Schematic Learning Definition of Term Technique: Basic Terms General DefinitionsDocument8 pagesSchematic Learning Definition of Term Technique: Basic Terms General DefinitionsKifaru Micro-electronics100% (1)
- Final BFK40303 2018 2019 Sem 2Document6 pagesFinal BFK40303 2018 2019 Sem 2EJ KooNo ratings yet
- ThermodynamicsDocument9 pagesThermodynamicssamir boseNo ratings yet
- Conzerv EM6400 Series Power Meters: User ManualDocument81 pagesConzerv EM6400 Series Power Meters: User ManualJayakanthan SangeeNo ratings yet