You might also like
- AP Macroeconomics Review Sheet 2013Document7 pagesAP Macroeconomics Review Sheet 2013Crystal Farmer100% (4)
- Sanger Dummy ReportDocument3 pagesSanger Dummy ReportAakash vermaNo ratings yet
- Mycobacterium Tuberculosis With Low-And High-Level ResistanceDocument6 pagesMycobacterium Tuberculosis With Low-And High-Level ResistanceGirish Kishor PaiNo ratings yet
- 81572-Article Text-197102-1-10-20170330Document10 pages81572-Article Text-197102-1-10-20170330Lydie Praxede EkoboNo ratings yet
- Mjhid 4 1 E2012024Document5 pagesMjhid 4 1 E2012024joseNo ratings yet
- Clinical Signi Cance of Oncogenic KIT and PDGFRA Mutations in Gastrointestinal Stromal Tumours PDFDocument22 pagesClinical Signi Cance of Oncogenic KIT and PDGFRA Mutations in Gastrointestinal Stromal Tumours PDFCarla CarolineNo ratings yet
- EPIGENETICS DRUG THERAPYpptx - 240118 - 070801Document43 pagesEPIGENETICS DRUG THERAPYpptx - 240118 - 070801Maryam HaniniNo ratings yet
- Platelet Antigens and Antibody Detection: Original PaperDocument5 pagesPlatelet Antigens and Antibody Detection: Original PaperstasirobertoNo ratings yet
- 5605 FullDocument5 pages5605 FullAniki PuspitaNo ratings yet
- A Second Genetic Polymorphism in Methylenetetrahydrofolate Reductase (MTHFR) Associated With Decreased Enzyme ActivityDocument4 pagesA Second Genetic Polymorphism in Methylenetetrahydrofolate Reductase (MTHFR) Associated With Decreased Enzyme ActivityMauro Porcel de PeraltaNo ratings yet
- T PMD 160884Document4 pagesT PMD 160884Rizwan TonoyNo ratings yet
- Up-Regulation of Luciferase Gene Expression With Antisense Oligonucleotides: Implications and Applications in Functional Assay DevelopmentDocument5 pagesUp-Regulation of Luciferase Gene Expression With Antisense Oligonucleotides: Implications and Applications in Functional Assay DevelopmentFilip IlievskiNo ratings yet
- Cytocrom FuntionDocument24 pagesCytocrom FuntionJorge Ramirez RaherNo ratings yet
- DNA Polymorphism of Butyrophilin Gene by PCR-RFLP Technique: Full Length Research PaperDocument3 pagesDNA Polymorphism of Butyrophilin Gene by PCR-RFLP Technique: Full Length Research PaperHAEDIRNo ratings yet
- Hyperserotonemia in Autism: The Potential Role of 5HT-related Gene VariantsDocument6 pagesHyperserotonemia in Autism: The Potential Role of 5HT-related Gene VariantsWesley MuhammadNo ratings yet
- B1JVSb ThapaDocument6 pagesB1JVSb ThapaDrashua AshuaNo ratings yet
- Pnas 201717789siDocument11 pagesPnas 201717789siygilad9139No ratings yet
- Himmelfarb 2004Document9 pagesHimmelfarb 2004Julieta SeifertNo ratings yet
- Supplementary Materials ForDocument37 pagesSupplementary Materials Forperito superNo ratings yet
- Ex SkippingDocument6 pagesEx SkippinganaNo ratings yet
- Week4 PCR Detailed StrategyDocument6 pagesWeek4 PCR Detailed StrategyArjun BujjiNo ratings yet
- Producing Kpc-Type Carbapenemases Mediated by Insertional Inactivation of The Phoq/Phop MGRB RegulatorDocument6 pagesProducing Kpc-Type Carbapenemases Mediated by Insertional Inactivation of The Phoq/Phop MGRB RegulatorABachiraya MongkhunNo ratings yet
- Il28b 2015Document7 pagesIl28b 2015Hafsa AzizNo ratings yet
- Gutjnl 2018 317856 Inline Supplementary Material 1Document21 pagesGutjnl 2018 317856 Inline Supplementary Material 1吳杺No ratings yet
- 1070 Impact of MTHFR rs1801133 MTHFR rs1801131 and Abcb1 rs1045642 Polymorphisms With Increased Susceptibility of Rheumatoid Arthritis in The West Algerian Population A Case Control Study FileDocument9 pages1070 Impact of MTHFR rs1801133 MTHFR rs1801131 and Abcb1 rs1045642 Polymorphisms With Increased Susceptibility of Rheumatoid Arthritis in The West Algerian Population A Case Control Study FileFaMe TanapornNo ratings yet
- Perrey 1998Document5 pagesPerrey 1998Shukr Wesman BlbasNo ratings yet
- MupB A New High Level Mechanism in S. AureusDocument5 pagesMupB A New High Level Mechanism in S. AureusM Shaheen IqbalNo ratings yet
- Hallock, Lee, Ramamoorthy - 2003 - MSI-78, An Analogue of The Magainin Antimicrobial Peptides, Disrupts Lipid Bilayer Structure Via PosiDocument9 pagesHallock, Lee, Ramamoorthy - 2003 - MSI-78, An Analogue of The Magainin Antimicrobial Peptides, Disrupts Lipid Bilayer Structure Via PosiGlen van den BergenNo ratings yet
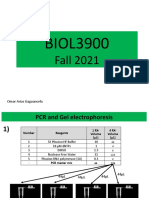
- BIOL3900: Fall 2021Document7 pagesBIOL3900: Fall 2021Arjun BujjiNo ratings yet
- Ores HAT HDACDocument7 pagesOres HAT HDACdvvargaslNo ratings yet
- Ensayos de Alto Rendimiento para La Detección de La Mutación F1534C en El Gen Del Canal de Sodio Dependiente de VoltajeDocument9 pagesEnsayos de Alto Rendimiento para La Detección de La Mutación F1534C en El Gen Del Canal de Sodio Dependiente de VoltajeJuan Miguel Castro CamachoNo ratings yet
- Macer A 1996Document5 pagesMacer A 1996dad dzd adaNo ratings yet
- GPM6A Research PaperDocument7 pagesGPM6A Research PaperRida ArifNo ratings yet
- Cloning and Expression of Human Glutamic Acid Decarboxylase (GAD 65) Gene in Escherichia ColiDocument8 pagesCloning and Expression of Human Glutamic Acid Decarboxylase (GAD 65) Gene in Escherichia ColiOpenaccess Research paperNo ratings yet
- Lab ReportDocument15 pagesLab ReportHtet Htet AungNo ratings yet
- TFG3/TAF30/ANC1, A Component of The Yeast SWI/SNF Complex That Is Similar To The Leukemogenic Proteins ENL and AF-9Document9 pagesTFG3/TAF30/ANC1, A Component of The Yeast SWI/SNF Complex That Is Similar To The Leukemogenic Proteins ENL and AF-9Eva Benito BerrocalNo ratings yet
- Spectrum of Mutations in Patients With Organic Acidurias From UkraineDocument10 pagesSpectrum of Mutations in Patients With Organic Acidurias From UkraineАнна ШаповаловаNo ratings yet
- Association of C677T MTHFR and G20210A FII Prothrombin Polymorphisms With Susceptibility To Myocardial InfarctionDocument6 pagesAssociation of C677T MTHFR and G20210A FII Prothrombin Polymorphisms With Susceptibility To Myocardial Infarctionseydou.organismNo ratings yet
- Ref 04Document11 pagesRef 04truong.nguyen.19.12.92No ratings yet
- Retroviral-Mediated Very-Long-Chain Fatty Acid Metabolism in Adrenoleukodystrophy FibroblastsDocument5 pagesRetroviral-Mediated Very-Long-Chain Fatty Acid Metabolism in Adrenoleukodystrophy FibroblastsmdquevedoNo ratings yet
- DiMarzo, Tumoral MacrophagesDocument35 pagesDiMarzo, Tumoral MacrophagesМатиас Себальос ГусманNo ratings yet
- A Unified Rapid PCR Method For Detection of NormalDocument6 pagesA Unified Rapid PCR Method For Detection of NormalShavana RajkumarNo ratings yet
- RodrguezFuentes G - Osmotic Regulation of A Novel Flavincontaining - 2008Document6 pagesRodrguezFuentes G - Osmotic Regulation of A Novel Flavincontaining - 2008Gabriela RodriguezNo ratings yet
- Molecular Diagnosis ofDocument67 pagesMolecular Diagnosis ofNadir KoçakNo ratings yet
- Vincristine Regulates The Phosphorylation of The Antiapoptotic Protein HSP27 in Breast Cancer CellsDocument10 pagesVincristine Regulates The Phosphorylation of The Antiapoptotic Protein HSP27 in Breast Cancer CellsEva Del ValleNo ratings yet
- Mdfund Unit16chapter14Document43 pagesMdfund Unit16chapter14Abigail LausNo ratings yet
- Chromatin DNA Methylation1Document43 pagesChromatin DNA Methylation1hadymatrixNo ratings yet
- 8 - geneMAP™ Thrombophilia Panel V2.3Document9 pages8 - geneMAP™ Thrombophilia Panel V2.3mirian flechaNo ratings yet
- Inhibition of Temperature Sensitive TRPV3 Channel by Two Na - 2022 - Acta PharmaDocument12 pagesInhibition of Temperature Sensitive TRPV3 Channel by Two Na - 2022 - Acta PharmaMohammed Shuaib AhmedNo ratings yet
- Expression and Characteristic of Synthetic Human Epidermal Growth Factor (hEGF) in Transgenic Tobacco PlantsDocument7 pagesExpression and Characteristic of Synthetic Human Epidermal Growth Factor (hEGF) in Transgenic Tobacco PlantsCarlos Julio Nova LopezNo ratings yet
- Misteli Et AlDocument5 pagesMisteli Et AlAmairanni HernzNo ratings yet
- Genomic Imprinting & Epigenetics: 徐国良 研究员 细胞大楼 300 电话 E-mail: glxu@sibs.ac.cnDocument53 pagesGenomic Imprinting & Epigenetics: 徐国良 研究员 细胞大楼 300 电话 E-mail: glxu@sibs.ac.cnapi-3700537No ratings yet
- Biochemistry and Biophysics ReportsDocument7 pagesBiochemistry and Biophysics ReportsMichael John AguilarNo ratings yet
- Cancer Res 1998 Potter 3627 32Document7 pagesCancer Res 1998 Potter 3627 32Frian LiaNo ratings yet
- Rusnak et al, 2001, The effects of the novel, reversible epidermal growth factor receptor:ErbB-2 tyrosine kinase inhibitor, GW2016, on the growth of human normal and tumor-derived cell lines in vitro and in vivoDocument11 pagesRusnak et al, 2001, The effects of the novel, reversible epidermal growth factor receptor:ErbB-2 tyrosine kinase inhibitor, GW2016, on the growth of human normal and tumor-derived cell lines in vitro and in vivodhania novitasariNo ratings yet
- A Chemical Biology Screen Identifies Glucocorticoids That Regulate C - 2007 - BLDocument8 pagesA Chemical Biology Screen Identifies Glucocorticoids That Regulate C - 2007 - BLTareeqanwar MohammedNo ratings yet
- 10 - Chapter 4Document10 pages10 - Chapter 4The FrequencyNo ratings yet
- JCM 32 4 1095-1098 1994Document4 pagesJCM 32 4 1095-1098 1994mariotecNo ratings yet
- Immunohistochemical Analysis of Omi/Htra2 Expression in Prostate Cancer and Benign Prostatic HyperplasiaDocument7 pagesImmunohistochemical Analysis of Omi/Htra2 Expression in Prostate Cancer and Benign Prostatic HyperplasiapadrastroNo ratings yet
- Kanaoka 1999Document6 pagesKanaoka 1999awdafeagega2r3No ratings yet
- Formulation and Development of Mint Containing Herbal Hand SanitizerDocument5 pagesFormulation and Development of Mint Containing Herbal Hand SanitizerShera NeazNo ratings yet
- Ethanol Determination Novel MethodDocument4 pagesEthanol Determination Novel MethodShera NeazNo ratings yet
- P 53 PathwayDocument10 pagesP 53 PathwayShera NeazNo ratings yet
- Ijaerv8n15spl 01Document9 pagesIjaerv8n15spl 01Shera NeazNo ratings yet
- Benzodiazepines (Urine) : Does This Test Have Other Names?Document4 pagesBenzodiazepines (Urine) : Does This Test Have Other Names?Shera NeazNo ratings yet
- Hci - Web Interface DesignDocument54 pagesHci - Web Interface DesigngopivrajanNo ratings yet
- Quick Charge Device ListDocument23 pagesQuick Charge Device ListIlham Nur AhzanNo ratings yet
- Tunnel Format 1 - MergedDocument9 pagesTunnel Format 1 - MergedLovely SinghNo ratings yet
- Decision Mathematics D1 January 2023 Question Paper Wdm11-01-Que-20230126Document28 pagesDecision Mathematics D1 January 2023 Question Paper Wdm11-01-Que-20230126VisakaNo ratings yet
- Experimentation, Orgasms, and The Rise of Anal Sex. - by William Saletan - SDocument13 pagesExperimentation, Orgasms, and The Rise of Anal Sex. - by William Saletan - Saweawerwerwe100% (1)
- SIEPAN 8PU Low Voltage Switchboards Technology by SiemensDocument4 pagesSIEPAN 8PU Low Voltage Switchboards Technology by SiemensaayushNo ratings yet
- NEW HOLLAND - Trucks, Tractor & Forklift Manual PDDocument14 pagesNEW HOLLAND - Trucks, Tractor & Forklift Manual PDAjjaakka0% (2)
- In The Garden of Beasts by Erik Larson - Reading Group GuideDocument9 pagesIn The Garden of Beasts by Erik Larson - Reading Group GuideCrown Publishing Group100% (1)
- Core3 SyllabusDocument2 pagesCore3 Syllabusapi-288048801No ratings yet
- Protection of Information Systems: © The Institute of Chartered Accountants of IndiaDocument28 pagesProtection of Information Systems: © The Institute of Chartered Accountants of Indiajonnajon92-1No ratings yet
- Irjece: Human Computer Interaction Direct ManipulationDocument4 pagesIrjece: Human Computer Interaction Direct ManipulationgigibowonseetNo ratings yet
- A Case Study of World Health OrganisationDocument26 pagesA Case Study of World Health OrganisationFarNo ratings yet
- Random Puzzle Questions PDF For Ibps RRB Clerk Prelims ExamDocument22 pagesRandom Puzzle Questions PDF For Ibps RRB Clerk Prelims ExamApyrvaNo ratings yet
- Mts 2003 25 1 167Document37 pagesMts 2003 25 1 167Yuri BaerNo ratings yet
- Document No.: Safety CheckDocument14 pagesDocument No.: Safety CheckRodolfo Alberto Muñoz CarcamoNo ratings yet
- Cape Law Unit 1 Mock Exam Module 2 Criminal LawDocument5 pagesCape Law Unit 1 Mock Exam Module 2 Criminal LawBrett SmithNo ratings yet
- Legacy - Wasteland AlmanacDocument33 pagesLegacy - Wasteland AlmanacВлад «Befly» Мирошниченко100% (3)
- Assignment Two CartoonsDocument3 pagesAssignment Two CartoonsAbraham Kang100% (1)
- Mat Lab Interview QuestionsDocument2 pagesMat Lab Interview QuestionsSiddu Shiva KadiwalNo ratings yet
- WILDVALLEY SHIPPING CO V CaDocument2 pagesWILDVALLEY SHIPPING CO V CaChariNo ratings yet
- Bai Tap On Tap Unit 123Document8 pagesBai Tap On Tap Unit 123Le VanNo ratings yet
- Amigurumi Angel FishDocument3 pagesAmigurumi Angel FishcapricorntranNo ratings yet
- Plan B ModuleDocument220 pagesPlan B ModuledamarwtunggadewiNo ratings yet
- International Arbitration ReviewDocument28 pagesInternational Arbitration ReviewOsagyefo Oliver Barker-VormaworNo ratings yet
- Mouth Breathing: Adverse Effects On Facial Growth, Health, Academics, and BehaviorDocument8 pagesMouth Breathing: Adverse Effects On Facial Growth, Health, Academics, and BehaviorlogoioanninaNo ratings yet
- SEMINARS AND FIELDTRIPS (59041, 59042, 59071) : Electronics Engineering DepartmentDocument3 pagesSEMINARS AND FIELDTRIPS (59041, 59042, 59071) : Electronics Engineering DepartmentDaniel TamisenNo ratings yet
- 2023 WARN Notice ListingsDocument15 pages2023 WARN Notice ListingsMasonNo ratings yet
- Brochure PerformanceDocument11 pagesBrochure PerformanceprabumnNo ratings yet
- Scribe America Final, Emergency DepartmentDocument41 pagesScribe America Final, Emergency DepartmentJulio CastilloNo ratings yet