You might also like
- Conscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantDocument84 pagesConscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantKhaled GharaibehNo ratings yet
- Conscious sedation techniques and risksDocument84 pagesConscious sedation techniques and risksKhaled GharaibehNo ratings yet
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- Nasta Pemicu 1 Gawat DaruratDocument21 pagesNasta Pemicu 1 Gawat DaruratThediDarmaWijayaNo ratings yet
- Medicine - Riley HarrisonDocument106 pagesMedicine - Riley HarrisonFiras AliNo ratings yet
- Managing Emergencies in Palliative & Geriatric CareDocument47 pagesManaging Emergencies in Palliative & Geriatric CareprashantNo ratings yet
- MG and MS Management GuideDocument2 pagesMG and MS Management GuideMarissa AsimNo ratings yet
- Medical Emergencies in OSDocument62 pagesMedical Emergencies in OSAditi RapriyaNo ratings yet
- ECT Clinical GuidelinesDocument50 pagesECT Clinical GuidelinesRhea Andrea Uy100% (1)
- Clinical Learning Session-Acute Coronary Syndromes Acs - 1Document31 pagesClinical Learning Session-Acute Coronary Syndromes Acs - 1api-611918048No ratings yet
- RenalPalliativeCarefinal Mar 2011Document5 pagesRenalPalliativeCarefinal Mar 2011Nexi anessaNo ratings yet
- Procedural Sedation in EDDocument41 pagesProcedural Sedation in EDadam NoheNo ratings yet
- Autonomic Neuropathy DMDocument49 pagesAutonomic Neuropathy DMJaskaran SinghNo ratings yet
- Catapres (Clonidine)Document2 pagesCatapres (Clonidine)Adrianne BazoNo ratings yet
- Yuli - Kuliah Blok 11 - Headache 2019Document66 pagesYuli - Kuliah Blok 11 - Headache 2019reshaNo ratings yet
- Spondylitis Tuberculosis and Cervical Paravertebral Abscess With Nutritional MarasmicDocument35 pagesSpondylitis Tuberculosis and Cervical Paravertebral Abscess With Nutritional MarasmicAntique HuntoyungoNo ratings yet
- Microsoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1Document23 pagesMicrosoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1api-19824701100% (1)
- Medically ComprmisedDocument73 pagesMedically Comprmisedhaitham192002No ratings yet
- Farmakologi ICUDocument54 pagesFarmakologi ICULin Phoponk100% (2)
- Tetanus FinalDocument45 pagesTetanus FinalSamra AhmadNo ratings yet
- Acute Lower Extremity Ischaemia (ALEXI) : Nadraj G NaidooDocument25 pagesAcute Lower Extremity Ischaemia (ALEXI) : Nadraj G NaidooVishad NaidooNo ratings yet
- General Anaesthesia in Acute Limb Ischemic Right R/ AmputationDocument20 pagesGeneral Anaesthesia in Acute Limb Ischemic Right R/ AmputationBangun Cholifa nusantaraNo ratings yet
- REGIONAL ANAESTHESIA IN PAEDIATRICSDocument83 pagesREGIONAL ANAESTHESIA IN PAEDIATRICSdennyramdhanNo ratings yet
- Acute Pain Management in Trauma PatientsDocument30 pagesAcute Pain Management in Trauma PatientsRafael BagusNo ratings yet
- NCM 116 Notes FinalsDocument44 pagesNCM 116 Notes Finalsyra capiliNo ratings yet
- Epilepsy: Dr. Hj. Meiti Frida, SP.S (K)Document53 pagesEpilepsy: Dr. Hj. Meiti Frida, SP.S (K)Hengki HaryandaNo ratings yet
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadisradiologi igdNo ratings yet
- Myasthenia Gravis Autoimmune Disorder ExplainedDocument30 pagesMyasthenia Gravis Autoimmune Disorder ExplainedMridula Mary AugustineNo ratings yet
- Headache: An Overview: Danish Ejaz BhattiDocument43 pagesHeadache: An Overview: Danish Ejaz BhattiPGHCNo ratings yet
- Unit 2 Anti Migraine and Drugs For Trigeminal Neuralgia Pharmacy-IIDocument38 pagesUnit 2 Anti Migraine and Drugs For Trigeminal Neuralgia Pharmacy-IIAsad MirajNo ratings yet
- Drug StudyDocument11 pagesDrug StudyJohn LesterNo ratings yet
- Cefaleas 2018Document87 pagesCefaleas 2018Anonimo DesconocidoNo ratings yet
- Neurology Paediatric ProtocolDocument44 pagesNeurology Paediatric ProtocolkirannesarajahNo ratings yet
- EpilepsyDocument73 pagesEpilepsyabenezer g/kirstosNo ratings yet
- HeadacheDocument36 pagesHeadacheabenezer g/kirstosNo ratings yet
- Check blood glucose level, administer insulin if required.Monitor vitals.Moderator: Let's move on to hypoglycemia nowDocument95 pagesCheck blood glucose level, administer insulin if required.Monitor vitals.Moderator: Let's move on to hypoglycemia nowVeena Goud100% (1)
- Metabolic EncephalopathyDocument22 pagesMetabolic Encephalopathytricia isabellaNo ratings yet
- Society For Obesity and Bariatric Anaesthesia: OS-MRS Calculator Tools - Farmacologiaclinica.infoDocument1 pageSociety For Obesity and Bariatric Anaesthesia: OS-MRS Calculator Tools - Farmacologiaclinica.infoHizami Norddin100% (2)
- Sedation & General Anesthesia: SMF Anestesiologi & Reanimasi, Intensive Care Rsud JayapuraDocument50 pagesSedation & General Anesthesia: SMF Anestesiologi & Reanimasi, Intensive Care Rsud JayapuraubayyumrNo ratings yet
- Gastrointestinal System: Antihistamine Half-Life: Onset: Peaks: DurationDocument3 pagesGastrointestinal System: Antihistamine Half-Life: Onset: Peaks: DurationsyerlyNo ratings yet
- Perioperative Pain ManagementDocument6 pagesPerioperative Pain ManagementAya RandallNo ratings yet
- Night Float Survival GuideDocument23 pagesNight Float Survival GuideNunu Mir100% (5)
- Diazepam CompiledDocument41 pagesDiazepam CompiledyayayanizaNo ratings yet
- Medicine - DrugsDocument101 pagesMedicine - Drugsvinaynagar1994No ratings yet
- DrugsDocument5 pagesDrugsnurse_nurseNo ratings yet
- Dönem 5 Ingilizce 02.04Document53 pagesDönem 5 Ingilizce 02.04Sarper Hikmet TAZENo ratings yet
- CNS: Drowsiness, Fatigue, Ataxia, Confusion, Paradoxic RageDocument4 pagesCNS: Drowsiness, Fatigue, Ataxia, Confusion, Paradoxic RageYanna N. CuakiNo ratings yet
- Pemicu 6 KGD DeniseDocument95 pagesPemicu 6 KGD DeniseVincent VandestyoNo ratings yet
- MS FTT S2 2019 PDFDocument37 pagesMS FTT S2 2019 PDFVannyNo ratings yet
- Epilepsy/ Seizures: Commonest Neurological DisorderDocument25 pagesEpilepsy/ Seizures: Commonest Neurological DisorderAlokh Saha RajNo ratings yet
- Droperidol (Inapsine)Document1 pageDroperidol (Inapsine)ENo ratings yet
- Neurologic and Neurosurgical Emergencies For Nursing StudentsDocument39 pagesNeurologic and Neurosurgical Emergencies For Nursing StudentsDr Ganeshgouda MajigoudraNo ratings yet
- Febrile Seizure and Epilepsy PDFDocument36 pagesFebrile Seizure and Epilepsy PDFMuhammad Amiro RasheeqNo ratings yet
- Characteristics of Thrombotic CVA: Transition To Neurological Nursing in The United States of AmericaDocument22 pagesCharacteristics of Thrombotic CVA: Transition To Neurological Nursing in The United States of AmericaAnn MavitiNo ratings yet
- Guillian Barre Syndrome NclexDocument15 pagesGuillian Barre Syndrome NclexKrishna SapkotaNo ratings yet
- Generalized Anxiety DisorderDocument3 pagesGeneralized Anxiety DisorderAhmad Syahmi YZNo ratings yet
- Guillain Barre SyndromeDocument16 pagesGuillain Barre SyndromeAgnes NesiaNo ratings yet
- Determine PH by PH Indicator and Universal IndicatorDocument3 pagesDetermine PH by PH Indicator and Universal IndicatorhaleelNo ratings yet
- Detailed Lesson Plan Boyle's LawDocument9 pagesDetailed Lesson Plan Boyle's LawTeacher Derick Daet86% (7)
- Catalog INSIZE - Instrumente de MasuraDocument32 pagesCatalog INSIZE - Instrumente de MasuraSculegero0% (1)
- Fire Crunch. M 08 Bushfire Attack Level BAL FZ TestedDocument3 pagesFire Crunch. M 08 Bushfire Attack Level BAL FZ TestedTimaiagNo ratings yet
- Calculation of Carbon Footprint: HouseDocument3 pagesCalculation of Carbon Footprint: HouseUmut ÇağırganNo ratings yet
- BMK PDFDocument8 pagesBMK PDFHuỳnh Minh SángNo ratings yet
- Lab ReportDocument9 pagesLab ReportQi Yi TanNo ratings yet
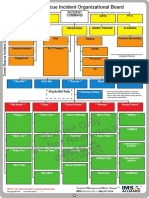
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- Factors to Consider in Reactor Design for Industrial ProcessesDocument3 pagesFactors to Consider in Reactor Design for Industrial Processesuma villashini100% (2)
- Hyundai-25 30 33L 35LN-9A19.01Rev.6 Eng-D4 PDFDocument20 pagesHyundai-25 30 33L 35LN-9A19.01Rev.6 Eng-D4 PDFVicente Antonio GonzalezNo ratings yet
- Rate Constant Determination 2Document8 pagesRate Constant Determination 2Divya UpadhyayNo ratings yet
- Enzyme ActivityDocument3 pagesEnzyme ActivityNabindra Ruwali100% (2)
- Philips HD5 enDocument5 pagesPhilips HD5 enmohamed boufasNo ratings yet
- Air Sentry - Energy Statement App 3 Dessicant and Filters PDFDocument20 pagesAir Sentry - Energy Statement App 3 Dessicant and Filters PDFEsteban Fernando Meza IbacetaNo ratings yet
- of The Blessedness of God.Document3 pagesof The Blessedness of God.itisme_angelaNo ratings yet
- Bronchiolitis A Practical Approach For The General RadiologistDocument42 pagesBronchiolitis A Practical Approach For The General RadiologistTara NareswariNo ratings yet
- GREEN AIR CONDITIONER Mechanical Presentation TopicsDocument9 pagesGREEN AIR CONDITIONER Mechanical Presentation TopicsCerin91No ratings yet
- Dip HenyDocument60 pagesDip HenyJinn Tanakrit HansuranantNo ratings yet
- Science: Pure Substances Vs MixturesDocument33 pagesScience: Pure Substances Vs MixturesElle Ma Rie100% (1)
- Preventive Maintenance Service Concept For SPACOM Product FamilyDocument27 pagesPreventive Maintenance Service Concept For SPACOM Product FamilyMiguel MarquesNo ratings yet
- Maximizing Area and Minimizing Costs with CalculusDocument18 pagesMaximizing Area and Minimizing Costs with Calculusanon_218576188No ratings yet
- Financing of New EnterpriseDocument8 pagesFinancing of New EnterpriseSunil BhamuNo ratings yet
- Rational Use of AntibioticsDocument35 pagesRational Use of AntibioticsRahul SharmaNo ratings yet
- Bernard BTB MIG GunsDocument8 pagesBernard BTB MIG GunsEdwin Mauricio Gallego OsorioNo ratings yet
- Fitness RX For Women - December 2013Document124 pagesFitness RX For Women - December 2013renrmrm100% (2)
- Problem Set 3_Cross-Text ConnectionDocument31 pagesProblem Set 3_Cross-Text Connectiontrinhdat11012010No ratings yet
- Solvent Extraction: Please Submit Question 4 For MarkingDocument3 pagesSolvent Extraction: Please Submit Question 4 For MarkingThembi Matebula100% (1)
- (New) Adjustable Voltage Power Supply 55 V - 20A High Power and Current - Automatic Fan On - OffDocument1 page(New) Adjustable Voltage Power Supply 55 V - 20A High Power and Current - Automatic Fan On - OffSek PyroNo ratings yet
- Assess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsDocument6 pagesAssess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsIJAR JOURNALNo ratings yet
- 2 1 Flash Klasa 6 Mod 1b Test ExtendedDocument4 pages2 1 Flash Klasa 6 Mod 1b Test ExtendedMonika Ciepłuch-Jarema100% (1)