You might also like
- Presentation of Godrej CompanyDocument15 pagesPresentation of Godrej CompanyRiya TopiwalaNo ratings yet
- Common Gynecologic ProceduresDocument55 pagesCommon Gynecologic ProceduresQurrataini IbanezNo ratings yet
- Anti Inflammatory DietDocument6 pagesAnti Inflammatory DietHW GomarNo ratings yet
- WISE Journal Volume 6, No. 1 (Spring, 2017)Document108 pagesWISE Journal Volume 6, No. 1 (Spring, 2017)Vas RaNo ratings yet
- Plastic Surgery: Understanding Abdominoplasty and LiposuctionDocument14 pagesPlastic Surgery: Understanding Abdominoplasty and LiposuctiondoctorbanNo ratings yet
- Modular ArithmeticDocument12 pagesModular ArithmeticJavadd KilamNo ratings yet
- Business Model Canvas: Maria Saeed KhattakDocument19 pagesBusiness Model Canvas: Maria Saeed KhattakWhatsapp StoriesNo ratings yet
- Alexanders Care of The Patient in Surgery Rothrock 16th Edition Test BankDocument9 pagesAlexanders Care of The Patient in Surgery Rothrock 16th Edition Test Bankjoshuabakergpctsonbwj100% (39)
- Abdominal Access TechniquesDocument7 pagesAbdominal Access TechniquesdrmarcsNo ratings yet
- Life Span Development Santrock 14th Edition Test BankDocument37 pagesLife Span Development Santrock 14th Edition Test Bankjosephwatsontsypjrcfki100% (48)
- Ureteral Injuries Obgyn-1Document53 pagesUreteral Injuries Obgyn-1mooni2009No ratings yet
- R HemicolectomyDocument15 pagesR Hemicolectomyrwilah100% (1)
- Abdominoperineal Resection MilesDocument17 pagesAbdominoperineal Resection MilesHugoNo ratings yet
- Chapter 41 - Roux-en-Y Gastric Bypass, LaparoscopicDocument4 pagesChapter 41 - Roux-en-Y Gastric Bypass, LaparoscopicCharbel AounNo ratings yet
- Case ReportDocument5 pagesCase Report260778No ratings yet
- Jurnal Hernia VentralisDocument10 pagesJurnal Hernia VentralisMusdalipaNo ratings yet
- Full Alexanders Care of The Patient in Surgery 14Th Edition Rothrock Test Bank Online PDF All ChapterDocument34 pagesFull Alexanders Care of The Patient in Surgery 14Th Edition Rothrock Test Bank Online PDF All Chapterflorisromcnicn100% (3)
- 2014 172 0 Retroperitoneal and Retrograde Total Laparoscopic Hysterectomy As A Standard Treatment in A Community Hospital 97 101 1Document5 pages2014 172 0 Retroperitoneal and Retrograde Total Laparoscopic Hysterectomy As A Standard Treatment in A Community Hospital 97 101 1Sarah MuharomahNo ratings yet
- Full Alexanders Care of The Patient in Surgery 15Th Edition Rothrock Test Bank Online PDF All ChapterDocument32 pagesFull Alexanders Care of The Patient in Surgery 15Th Edition Rothrock Test Bank Online PDF All Chapterflorisromcnicn100% (4)
- Minimallyinvasive Esophagectomyforbenign Disease: Blair A. JobeDocument10 pagesMinimallyinvasive Esophagectomyforbenign Disease: Blair A. JobeYacine Tarik AizelNo ratings yet
- Radical Hysterectomy With Pelvic Lymphadenectomy - Indications TeDocument12 pagesRadical Hysterectomy With Pelvic Lymphadenectomy - Indications TexmatisaNo ratings yet
- Alexanders Care of The Patient in Surgery 14th Edition Rothrock Test Bank Full Chapter PDFDocument27 pagesAlexanders Care of The Patient in Surgery 14th Edition Rothrock Test Bank Full Chapter PDFwilliamboydnatcwzpofb100% (17)
- Research ArticleDocument9 pagesResearch ArticleJuliánPitalúaNo ratings yet
- Case Report: Laparoscopic Repair of Postoperative Perineal HerniaDocument3 pagesCase Report: Laparoscopic Repair of Postoperative Perineal HerniacleybismarNo ratings yet
- Umbilical Hernia Repair MedscapeDocument5 pagesUmbilical Hernia Repair MedscapeVanessa Au YongNo ratings yet
- Ms AJCRS 99757Document6 pagesMs AJCRS 99757Cesar DominguezNo ratings yet
- Tan-Bianchi Procedure and Modifications August2004Document37 pagesTan-Bianchi Procedure and Modifications August2004Rizky Syawaluddin DjamalNo ratings yet
- Surgical Endoscopy Oct.1997Document87 pagesSurgical Endoscopy Oct.1997Saibo BoldsaikhanNo ratings yet
- Jurnal Windi 2Document6 pagesJurnal Windi 2Fiella Ardhilia NuchnumNo ratings yet
- Yeyunos LaparosDocument7 pagesYeyunos LaparosFlipNo ratings yet
- Laparoscopic Surgery in Gynaecologic OncologyDocument7 pagesLaparoscopic Surgery in Gynaecologic OncologyManan BoobNo ratings yet
- International Journal of Surgery Case ReportsDocument3 pagesInternational Journal of Surgery Case Reportshussein_faourNo ratings yet
- Preventing Urinary Tract Injury at The Time of HysterectomyDocument7 pagesPreventing Urinary Tract Injury at The Time of HysterectomyjayeshEPGPNo ratings yet
- Radical Hysterectomy With Pelvic Lymphadenectomy: Indications, Technique, and ComplicationsDocument10 pagesRadical Hysterectomy With Pelvic Lymphadenectomy: Indications, Technique, and ComplicationsAzura MotovlogNo ratings yet
- Sleeve-Gastrectomy 2011 BrethauerDocument15 pagesSleeve-Gastrectomy 2011 BrethauerDavid Schnettler RodriguezNo ratings yet
- Test Bank Alexanders Care of The Patient in Surgery 16th Edition Rothrock DownloadDocument9 pagesTest Bank Alexanders Care of The Patient in Surgery 16th Edition Rothrock Downloadlaurafloresejzawnptxr100% (30)
- Williams2013 Article LaparoscopicManagementOfHighTrDocument3 pagesWilliams2013 Article LaparoscopicManagementOfHighTrVishnu priya kokkulaNo ratings yet
- Principles of Laparoscopic Surgery.Document1 pagePrinciples of Laparoscopic Surgery.abinash chihnaraNo ratings yet
- PBEI Incisional Hernia PDFDocument31 pagesPBEI Incisional Hernia PDFAdi WijayantoNo ratings yet
- AppendectomyDocument6 pagesAppendectomyRENOBLAS, GLORYLEIN MARNo ratings yet
- Total Abdominal Hysterectomy Bilateral SaphingoDocument7 pagesTotal Abdominal Hysterectomy Bilateral SaphingoAndrea BroccoliNo ratings yet
- Incisional HerniaDocument9 pagesIncisional HerniaAdelina Martinica0% (1)
- Ciencia e Technica Omentum Overlay PDFDocument10 pagesCiencia e Technica Omentum Overlay PDFAlin MihetiuNo ratings yet
- AppendectomyDocument7 pagesAppendectomyLeis FatwaNo ratings yet
- Lumbar Hernia: Case ReportDocument2 pagesLumbar Hernia: Case ReportGabriela SanhuezaNo ratings yet
- Pphsurgical 171108173433Document40 pagesPphsurgical 171108173433FatimaMalazaiNo ratings yet
- Alexanders Care of The Patient in Surgery 15th Edition Rothrock Test Bank Full Chapter PDFDocument30 pagesAlexanders Care of The Patient in Surgery 15th Edition Rothrock Test Bank Full Chapter PDFwilliamboydnatcwzpofb100% (13)
- Successful Use of Laparoscopic Myomectomy To Remove A Giant Uterine Myoma A Case ReportDocument4 pagesSuccessful Use of Laparoscopic Myomectomy To Remove A Giant Uterine Myoma A Case ReportnicabiNo ratings yet
- Abdelhameed Et Al (June 2019)Document6 pagesAbdelhameed Et Al (June 2019)drpklalNo ratings yet
- Modified Manchester de BoerDocument7 pagesModified Manchester de BoerGustavo flores quispeNo ratings yet
- Laparoscopic Entry TechniquesDocument9 pagesLaparoscopic Entry TechniquesDougNo ratings yet
- Laparoscopic Right Radical Hemicolectomy: Howidoit?Document4 pagesLaparoscopic Right Radical Hemicolectomy: Howidoit?pingusNo ratings yet
- Abdominal Mass Removal: Hugh H. Allen, M.DDocument6 pagesAbdominal Mass Removal: Hugh H. Allen, M.DAbbyKristekNo ratings yet
- Dimatingcal, Warda M. BSN14D Group 24 (Laparoscopic Feeding Jejunostomy)Document18 pagesDimatingcal, Warda M. BSN14D Group 24 (Laparoscopic Feeding Jejunostomy)WARDA DIMATINGCALNo ratings yet
- 3 BaruDocument17 pages3 BaruAnditha Namira RSNo ratings yet
- Chilaiditi Syndrome About A Case: The Experience of The Medical Clinic The Stars of BamakoDocument6 pagesChilaiditi Syndrome About A Case: The Experience of The Medical Clinic The Stars of BamakoIJAR JOURNALNo ratings yet
- Abdominal Surgeries in PregnancyDocument10 pagesAbdominal Surgeries in PregnancyNoel QuintonNo ratings yet
- 1 s2.0 S0065341116000038 MainDocument12 pages1 s2.0 S0065341116000038 MainFlorin AchimNo ratings yet
- Final Version Surgery AssignmentDocument28 pagesFinal Version Surgery AssignmentAyele AsefaNo ratings yet
- Surgery News Summer 2012 Newsletter - Spotlight On Colorectal SurgeryDocument4 pagesSurgery News Summer 2012 Newsletter - Spotlight On Colorectal SurgeryContinuum Hospitals of New YorkNo ratings yet
- McKeown EsophagectomyDocument9 pagesMcKeown EsophagectomyDa JunNo ratings yet
- Umbilicalherniarepair TechniqueDocument9 pagesUmbilicalherniarepair Techniqueanz_4191No ratings yet
- Glauser Et Al (Sept 2019)Document7 pagesGlauser Et Al (Sept 2019)drpklalNo ratings yet
- Original Article: 360 Degree Subannular Tympanoplasty: A Retrospective StudyDocument7 pagesOriginal Article: 360 Degree Subannular Tympanoplasty: A Retrospective StudyAkanshaNo ratings yet
- Maq 2Document5 pagesMaq 2eduardoNo ratings yet
- Pathfit 3 Module Chapter 2Document18 pagesPathfit 3 Module Chapter 2Marc BorcilloNo ratings yet
- Gender Stereotypes Discussion Questions PDFDocument2 pagesGender Stereotypes Discussion Questions PDFHypeLensNo ratings yet
- Third Quarter Module Time Frame MgsDocument2 pagesThird Quarter Module Time Frame MgsCHRISTOPHER JOHN LIVINANo ratings yet
- Prueba Corta Modales de Obligación InglésDocument3 pagesPrueba Corta Modales de Obligación InglésGLEDYS HERNANDEZNo ratings yet
- Tlisw CL 10 English Term 1 Student Portfolio 22-23Document2 pagesTlisw CL 10 English Term 1 Student Portfolio 22-23Darsh AgarwalNo ratings yet
- WORLD THINKING DAY 2022 ProposalDocument9 pagesWORLD THINKING DAY 2022 ProposalPerlita CarpenteroNo ratings yet
- Drowning PDFDocument7 pagesDrowning PDFAditya Chandra ForestaNo ratings yet
- 1 Preparing Persuasive MessagesDocument14 pages1 Preparing Persuasive MessagesAmit GiriNo ratings yet
- Results For Sai Teja Traders - Rajahmundry - ZonalinfoDocument4 pagesResults For Sai Teja Traders - Rajahmundry - ZonalinfoManoj Digi LoansNo ratings yet
- ICT LP (AutoRecovered)Document7 pagesICT LP (AutoRecovered)Richel Madara NideaNo ratings yet
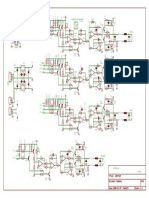
- Electrical EngineeringDocument200 pagesElectrical EngineeringEhsan Elahi BashirNo ratings yet
- Every Child Matters A Practical Guide For Teachers PDFDocument2 pagesEvery Child Matters A Practical Guide For Teachers PDFBarbaraNo ratings yet
- Lecture 4. Theories of International TradeDocument39 pagesLecture 4. Theories of International TradeBorn HyperNo ratings yet
- 150 515Document1 page150 515Zeljko TomicNo ratings yet
- Kelas 8 Present Continous - 083001Document3 pagesKelas 8 Present Continous - 083001RachiyopaaNo ratings yet
- Ajinomoto - SSFW M544 - Facial Wash - AMISOFT Base Paste Type Facial WashDocument1 pageAjinomoto - SSFW M544 - Facial Wash - AMISOFT Base Paste Type Facial Washmarcel leeNo ratings yet
- DUI INstall Manual 232ci - 6516-3Document2 pagesDUI INstall Manual 232ci - 6516-3EdwinNo ratings yet
- Tom Coffing TD BasicsDocument58 pagesTom Coffing TD Basicsypswamy3631No ratings yet
- Wax Patterns in FPDDocument39 pagesWax Patterns in FPDMihaela VasiliuNo ratings yet
- English Grammar: Prepositions of TimeDocument3 pagesEnglish Grammar: Prepositions of Timecavil2006No ratings yet
- 105 Mid-Week AssignmentDocument4 pages105 Mid-Week AssignmentSandhya SharmaNo ratings yet
- 8 - Problem Reduction SearchDocument31 pages8 - Problem Reduction SearchArchana PanwarNo ratings yet
- Rotc Reviewer For Final ExamDocument33 pagesRotc Reviewer For Final ExamKaiNo ratings yet
- Catalysis & Catalysts - Impregnation and Reaction MechanismDocument19 pagesCatalysis & Catalysts - Impregnation and Reaction MechanismZamri Fadilah IINo ratings yet