You might also like
- Hesi Hints MaternityDocument4 pagesHesi Hints MaternityThomas Stewart91% (11)
- Active Management of Normal LabourDocument16 pagesActive Management of Normal LabourjincyneeleshNo ratings yet
- Technical Documentation IPM: Savina 300 Intensive Care VentilatorDocument166 pagesTechnical Documentation IPM: Savina 300 Intensive Care VentilatorhoudaNo ratings yet
- NCM 102 Power and PsycheDocument13 pagesNCM 102 Power and Psychelarissedeleon100% (1)
- Stage 1Document10 pagesStage 1JosephNawenNo ratings yet
- Stages of Labor NSG MGTDocument3 pagesStages of Labor NSG MGTMelDred Cajes BolandoNo ratings yet
- Nursing Care During LaborDocument19 pagesNursing Care During LaborBaniwas Marie AgnesNo ratings yet
- Normal Labour: PRESENTED BY DR Tsitsi Vimbayi ChatoraDocument13 pagesNormal Labour: PRESENTED BY DR Tsitsi Vimbayi ChatoraChatora Tsitsi VimbayiNo ratings yet
- Management of The First Stage of Labour LectureDocument48 pagesManagement of The First Stage of Labour LectureJSeashark100% (3)
- 11 - Management of Labour & Fetal AssessmenDocument77 pages11 - Management of Labour & Fetal AssessmenGreen ArrowNo ratings yet
- Hesi Review For MaternityDocument29 pagesHesi Review For MaternitySteam Lc86% (21)
- Labour Presentation ObsDocument48 pagesLabour Presentation ObsVera BannorNo ratings yet
- Management of Normal LabourDocument37 pagesManagement of Normal LabourGlucose DRglucoseNo ratings yet
- Obgyn SL1Document39 pagesObgyn SL1mustafe omarNo ratings yet
- Postnatal CareDocument19 pagesPostnatal Carejomarie gamiao0% (1)
- Postpartum Physical AssessmentDocument60 pagesPostpartum Physical Assessmentalmyr_rimandoNo ratings yet
- Neonatal ResuscitationDocument51 pagesNeonatal ResuscitationAbdulkadir HasanNo ratings yet
- Dec2012nletips MCHN 121021230343 Phpapp01 PDFDocument7 pagesDec2012nletips MCHN 121021230343 Phpapp01 PDFJessamine Rochelle Reyes EsbertoNo ratings yet
- Stages of LaborDocument5 pagesStages of LaborL Rean Carmelle MAGALLONES100% (1)
- Prolonged LabourDocument3 pagesProlonged Labourgeorgeloto12No ratings yet
- Stages of LaborDocument15 pagesStages of LaborJune DumdumayaNo ratings yet
- Principles of Postpartum CareDocument2 pagesPrinciples of Postpartum CareZaire DylanNo ratings yet
- Labor WatchDocument35 pagesLabor WatchLawrence Steve Beronio MapaNo ratings yet
- Postpartum Physical AssessmentDocument60 pagesPostpartum Physical AssessmentJhgrace Mary Pacaña Gallo100% (1)
- Low Risk Labour CareDocument11 pagesLow Risk Labour CareYwagar YwagarNo ratings yet
- Presentasi Partus Spontan Pervaginam - PPT (Compatibility Mode)Document50 pagesPresentasi Partus Spontan Pervaginam - PPT (Compatibility Mode)Ahmed MawardiNo ratings yet
- NCM 107 Lecture - Nursing Diagnosis - Maternal (Midterm)Document38 pagesNCM 107 Lecture - Nursing Diagnosis - Maternal (Midterm)conahs nasugbuNo ratings yet
- Stages of LaborDocument3 pagesStages of LaborShyla mayNo ratings yet
- Resuscitation Nisha 1Document64 pagesResuscitation Nisha 1Nisha Chaudhary LamberdarNo ratings yet
- Physiology of 1st Stage of LaborDocument134 pagesPhysiology of 1st Stage of LaborVijith.V.kumar50% (2)
- Labor Delivery 1Document29 pagesLabor Delivery 1Elmer DaquilañeaNo ratings yet
- 39 Neonatal ResuscitationDocument38 pages39 Neonatal ResuscitationbenNo ratings yet
- Mechanism of LaborDocument84 pagesMechanism of LaborRavi Kant100% (1)
- Clinical Course and Management of First and SecondDocument66 pagesClinical Course and Management of First and SecondEkawali Sharma100% (1)
- Newborn Resuscitation Programme NRPDocument52 pagesNewborn Resuscitation Programme NRPHala BahaaNo ratings yet
- JINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioDocument13 pagesJINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioJashtine JingcoNo ratings yet
- Stages of Labor: Dela Cruz, Dineros, DimaporoDocument25 pagesStages of Labor: Dela Cruz, Dineros, DimaporoEvelyn MedinaNo ratings yet
- New Born ResuscitationDocument34 pagesNew Born ResuscitationPAUL NDEKINo ratings yet
- 4 Stages of LaborDocument15 pages4 Stages of LaborFelaih Binasoy Dela CruzNo ratings yet
- Care During First Stage of LabourDocument6 pagesCare During First Stage of LabourSabita PaudelNo ratings yet
- Labor and DeliveryDocument10 pagesLabor and DeliveryDelia Ramirez0% (1)
- Partograph - Used When The Mother Is About 4 CM Cervical Dilatation - The Updated Usage of It According To TheDocument5 pagesPartograph - Used When The Mother Is About 4 CM Cervical Dilatation - The Updated Usage of It According To TheGenierose YantoNo ratings yet
- NCM 109 DR and Nursery 2023 1Document38 pagesNCM 109 DR and Nursery 2023 1Patricia CaladoNo ratings yet
- Mother Baby Final Exam ReviewDocument14 pagesMother Baby Final Exam ReviewAngelina mendezNo ratings yet
- Labor & DeliveryDocument9 pagesLabor & DeliveryfriaslenemoNo ratings yet
- Antepartum Fetal Assessment 2018Document39 pagesAntepartum Fetal Assessment 2018amena mahmoudNo ratings yet
- Normal Labor - AMTSLDocument27 pagesNormal Labor - AMTSLNational Child Health Resource Centre (NCHRC)No ratings yet
- Esarean Ction: Cadalin, Fremelen Rose Cedamon, CarloDocument18 pagesEsarean Ction: Cadalin, Fremelen Rose Cedamon, CarloMonette Abalos MendovaNo ratings yet
- Signs of LaborDocument40 pagesSigns of LaborDominicSavioNo ratings yet
- Assigment VDocument4 pagesAssigment VJoey ParkNo ratings yet
- Helping Baby To BreathDocument49 pagesHelping Baby To BreathmohdmaghyrehNo ratings yet
- Failure To Initiate and Sustain Breathing at Birth Is Called Birth AsphyxiaDocument21 pagesFailure To Initiate and Sustain Breathing at Birth Is Called Birth AsphyxiaNishaThakuriNo ratings yet
- Essential Newborn CareDocument5 pagesEssential Newborn CareJig PirameNo ratings yet
- Skills Building Maternal and Child Care: Prepared By: Angeli Joy V. MontonDocument61 pagesSkills Building Maternal and Child Care: Prepared By: Angeli Joy V. MontonboinkjilijoyNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Advice To Wives On The Management Of Themselves, During The Periods Of Pregnancy, Labour And SucklingFrom EverandAdvice To Wives On The Management Of Themselves, During The Periods Of Pregnancy, Labour And SucklingNo ratings yet
- Getting Pregnant Faster: Step-By-Step Guide To Achieving PregnancyFrom EverandGetting Pregnant Faster: Step-By-Step Guide To Achieving PregnancyNo ratings yet
- Dental Management of the Pregnant PatientFrom EverandDental Management of the Pregnant PatientChristos A. SkouterisNo ratings yet
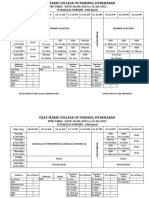
- Time Table-I - IV Year B.SC 2023Document36 pagesTime Table-I - IV Year B.SC 2023priyagerardNo ratings yet
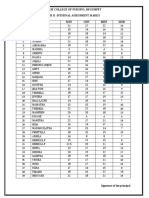
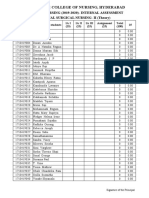
- 17 Batch I.A MarksDocument1 page17 Batch I.A MarkspriyagerardNo ratings yet
- Adoption 150109001206 Conversion Gate01Document44 pagesAdoption 150109001206 Conversion Gate01priyagerardNo ratings yet
- Letter Seeking Experts For Content Validity of ToolDocument1 pageLetter Seeking Experts For Content Validity of ToolpriyagerardNo ratings yet
- 4304 - M.Sc. - Community - Health - Nursing ImportantDocument84 pages4304 - M.Sc. - Community - Health - Nursing ImportantpriyagerardNo ratings yet
- BLINDNESSDocument24 pagesBLINDNESSpriyagerardNo ratings yet
- 17 Batch AttendanceDocument3 pages17 Batch AttendancepriyagerardNo ratings yet
- 3RD Yr Time Table, 2ND Year and 4TH Year Time Table From 07-2-22 To 12-2-22Document4 pages3RD Yr Time Table, 2ND Year and 4TH Year Time Table From 07-2-22 To 12-2-22priyagerardNo ratings yet
- AMOEBIASISDocument31 pagesAMOEBIASISpriyagerard100% (1)
- GNM Vol I Community Health Nursing Part 2 MinDocument446 pagesGNM Vol I Community Health Nursing Part 2 MinpriyagerardNo ratings yet
- Abdelfattah Monged Selim - SporotrichosisDocument14 pagesAbdelfattah Monged Selim - SporotrichosispriyagerardNo ratings yet
- 2 2018 12 15!09 27 25 AmDocument24 pages2 2018 12 15!09 27 25 AmNatalia CaramanNo ratings yet
- 2020 IA 3rd YearDocument7 pages2020 IA 3rd YearpriyagerardNo ratings yet
- Nursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)Document35 pagesNursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)priyagerardNo ratings yet
- International Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikDocument56 pagesInternational Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikpriyagerardNo ratings yet
- Annexure For Dissertations Synopsis SubmissionDocument2 pagesAnnexure For Dissertations Synopsis SubmissionpriyagerardNo ratings yet
- Med Term 2 MTDocument9 pagesMed Term 2 MTpriyagerardNo ratings yet
- Pituitary GlandDocument34 pagesPituitary GlandpriyagerardNo ratings yet
- 0 EndocrinedisordersseminarDocument52 pages0 EndocrinedisordersseminarpriyagerardNo ratings yet
- Anatomy and Physiology Tonsils: MRS. Priya GerardDocument11 pagesAnatomy and Physiology Tonsils: MRS. Priya GerardpriyagerardNo ratings yet
- College Report 2015Document120 pagesCollege Report 2015priyagerardNo ratings yet
- S. No. ContentDocument167 pagesS. No. ContentpriyagerardNo ratings yet
- Pathology Notes HemalathaDocument117 pagesPathology Notes HemalathapriyagerardNo ratings yet
- UNIT PLAN I CHN IDocument7 pagesUNIT PLAN I CHN IpriyagerardNo ratings yet
- CHN I & Ii Course PlanDocument17 pagesCHN I & Ii Course PlanpriyagerardNo ratings yet
- Body Cavity FluidsDocument29 pagesBody Cavity FluidspriyagerardNo ratings yet
- Second Year M.SC Nursing Degree Examinations - September 2016Document1 pageSecond Year M.SC Nursing Degree Examinations - September 2016priyagerardNo ratings yet
- Unit Iv Body Fluid AnalysisDocument8 pagesUnit Iv Body Fluid AnalysispriyagerardNo ratings yet
- Unit Iv: Body Fluid AnalysisDocument41 pagesUnit Iv: Body Fluid AnalysispriyagerardNo ratings yet
- Report On Cancer Run: "Race For Grace"Document2 pagesReport On Cancer Run: "Race For Grace"priyagerardNo ratings yet
- Zinc Silicate or Zinc Epoxy As The Preferred High Performance PrimerDocument10 pagesZinc Silicate or Zinc Epoxy As The Preferred High Performance Primerbabis1980100% (1)
- Ranitidine + OndansetronDocument7 pagesRanitidine + OndansetronAllicia PutriNo ratings yet
- Fawwaz Muhammad X-Ipa 1: 1. Who Is The Main Character of The Story? 2. When Did It Happen?Document3 pagesFawwaz Muhammad X-Ipa 1: 1. Who Is The Main Character of The Story? 2. When Did It Happen?Abbas AminuNo ratings yet
- JECFA Carrageenan MonographDocument5 pagesJECFA Carrageenan MonographSurya SaputraNo ratings yet
- Problems Associated With The Use of Compaction Grout For SinkholeDocument4 pagesProblems Associated With The Use of Compaction Grout For SinkholeVetriselvan ArumugamNo ratings yet
- Aaos PDFDocument4 pagesAaos PDFWisnu CahyoNo ratings yet
- ISO 27001 MindmapsDocument6 pagesISO 27001 MindmapsYagnesh VyasNo ratings yet
- Quality Control Argex 0032/32.50.15.08 4/10 MM EN 13055: EN 15732 NL BSB K73820/01 (1/01/2004)Document1 pageQuality Control Argex 0032/32.50.15.08 4/10 MM EN 13055: EN 15732 NL BSB K73820/01 (1/01/2004)joe briffaNo ratings yet
- Account Transfer Form: Fax Cover SheetDocument6 pagesAccount Transfer Form: Fax Cover SheetJitendra SharmaNo ratings yet
- EpidemiologyDocument26 pagesEpidemiologymohildasadiaNo ratings yet
- Offshore Drilling Operation in East Indonesia Oil and Gas FieldsDocument3 pagesOffshore Drilling Operation in East Indonesia Oil and Gas FieldsMuhammad Galih Eko SaputroNo ratings yet
- Logiq e BT11 User Guide PDFDocument192 pagesLogiq e BT11 User Guide PDFprofesorbartolomeo0% (1)
- Cation Ion Exchange CapacityDocument1 pageCation Ion Exchange CapacityGopal MallickNo ratings yet
- 10 Achievement ChartDocument3 pages10 Achievement ChartLyka ollerasNo ratings yet
- Homework #3Document2 pagesHomework #3RobbieNo ratings yet
- ASTM C309: Do Liquid Hardeners Meet This Standard?Document2 pagesASTM C309: Do Liquid Hardeners Meet This Standard?Kishore Nayak kNo ratings yet
- Phaser 3250 Service Manual 0106 2010Document334 pagesPhaser 3250 Service Manual 0106 2010Terry BogardNo ratings yet
- Current Issues On Construction Project ManagementDocument2 pagesCurrent Issues On Construction Project ManagementJoyce Abegail De PedroNo ratings yet
- Patoflow DMDocument2 pagesPatoflow DMAngel da CostaNo ratings yet
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Siklus Biogeokimia - Retensi NutrienDocument24 pagesSiklus Biogeokimia - Retensi NutrienPutri Nur Fadhilah YasharNo ratings yet
- Hitec 8888Z Atf C4 & To4 - TDSDocument2 pagesHitec 8888Z Atf C4 & To4 - TDSPranit More Arabian Petroleum LimitedNo ratings yet
- Chapter 3 - Assessment of PostureDocument31 pagesChapter 3 - Assessment of Posturehis.thunder122No ratings yet
- Substation Basic PDFDocument6 pagesSubstation Basic PDFSaraswatapalitNo ratings yet
- Nexgard For Dogs and Puppies Free 2 Day ShippingDocument1 pageNexgard For Dogs and Puppies Free 2 Day Shippinglyly23748No ratings yet
- 2022 EDCS Weekly Surveillance Report No 5Document22 pages2022 EDCS Weekly Surveillance Report No 5Aesthetics MinNo ratings yet
- CORONADocument25 pagesCORONAMohammedNo ratings yet
- Anexate IVsolnDocument7 pagesAnexate IVsolnJelena Obrenovic StankovicNo ratings yet
- Self Esteem and AdjustmentDocument22 pagesSelf Esteem and AdjustmentJan IrishNo ratings yet