You might also like
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Terminology CHNDocument4 pagesTerminology CHNKailash NagarNo ratings yet
- Lecture 10 Protein Energy Malnutrition (PEM)Document26 pagesLecture 10 Protein Energy Malnutrition (PEM)jaish8904100% (1)
- Disposable Delivery KitDocument13 pagesDisposable Delivery Kitapi-3823785100% (1)
- Anatomy and Physiology of GallbladderDocument15 pagesAnatomy and Physiology of GallbladderIkea Balhon100% (1)
- Common Communicable DiseasesDocument13 pagesCommon Communicable DiseasesSanthosh.S.U100% (1)
- Diarrhoeal Diseases in NepalDocument86 pagesDiarrhoeal Diseases in NepalBinayaNo ratings yet
- Sigmoid Volvulus: Rashid Swed S. (Md4) Mwanyingili John A. (Md3)Document46 pagesSigmoid Volvulus: Rashid Swed S. (Md4) Mwanyingili John A. (Md3)Amani Twaha MsemakweliNo ratings yet
- Assessing Newborns EffectivelyDocument35 pagesAssessing Newborns EffectivelyBaldwin Hamzcorp Hamoonga100% (1)
- Hookworm Diseases: (Ancylostomiasis /Miner'S Disease/Egyptian Chlorisis)Document21 pagesHookworm Diseases: (Ancylostomiasis /Miner'S Disease/Egyptian Chlorisis)Mel Izhra N. Margate100% (1)
- National Polio Eradication ProgramDocument36 pagesNational Polio Eradication Programayushi rainaNo ratings yet
- Managing Diarrhea in Under-5sDocument15 pagesManaging Diarrhea in Under-5skuruvagadda sagarNo ratings yet
- Chicken Pox and Herpes ZosterfinalDocument31 pagesChicken Pox and Herpes ZosterfinalBinayaNo ratings yet
- Case Management of Ari at PHC LevelDocument29 pagesCase Management of Ari at PHC Levelapi-3823785No ratings yet
- WVSU Nursing Process for Step-Down NICUDocument14 pagesWVSU Nursing Process for Step-Down NICUCharles Jebb Belonio JuanitasNo ratings yet
- MumpsDocument11 pagesMumpscasandra moranteNo ratings yet
- On National GoalsDocument68 pagesOn National Goalssreedhar muthyala0% (2)
- Pulse PolioDocument99 pagesPulse PolioChulbul Pandey100% (1)
- BSC Nursing Guide: Tonsillitis and AdenoiditisDocument41 pagesBSC Nursing Guide: Tonsillitis and AdenoiditisYAMINIPRIYANNo ratings yet
- Dengue Health TalkDocument20 pagesDengue Health TalkAnnamalai MNo ratings yet
- Epidemiology of Non-Communicable DiseasesDocument16 pagesEpidemiology of Non-Communicable DiseasesAparna AbyNo ratings yet
- Food HygieneDocument31 pagesFood Hygienehemihema100% (1)
- Nursing Management of Patients Occupational and Industrial DisordersDocument11 pagesNursing Management of Patients Occupational and Industrial DisordersNandini VermaNo ratings yet
- PRIMARY HEALTH CARE - IMMUNIZATIONDocument24 pagesPRIMARY HEALTH CARE - IMMUNIZATIONAhmed Azeez100% (1)
- Community Health Assessment Form 1Document4 pagesCommunity Health Assessment Form 1Vrent Mica SilotNo ratings yet
- TyphoidDocument10 pagesTyphoidpeterjongNo ratings yet
- Breast Self ExaminationDocument13 pagesBreast Self ExaminationChanDa DasNo ratings yet
- Hookworm Disease: Ancylostoma Duodenale-Are Anthropophilic Human Hookworms Transmitted From Infected SoilDocument5 pagesHookworm Disease: Ancylostoma Duodenale-Are Anthropophilic Human Hookworms Transmitted From Infected SoilBrix Valdriz100% (1)
- Diarrhea: DefinitionDocument13 pagesDiarrhea: Definitionudaybujji100% (1)
- Disease PEMDocument16 pagesDisease PEMMeena KoushalNo ratings yet
- National iodine deficiency disorder programme aims to reduce goitre prevalenceDocument6 pagesNational iodine deficiency disorder programme aims to reduce goitre prevalencemalathi100% (1)
- SCABIESDocument14 pagesSCABIESNom Kumar Naik Rathod100% (1)
- Feeding Helpless Patient - Types Od Diet and Factors Affecting Dietary PatternDocument12 pagesFeeding Helpless Patient - Types Od Diet and Factors Affecting Dietary PatternKenje Kate Agripo0% (4)
- Cholera & DysenteryDocument28 pagesCholera & DysenterySherbaz Sheikh100% (1)
- Epidemilogy Measurment MethodsDocument100 pagesEpidemilogy Measurment MethodsKailash NagarNo ratings yet
- CASE PRESENTATION ON ANORECTAL MALFORMATIONS (ARMsDocument39 pagesCASE PRESENTATION ON ANORECTAL MALFORMATIONS (ARMsSomyee PachuauNo ratings yet
- Ascariasis: Roundworm Ascaris LumbricoidesDocument18 pagesAscariasis: Roundworm Ascaris LumbricoidesSuneel Kumar PrajapatiNo ratings yet
- Wk1 - Introduction To Nursing ResearchDocument37 pagesWk1 - Introduction To Nursing ResearchSophia GraziellaNo ratings yet
- Marasmus PresentationDocument29 pagesMarasmus PresentationApriany Cordias Arlita Silalahi100% (2)
- UNFPADocument17 pagesUNFPAshipra arora50% (2)
- Yaws Eradication ProgrammeDocument82 pagesYaws Eradication ProgrammeAparna Aby50% (2)
- On LeukemiaDocument28 pagesOn LeukemiaMeena Koushal100% (1)
- Esophageal ObstructionDocument18 pagesEsophageal ObstructionArun Murali50% (2)
- Stomal Therapy GuideDocument2 pagesStomal Therapy Guideসায়ন্তন দত্ত100% (1)
- Pre - Operative and Post Operative CareDocument52 pagesPre - Operative and Post Operative CareChonnetteAshlynKingNo ratings yet
- Sister Nivedita Government Nursing College, Igmc Shimla: Submitted To Submitted byDocument6 pagesSister Nivedita Government Nursing College, Igmc Shimla: Submitted To Submitted byshivaniNo ratings yet
- Neonatal SepsisDocument63 pagesNeonatal SepsisDemewoz Fikir100% (2)
- Presentation On Blood DisordersDocument122 pagesPresentation On Blood Disordersvarshasharma05No ratings yet
- Gastritis PDFDocument15 pagesGastritis PDFSangeeta BSR100% (2)
- Management of patients with meningitis and encephalitisDocument71 pagesManagement of patients with meningitis and encephalitisSachin DwivediNo ratings yet
- Care of Patient With AnorexiaDocument14 pagesCare of Patient With Anorexiavaishali TMU studentNo ratings yet
- Balanced DietDocument40 pagesBalanced DietAkshatha ShivNo ratings yet
- CURRENT STATUS-WPS OfficeDocument35 pagesCURRENT STATUS-WPS OfficeVinnyNo ratings yet
- Nursing Care PneumoniaDocument26 pagesNursing Care PneumoniaIsaac Kipkemoi100% (1)
- PoliomyelitisDocument43 pagesPoliomyelitisGurpreet KaurNo ratings yet
- Leprosy CHNDocument14 pagesLeprosy CHNPhillip ChingNo ratings yet
- NHP 2Document42 pagesNHP 2A J FathimaNo ratings yet
- Manage Newborn HypothermiaDocument3 pagesManage Newborn HypothermiaYwagar YwagarNo ratings yet
- Childhood Nephrotic Syndrome Diagnosis and ManagementDocument52 pagesChildhood Nephrotic Syndrome Diagnosis and ManagementNilupul Niwantha100% (1)
- A Study To Assess The Effectiveness of Planned Teaching Programme On Knowledge Regarding Eating Disorders Among Adolescent Girls in The Selected Schools of Jabalpur City, MPDocument8 pagesA Study To Assess The Effectiveness of Planned Teaching Programme On Knowledge Regarding Eating Disorders Among Adolescent Girls in The Selected Schools of Jabalpur City, MPEditor IJTSRDNo ratings yet
- Time Table-I - IV Year B.SC 2023Document36 pagesTime Table-I - IV Year B.SC 2023priyagerardNo ratings yet
- Adoption 150109001206 Conversion Gate01Document44 pagesAdoption 150109001206 Conversion Gate01priyagerardNo ratings yet
- 17 Batch AttendanceDocument3 pages17 Batch AttendancepriyagerardNo ratings yet
- Letter Seeking Experts For Content Validity of ToolDocument1 pageLetter Seeking Experts For Content Validity of ToolpriyagerardNo ratings yet
- 4304 - M.Sc. - Community - Health - Nursing ImportantDocument84 pages4304 - M.Sc. - Community - Health - Nursing ImportantpriyagerardNo ratings yet
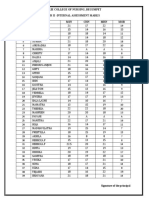
- 17 Batch I.A MarksDocument1 page17 Batch I.A MarkspriyagerardNo ratings yet
- BLINDNESSDocument24 pagesBLINDNESSpriyagerardNo ratings yet
- Abdelfattah Monged Selim - SporotrichosisDocument14 pagesAbdelfattah Monged Selim - SporotrichosispriyagerardNo ratings yet
- International Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikDocument56 pagesInternational Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikpriyagerardNo ratings yet
- 3RD Yr Time Table, 2ND Year and 4TH Year Time Table From 07-2-22 To 12-2-22Document4 pages3RD Yr Time Table, 2ND Year and 4TH Year Time Table From 07-2-22 To 12-2-22priyagerardNo ratings yet
- 0 EndocrinedisordersseminarDocument52 pages0 EndocrinedisordersseminarpriyagerardNo ratings yet
- Nursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)Document35 pagesNursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)priyagerardNo ratings yet
- GNM FIRST YEAR LESSON PLANS FOR COMMUNITY HEALTH NURSINGDocument446 pagesGNM FIRST YEAR LESSON PLANS FOR COMMUNITY HEALTH NURSINGpriyagerardNo ratings yet
- 2020 IA 3rd YearDocument7 pages2020 IA 3rd YearpriyagerardNo ratings yet
- Anatomy and Physiology of the TonsilsDocument11 pagesAnatomy and Physiology of the TonsilspriyagerardNo ratings yet
- 2 2018 12 15!09 27 25 AmDocument24 pages2 2018 12 15!09 27 25 AmNatalia CaramanNo ratings yet
- College Report 2015Document120 pagesCollege Report 2015priyagerardNo ratings yet
- Pituitary GlandDocument34 pagesPituitary GlandpriyagerardNo ratings yet
- Annexure For Dissertations Synopsis SubmissionDocument2 pagesAnnexure For Dissertations Synopsis SubmissionpriyagerardNo ratings yet
- Med Term 2 MTDocument9 pagesMed Term 2 MTpriyagerardNo ratings yet
- S. No. ContentDocument167 pagesS. No. ContentpriyagerardNo ratings yet
- CHN I & Ii Course PlanDocument17 pagesCHN I & Ii Course PlanpriyagerardNo ratings yet
- Body Cavity FluidsDocument29 pagesBody Cavity FluidspriyagerardNo ratings yet
- Unit Iv: Body Fluid AnalysisDocument41 pagesUnit Iv: Body Fluid AnalysispriyagerardNo ratings yet
- Pathology Notes HemalathaDocument117 pagesPathology Notes HemalathapriyagerardNo ratings yet
- Body Fluid Analysis Guide for CSF, Synovial, Pleural FluidsDocument8 pagesBody Fluid Analysis Guide for CSF, Synovial, Pleural FluidspriyagerardNo ratings yet
- UNIT PLAN I CHN IDocument7 pagesUNIT PLAN I CHN IpriyagerardNo ratings yet
- Second Year M.SC Nursing Degree Examinations - September 2016Document1 pageSecond Year M.SC Nursing Degree Examinations - September 2016priyagerardNo ratings yet
- Report On Cancer Run: "Race For Grace"Document2 pagesReport On Cancer Run: "Race For Grace"priyagerardNo ratings yet
- Y10 ICT End of TermDocument7 pagesY10 ICT End of TermIvy Atuhairwe BisoborwaNo ratings yet
- Organic Compounds ExplainedDocument37 pagesOrganic Compounds ExplainedAlejandro VillanuevaNo ratings yet
- The 8 Body ConstitutionsDocument29 pagesThe 8 Body ConstitutionsNiNo ratings yet
- Thesis Based On Digital Image ProcessingDocument7 pagesThesis Based On Digital Image Processingkristenwilsonpeoria100% (1)
- Macalloy Corporate Brochure September 2018 LR PDFDocument12 pagesMacalloy Corporate Brochure September 2018 LR PDFsampathkumarNo ratings yet
- Cucs 016 13 PDFDocument16 pagesCucs 016 13 PDFAnonymous SlyvspdBNo ratings yet
- Innovative Lp1 BlogDocument5 pagesInnovative Lp1 BlogArya ElizabethNo ratings yet
- Nursing Theories: Nightingale, Johnson, Abdellah & MoreDocument8 pagesNursing Theories: Nightingale, Johnson, Abdellah & More3amabelle arevaloNo ratings yet
- 04powertrain 1010Document8 pages04powertrain 1010francis_15inNo ratings yet
- KankanaP Phd2022Document243 pagesKankanaP Phd2022Mo NaNo ratings yet
- Parenteral Fluid Therapy: Types of Intravenous SolutionDocument18 pagesParenteral Fluid Therapy: Types of Intravenous SolutionKathleen Joy Costales Magtanong100% (1)
- Orienteering Lesson PlanDocument34 pagesOrienteering Lesson PlanJuan Carlos Guillen BayonNo ratings yet
- Solar/Wind/Diesel Hybrid Energy System With Battery Storage For Rural ElectrificationDocument15 pagesSolar/Wind/Diesel Hybrid Energy System With Battery Storage For Rural ElectrificationWelde AynaleNo ratings yet
- Tutorial Letter 101/3/2023/B: International OrganisationsDocument15 pagesTutorial Letter 101/3/2023/B: International OrganisationslesegononNo ratings yet
- Table of ContentsDocument2 pagesTable of ContentsPewter VulturelynxNo ratings yet
- A New Approach To The Deposition of Elemental Boron and Boron-Based Coatings by Pulsed Magnetron Sputtering of Loosely Packed Boron Powder TargetsDocument6 pagesA New Approach To The Deposition of Elemental Boron and Boron-Based Coatings by Pulsed Magnetron Sputtering of Loosely Packed Boron Powder TargetsyouamareNo ratings yet
- Toufik Hossain Project On ODE Using Fourier TransformDocument6 pagesToufik Hossain Project On ODE Using Fourier TransformToufik HossainNo ratings yet
- Research Methods in AnthropologyDocument28 pagesResearch Methods in AnthropologyMohammad ALNAJJARNo ratings yet
- Chapter 12 1Document15 pagesChapter 12 1Brigitte ReyesNo ratings yet
- X1jet MX Manual PDFDocument97 pagesX1jet MX Manual PDFrithik srivastavaNo ratings yet
- MC61ADocument5 pagesMC61AAlison Foster100% (1)
- Business Ethics Q3 Mod2 Foundations of The Principles of Business1Document5 pagesBusiness Ethics Q3 Mod2 Foundations of The Principles of Business1Julie CabusaoNo ratings yet
- Sample Final Exam Larkin AnswersDocument18 pagesSample Final Exam Larkin AnswersLovejot SinghNo ratings yet
- Helmut Lethen - Cool Conduct - The Culture of Distance in Weimar Germany (Weimar and Now - German Cultural Criticism) - University of California Press (2001) PDFDocument265 pagesHelmut Lethen - Cool Conduct - The Culture of Distance in Weimar Germany (Weimar and Now - German Cultural Criticism) - University of California Press (2001) PDFJaco CMNo ratings yet
- TCS L6 ActsDocument7 pagesTCS L6 ActsBhebz Erin MaeNo ratings yet
- Demolition and excavation worksDocument30 pagesDemolition and excavation worksHafizan Hanafiah100% (3)
- Physics Universe ModelsDocument14 pagesPhysics Universe ModelsTracy zorca50% (2)
- PreciControl CMV IgG Avidity - Ms - 05942322190.V4.EnDocument2 pagesPreciControl CMV IgG Avidity - Ms - 05942322190.V4.EnARIF AHAMMED PNo ratings yet
- Rhythm MP - The Music Page - Theory Made Easy For Little Children Level 1Document9 pagesRhythm MP - The Music Page - Theory Made Easy For Little Children Level 1AmilacicNo ratings yet
- Farmakoterapi Penyakit Infeksi: in Infectious Diseases Dewi Rahmawati, M.Farm-Klin.,AptDocument87 pagesFarmakoterapi Penyakit Infeksi: in Infectious Diseases Dewi Rahmawati, M.Farm-Klin.,AptYemima MNo ratings yet