You might also like
- Melbourne ACL Rehabilitation Guide 2.0: A criteria driven ACL rehab protocolDocument32 pagesMelbourne ACL Rehabilitation Guide 2.0: A criteria driven ACL rehab protocolgabi balaNo ratings yet
- Evidence-Based Physical Therapy For The Pelvic Floor: Bridging Science and Clinical PracticeDocument438 pagesEvidence-Based Physical Therapy For The Pelvic Floor: Bridging Science and Clinical PracticeNathalie GodartNo ratings yet
- MyITLab Access Grader Real Estate Case SolutionDocument3 pagesMyITLab Access Grader Real Estate Case SolutionShivaani Aggarwal0% (1)
- Profile Shakeel Carpentry Joinery WorksDocument46 pagesProfile Shakeel Carpentry Joinery WorksShakeel Ahmad100% (1)
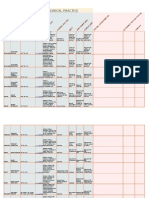
- Goniometry For Clinical PracticeDocument7 pagesGoniometry For Clinical Practicedramitsaini33% (3)
- Efecto de Salud Fisica y Mental Del Covid en FMDocument11 pagesEfecto de Salud Fisica y Mental Del Covid en FMtavo570No ratings yet
- pdf_4401Document9 pagespdf_4401labsoneducationNo ratings yet
- PDF - 4311 FibromyalgiaDocument7 pagesPDF - 4311 Fibromyalgiahekate.yantraNo ratings yet
- BAib12017-02 Guideline On Conceptual Design and Engineering Requirements For CSSU PDFDocument76 pagesBAib12017-02 Guideline On Conceptual Design and Engineering Requirements For CSSU PDFfispl100% (1)
- Rompa International 2023Document220 pagesRompa International 2023AnAs Al ArjanNo ratings yet
- NorthStar Blue Batteries SES-542-55 PDFDocument4 pagesNorthStar Blue Batteries SES-542-55 PDFdamarNo ratings yet
- DENAH GEREJA IMANUEL BAUTASIK-ModelDocument1 pageDENAH GEREJA IMANUEL BAUTASIK-ModelVia YunusNo ratings yet
- White Book Europa MediciphysicaDocument49 pagesWhite Book Europa MediciphysicaІгор СомовNo ratings yet
- JURUTERA Jun22 CompilationDocument48 pagesJURUTERA Jun22 CompilationKit Keong FOONGNo ratings yet
- Rizal Street: Vicinity Map PerspectiveDocument1 pageRizal Street: Vicinity Map PerspectiveLenon RugayanNo ratings yet
- Medicinal MushroomsDocument3 pagesMedicinal MushroomsEllice O. MonizNo ratings yet
- Ground Floor Plan: Waterbody WaterbodyDocument1 pageGround Floor Plan: Waterbody WaterbodyHB ARCHITECTNo ratings yet
- Denah Basement Denah Ac Lantai Basement: Nama Tugas Utilitas BangunanDocument1 pageDenah Basement Denah Ac Lantai Basement: Nama Tugas Utilitas BangunanAlif Dio Riskiansyah100% (1)
- ADAPTOGENS For The New Year PDFDocument1 pageADAPTOGENS For The New Year PDFRaluca ScrieciuNo ratings yet
- ADAPTOGENSDocument1 pageADAPTOGENSIveri Aura100% (1)
- Planta Estructuras y Elevaciones - Sede Social Color PDFDocument1 pagePlanta Estructuras y Elevaciones - Sede Social Color PDFNikolas CaroNo ratings yet
- Btoaug20 AngmokioDocument1 pageBtoaug20 AngmokioShawn LimNo ratings yet
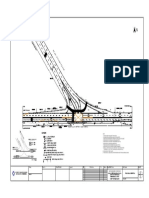
- Sample TMP 1 PDFDocument1 pageSample TMP 1 PDFNizar SeraNo ratings yet
- TBF-300A-310-410 ManualDocument100 pagesTBF-300A-310-410 ManualNuno Costa NumiescoNo ratings yet
- ACCRA Skyport Entry Service Opens UpDocument1 pageACCRA Skyport Entry Service Opens Upvikrant singhNo ratings yet
- Distances Table (In Nautical Miles)Document1 pageDistances Table (In Nautical Miles)muhammad rizalNo ratings yet
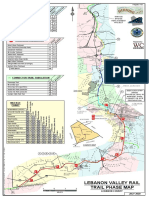
- Lebanon Rail Trail-Map PDFDocument1 pageLebanon Rail Trail-Map PDFj gNo ratings yet
- Outbreak To Recovery: C O V I D - 1 9 2 0 2 0Document2 pagesOutbreak To Recovery: C O V I D - 1 9 2 0 2 0Jeff MorrisNo ratings yet
- Philippine Adult Immunization Recommendation 2017 PDFDocument2 pagesPhilippine Adult Immunization Recommendation 2017 PDFLinius CruzNo ratings yet
- Glasnik SGD 1976Document310 pagesGlasnik SGD 1976Eremac24No ratings yet
- BP Fragrance Journal PagesDocument1 pageBP Fragrance Journal PagesConstance FenskeNo ratings yet
- Generic Medicinre: Generic Medicine Generic Medicine Generic Medicine Generic MedicineDocument5 pagesGeneric Medicinre: Generic Medicine Generic Medicine Generic Medicine Generic MedicineganeshNo ratings yet
- Incremento salarial del 2% en enero de 2021Document9 pagesIncremento salarial del 2% en enero de 2021Gersy paul Rodriguez AraujoNo ratings yet
- Catalogue ProductsDocument344 pagesCatalogue Productsshahar swissaNo ratings yet
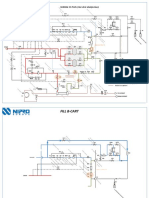
- Dialysate and blood circuit for patient toxin removalDocument4 pagesDialysate and blood circuit for patient toxin removalHyacinthe KOSSINo ratings yet
- West Briar: Buffa Lo Ba YouDocument1 pageWest Briar: Buffa Lo Ba Youdiego masinoNo ratings yet
- Town of Philipstown Land Use and Development Overlay District Zoning MapDocument1 pageTown of Philipstown Land Use and Development Overlay District Zoning MapPCNRNo ratings yet
- Onshore Receiving Facility Isometric Piping DrawingDocument4 pagesOnshore Receiving Facility Isometric Piping DrawingGayuhNo ratings yet
- Proyecto Damas-PLANTADocument1 pageProyecto Damas-PLANTACristhian IvanNo ratings yet
- PPE Assessment MatrixDocument1 pagePPE Assessment MatrixthennarasuNo ratings yet
- Paz Soldán - Cartas Históricas Del Perú V. IDocument444 pagesPaz Soldán - Cartas Históricas Del Perú V. IDaniel Rodriguez SanchezNo ratings yet
- DHARIAWADDocument1 pageDHARIAWADAGM Operation UdaipurNo ratings yet
- Park at Numaish GroundDocument1 pagePark at Numaish GroundAnshul SharmaNo ratings yet
- BP Fragrance Families TableDocument1 pageBP Fragrance Families TableConstance FenskeNo ratings yet
- LG 42LC4RDocument88 pagesLG 42LC4RbimusicaNo ratings yet
- General Notes:: WC DP SHDocument9 pagesGeneral Notes:: WC DP SHDT DESIGN STUDIONo ratings yet
- pf84 EngDocument1 pagepf84 EngDiego Vinicius LopesNo ratings yet
- Santa Monica A1Document1 pageSanta Monica A1gambetzNo ratings yet
- Btoaug20 BishanDocument1 pageBtoaug20 BishanShawn LimNo ratings yet
- Achievement Chart MacasDocument4 pagesAchievement Chart MacasJenn MacasNo ratings yet
- Progress Chart MacasDocument4 pagesProgress Chart MacasJenn MacasNo ratings yet
- Quick Install Guide Compact Multiplus 12v 24v 800va 1200va 1600va 230vac enDocument1 pageQuick Install Guide Compact Multiplus 12v 24v 800va 1200va 1600va 230vac enivan bkoNo ratings yet
- Adult Immunization Recommendation 2017: Philippine Foundation For Vaccina IonDocument2 pagesAdult Immunization Recommendation 2017: Philippine Foundation For Vaccina Iontheresa chingNo ratings yet
- REKAP KELAS XII GanjilDocument10 pagesREKAP KELAS XII GanjilNurul HudaNo ratings yet
- Floor PlanDocument1 pageFloor PlanJohn Michael PilongoNo ratings yet
- Website security future updatesDocument7 pagesWebsite security future updatesJessa Mae CatabayNo ratings yet
- Structures Project: Typical Floor Beam LayoutDocument1 pageStructures Project: Typical Floor Beam LayoutAlekhya DeviNo ratings yet
- Readiness Assessment Tools - CAVITE PROVINCE 2023 MR SIA - (PHO CHO MHO RHU HC BHSDocument186 pagesReadiness Assessment Tools - CAVITE PROVINCE 2023 MR SIA - (PHO CHO MHO RHU HC BHSChristean Val Bayani ValezaNo ratings yet
- 5182775-DRS-ELEC-SD-00086-Rev.1-2F PLAN LV CONTAINMENT LAYOUT (SHEET 2)Document1 page5182775-DRS-ELEC-SD-00086-Rev.1-2F PLAN LV CONTAINMENT LAYOUT (SHEET 2)Maged BeshayNo ratings yet
- Master Plan.Document1 pageMaster Plan.Hikmat AyerNo ratings yet
- Master Plan of Bhaktapur ResortDocument1 pageMaster Plan of Bhaktapur ResortHikmat AyerNo ratings yet
- Theory of Knowledge - Key Concepts - Marija Uzunova Dang and Arvin Singh Uzunov Dang - Oxford 2020Document15 pagesTheory of Knowledge - Key Concepts - Marija Uzunova Dang and Arvin Singh Uzunov Dang - Oxford 2020Rex Wong50% (2)
- The Rough Guide to Beijing (Travel Guide eBook)From EverandThe Rough Guide to Beijing (Travel Guide eBook)Rating: 2 out of 5 stars2/5 (1)
- Skeletal Muscle Hypertrophy After Aerobic Exercise TrainingDocument9 pagesSkeletal Muscle Hypertrophy After Aerobic Exercise TrainingDouglas MarinNo ratings yet
- El Estrés, El Sueño No Reparador y La Inactividad Física Como Factores de Riesgo de Dolor Crónico en Adultos JóvenesDocument17 pagesEl Estrés, El Sueño No Reparador y La Inactividad Física Como Factores de Riesgo de Dolor Crónico en Adultos JóvenesDANIELANo ratings yet
- MainDocument15 pagesMainJesusNavarrete97No ratings yet
- ShijagurumayumAcharya2020 Article PelvicFloorMuscleTrainingProgrDocument11 pagesShijagurumayumAcharya2020 Article PelvicFloorMuscleTrainingProgrJesusNavarrete97No ratings yet
- Exercise Physiology in Cirrhosis and The Potential Benefits of Exercise Interventions A ReviewDocument19 pagesExercise Physiology in Cirrhosis and The Potential Benefits of Exercise Interventions A ReviewJesusNavarrete97No ratings yet
- Physical Exercise Is A Potential "Medicine" For AtherosclerosisDocument18 pagesPhysical Exercise Is A Potential "Medicine" For AtherosclerosisJesusNavarrete97No ratings yet
- The 5 Min Meta-Analysis. Understanding How To Read and Interpret A Forest PlotDocument3 pagesThe 5 Min Meta-Analysis. Understanding How To Read and Interpret A Forest PlotJesusNavarrete97No ratings yet
- Evidence For Prescribing PA As Therapy in 26 Different Chronic Diseases PDFDocument72 pagesEvidence For Prescribing PA As Therapy in 26 Different Chronic Diseases PDFKike TostadoNo ratings yet
- 2017 The Cardiovascular System After Exercise PDFDocument8 pages2017 The Cardiovascular System After Exercise PDFTote Cifuentes AmigoNo ratings yet
- A Century of Exercise Physiology Key Concepts in Muscle Cell Volume RegulationDocument19 pagesA Century of Exercise Physiology Key Concepts in Muscle Cell Volume RegulationJesusNavarrete97No ratings yet
- The Effect of Nordic Hamstring Exercise InterventiDocument17 pagesThe Effect of Nordic Hamstring Exercise InterventiMostafa EsmaelieNo ratings yet
- How to actively read scientific papersDocument6 pagesHow to actively read scientific paperscastillojessNo ratings yet
- Effects of Exercise On Cellular and Tissue AgingDocument22 pagesEffects of Exercise On Cellular and Tissue AgingJesusNavarrete97No ratings yet
- Effects of Physical Therapy On Mental Function in Patients With StrokeDocument6 pagesEffects of Physical Therapy On Mental Function in Patients With StrokeTeuku FadhliNo ratings yet
- The Role of Resistance Exercise Training For Improving Cardiorespiratory Fitness in Healthy Older Adults. A Systematic Review and Meta-AnalysisDocument9 pagesThe Role of Resistance Exercise Training For Improving Cardiorespiratory Fitness in Healthy Older Adults. A Systematic Review and Meta-AnalysisJesusNavarrete97No ratings yet
- High Ankle SprainDocument6 pagesHigh Ankle SprainJesusNavarrete97No ratings yet
- Physiotherapy Blood Investigations JPDocument51 pagesPhysiotherapy Blood Investigations JPJesusNavarrete97No ratings yet
- Flyer Ankle Sprain Rehabilitation PT GuidelineDocument3 pagesFlyer Ankle Sprain Rehabilitation PT GuidelineEka Wahyu HerdiyantiNo ratings yet
- UntitledDocument1 pageUntitledMoizur RahmanNo ratings yet
- Monopolistic screening in the labor marketDocument6 pagesMonopolistic screening in the labor marketKand HroppaNo ratings yet
- Generac Generac CAT MTU Cummins KohlerDocument3 pagesGenerac Generac CAT MTU Cummins KohlerJuly E. Maldonado M.No ratings yet
- 8.4.3 Alien Genetics LabDocument2 pages8.4.3 Alien Genetics LabCharles KnightNo ratings yet
- Micro-operations and the CPU ClockDocument28 pagesMicro-operations and the CPU ClockchandraNo ratings yet
- CorrectDocument45 pagesCorrectaskerman 3No ratings yet
- Airfoil DesignDocument18 pagesAirfoil Designapi-269373691No ratings yet
- Revit Quiz 1 ReviewerDocument13 pagesRevit Quiz 1 ReviewerLanz RamosNo ratings yet
- 2022 AMC Paper MP OMRDocument12 pages2022 AMC Paper MP OMRshilpa_aryan100% (1)
- Ryan Ashby DickinsonDocument2 pagesRyan Ashby Dickinsonapi-347999772No ratings yet
- Chapter Arithmetic and Geometric Progressions 024005Document14 pagesChapter Arithmetic and Geometric Progressions 024005ravichandran_brNo ratings yet
- Design Approval Checklist 2nd Rev.Document3 pagesDesign Approval Checklist 2nd Rev.Daric Tesfaye0% (1)
- The Future of Luxury Fashion ReportDocument70 pagesThe Future of Luxury Fashion Reportsalma andjaniNo ratings yet
- Sem NotesDocument39 pagesSem NotesN NandiniNo ratings yet
- UKPSC JE Civil 2024 Exam (Technical) - ScheduleDocument4 pagesUKPSC JE Civil 2024 Exam (Technical) - ScheduleIES-GATEWizNo ratings yet
- Sump Pumps: Single Channel Soft Solids Handling Sewage PumpDocument2 pagesSump Pumps: Single Channel Soft Solids Handling Sewage PumpMohammad ZeeshanNo ratings yet
- (Manual) Design Standards For Stormwater Detention and Retention - 14-05 VersionDocument113 pages(Manual) Design Standards For Stormwater Detention and Retention - 14-05 VersionMarcos JulianoNo ratings yet
- Design of Base Slab of UGTDocument5 pagesDesign of Base Slab of UGTAamir SuhailNo ratings yet
- David Kassan DemoDocument3 pagesDavid Kassan DemokingkincoolNo ratings yet
- Did You Ever Meet Shattered Illusions?Document5 pagesDid You Ever Meet Shattered Illusions?Junjie HuangNo ratings yet
- Anis MahmudahDocument14 pagesAnis MahmudahAlim ZainulNo ratings yet
- Plastiment BV40Document2 pagesPlastiment BV40the pilotNo ratings yet
- Consumer Behavior Quiz (01-16-21)Document3 pagesConsumer Behavior Quiz (01-16-21)litNo ratings yet
- Fibre OpticDocument16 pagesFibre OpticJoanna BaileyNo ratings yet
- SFRM Commissioning and Field Testing - Structural Fire Resistance Content From Fire Protection EngineeringDocument6 pagesSFRM Commissioning and Field Testing - Structural Fire Resistance Content From Fire Protection EngineeringRichard HollidayNo ratings yet
- OSHCo Study I MalaysiaDocument7 pagesOSHCo Study I MalaysiafairusNo ratings yet
- Risktec Drilling Soc 0.3 PDFDocument16 pagesRisktec Drilling Soc 0.3 PDF1sNo ratings yet
- Paper ESEE2017 CLJLand MLDocument12 pagesPaper ESEE2017 CLJLand MLMatheus CardimNo ratings yet