You might also like
- PDF - 4311 FibromyalgiaDocument7 pagesPDF - 4311 Fibromyalgiahekate.yantraNo ratings yet
- Efecto de Salud Fisica y Mental Del Covid en FMDocument11 pagesEfecto de Salud Fisica y Mental Del Covid en FMtavo570No ratings yet
- Preoperative Pain Neurophysiology Education For Lumbar Radiculopathy. A Randomized-Controlled TrialDocument8 pagesPreoperative Pain Neurophysiology Education For Lumbar Radiculopathy. A Randomized-Controlled TrialJesusNavarrete97No ratings yet
- White Book Europa MediciphysicaDocument49 pagesWhite Book Europa MediciphysicaІгор СомовNo ratings yet
- Procedimientos y Cirugía en ORL ZurdosDocument1 pageProcedimientos y Cirugía en ORL ZurdosMarco Antonio FigueroaNo ratings yet
- BAib12017-02 Guideline On Conceptual Design and Engineering Requirements For CSSU PDFDocument76 pagesBAib12017-02 Guideline On Conceptual Design and Engineering Requirements For CSSU PDFfispl100% (1)
- JURUTERA Jun22 CompilationDocument48 pagesJURUTERA Jun22 CompilationKit Keong FOONGNo ratings yet
- Generic Medicinre: Generic Medicine Generic Medicine Generic Medicine Generic MedicineDocument5 pagesGeneric Medicinre: Generic Medicine Generic Medicine Generic Medicine Generic MedicineganeshNo ratings yet
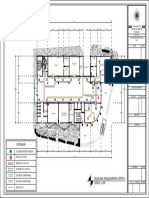
- Denah Basement Denah Ac Lantai Basement: Nama Tugas Utilitas BangunanDocument1 pageDenah Basement Denah Ac Lantai Basement: Nama Tugas Utilitas BangunanAlif Dio Riskiansyah100% (1)
- Rompa International 2023Document220 pagesRompa International 2023AnAs Al ArjanNo ratings yet
- Medicinal MushroomsDocument3 pagesMedicinal MushroomsEllice O. MonizNo ratings yet
- Outbreak To Recovery: C O V I D - 1 9 2 0 2 0Document2 pagesOutbreak To Recovery: C O V I D - 1 9 2 0 2 0Jeff MorrisNo ratings yet
- Theory of Knowledge - Key Concepts - Marija Uzunova Dang and Arvin Singh Uzunov Dang - Oxford 2020Document15 pagesTheory of Knowledge - Key Concepts - Marija Uzunova Dang and Arvin Singh Uzunov Dang - Oxford 2020Rex Wong50% (2)
- DENAH GEREJA IMANUEL BAUTASIK-ModelDocument1 pageDENAH GEREJA IMANUEL BAUTASIK-ModelVia YunusNo ratings yet
- ROADMAP 2050: Technical Analysis Executive SummaryDocument24 pagesROADMAP 2050: Technical Analysis Executive Summarybfly754151No ratings yet
- Planta Estructuras y Elevaciones - Sede Social Color PDFDocument1 pagePlanta Estructuras y Elevaciones - Sede Social Color PDFNikolas CaroNo ratings yet
- Wms GINA 2018 Strategy Report V1.1 PDFDocument161 pagesWms GINA 2018 Strategy Report V1.1 PDFEdson ArmandoNo ratings yet
- Progress Chart MacasDocument4 pagesProgress Chart MacasJenn MacasNo ratings yet
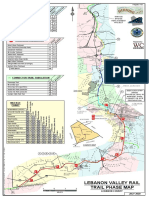
- Lebanon Rail Trail-Map PDFDocument1 pageLebanon Rail Trail-Map PDFj gNo ratings yet
- Achievement Chart MacasDocument4 pagesAchievement Chart MacasJenn MacasNo ratings yet
- NorthStar Blue Batteries SES-542-55 PDFDocument4 pagesNorthStar Blue Batteries SES-542-55 PDFdamarNo ratings yet
- ACCRA Skyport Entry Service Opens UpDocument1 pageACCRA Skyport Entry Service Opens Upvikrant singhNo ratings yet
- Renc - Cilling 1Document1 pageRenc - Cilling 1trio alfajarNo ratings yet
- Btoaug20 AngmokioDocument1 pageBtoaug20 AngmokioShawn LimNo ratings yet
- Math 162Document5 pagesMath 162Surafel L. TilahunNo ratings yet
- Upgrading Highway Project Plan and Profile SheetsDocument1 pageUpgrading Highway Project Plan and Profile Sheets4jhe Di4sNo ratings yet
- The Reward and Remuneration Series Handbook PDFDocument320 pagesThe Reward and Remuneration Series Handbook PDFOdhis KanayoNo ratings yet
- JEmergTraumaShock - 2013 KhoeDocument3 pagesJEmergTraumaShock - 2013 Khoenurulanisa0703No ratings yet
- Air Purifier THDocument1 pageAir Purifier THviktorija bezhovskaNo ratings yet
- TBF-300A-310-410 ManualDocument100 pagesTBF-300A-310-410 ManualNuno Costa NumiescoNo ratings yet
- Paz Soldán - Cartas Históricas Del Perú V. IDocument444 pagesPaz Soldán - Cartas Históricas Del Perú V. IDaniel Rodriguez SanchezNo ratings yet
- 2017 GINA Report, Global Strategy For Asthma Management and Prevention PDFDocument159 pages2017 GINA Report, Global Strategy For Asthma Management and Prevention PDFNalemi JT100% (1)
- LG 42LC4RDocument88 pagesLG 42LC4RbimusicaNo ratings yet
- ADAPTOGENS For The New Year PDFDocument1 pageADAPTOGENS For The New Year PDFRaluca ScrieciuNo ratings yet
- Website security future updatesDocument7 pagesWebsite security future updatesJessa Mae CatabayNo ratings yet
- ADAPTOGENSDocument1 pageADAPTOGENSIveri Aura100% (1)
- PERIMETRICO 2-ModeloDocument1 pagePERIMETRICO 2-ModeloGustavo OrtegaNo ratings yet
- Malaysian Education System Reform EducatDocument5 pagesMalaysian Education System Reform EducatFunninhaNo ratings yet
- UNRSF Who We Are Jan21Document2 pagesUNRSF Who We Are Jan21Carlos Guillermo Carrillo BolañosNo ratings yet
- BP Fragrance Journal PagesDocument1 pageBP Fragrance Journal PagesConstance FenskeNo ratings yet
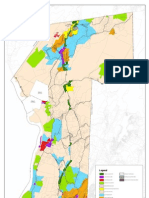
- Town of Philipstown Land Use and Development Overlay District Zoning MapDocument1 pageTown of Philipstown Land Use and Development Overlay District Zoning MapPCNRNo ratings yet
- Floor PlanDocument1 pageFloor PlanJohn Michael PilongoNo ratings yet
- Glasnik SGD 1976Document310 pagesGlasnik SGD 1976Eremac24No ratings yet
- Psychological First AidDocument1 pagePsychological First AidXBXNo ratings yet
- Distances Table (In Nautical Miles)Document1 pageDistances Table (In Nautical Miles)muhammad rizalNo ratings yet
- Sample TMP 1 PDFDocument1 pageSample TMP 1 PDFNizar SeraNo ratings yet
- Rizal Street: Vicinity Map PerspectiveDocument1 pageRizal Street: Vicinity Map PerspectiveLenon RugayanNo ratings yet
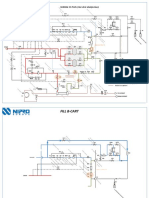
- Dialysate and blood circuit for patient toxin removalDocument4 pagesDialysate and blood circuit for patient toxin removalHyacinthe KOSSINo ratings yet
- BP Fragrance Families TableDocument1 pageBP Fragrance Families TableConstance FenskeNo ratings yet
- Ignatius Ivan Putrantyo: Course CertificateDocument1 pageIgnatius Ivan Putrantyo: Course CertificateXBXNo ratings yet
- Coursera 8T46PEUTWKS6 PDFDocument1 pageCoursera 8T46PEUTWKS6 PDFMarjan HabibNo ratings yet
- Abstractbook 14th INTEREST 2020Document523 pagesAbstractbook 14th INTEREST 2020Pelumi AshamuNo ratings yet
- 04 10 2019 Lamifil Ohc Brochure LR PDFDocument11 pages04 10 2019 Lamifil Ohc Brochure LR PDFgheorghe_marian_7No ratings yet
- Saudi Electricity Company Eastern Region Branch Indoor and Outdoor Lighting System DesignDocument9 pagesSaudi Electricity Company Eastern Region Branch Indoor and Outdoor Lighting System DesignSomnath DasNo ratings yet
- Keterangan: Ac Ceiling Mounted Cassete Fan Coil Unit (Fcu)Document1 pageKeterangan: Ac Ceiling Mounted Cassete Fan Coil Unit (Fcu)zani marcelianaNo ratings yet
- The Rough Guide to Beijing (Travel Guide eBook)From EverandThe Rough Guide to Beijing (Travel Guide eBook)Rating: 2 out of 5 stars2/5 (1)
- A Comparative Study of Positive Versus Negative Polarity in the tDocument55 pagesA Comparative Study of Positive Versus Negative Polarity in the tlabsoneducationNo ratings yet
- fes_electrode_placement_upper_body-2018Document5 pagesfes_electrode_placement_upper_body-2018labsoneducationNo ratings yet
- 19 Electrical Stimulation for the Upper Extremity 2016 04 HandoutDocument22 pages19 Electrical Stimulation for the Upper Extremity 2016 04 HandoutlabsoneducationNo ratings yet
- tDCS in pediatric hemiparesisDocument1 pagetDCS in pediatric hemiparesislabsoneducationNo ratings yet
- Valery Labou Professional CV Resume Apr 2024 CFEDocument2 pagesValery Labou Professional CV Resume Apr 2024 CFElabsoneducationNo ratings yet
- safety limits fortDCSDocument2 pagessafety limits fortDCSlabsoneducationNo ratings yet
- ROBOTIC REHABILITATION OF STROKE PATIENTSDocument11 pagesROBOTIC REHABILITATION OF STROKE PATIENTSlabsoneducationNo ratings yet
- EMG MuscleStrength LS2 ELVISDocument15 pagesEMG MuscleStrength LS2 ELVISlabsoneducationNo ratings yet
- Repetitive transcranial magnetic stimulation and tDCS in motor rehab after strokeDocument5 pagesRepetitive transcranial magnetic stimulation and tDCS in motor rehab after strokelabsoneducationNo ratings yet
- PDF 20230322 205237 0000 PDFDocument1 pagePDF 20230322 205237 0000 PDFDynamicmusic AnbuNo ratings yet
- safetyaspect in tDCS in patient and healthy subjectsDocument7 pagessafetyaspect in tDCS in patient and healthy subjectslabsoneducationNo ratings yet
- Face-to-face physiotherapy compared with a supported home exercise programme for the management of musculoskeletal conditions- protocol of a multicentre, randomised controlled trial—the REFORM trialDocument8 pagesFace-to-face physiotherapy compared with a supported home exercise programme for the management of musculoskeletal conditions- protocol of a multicentre, randomised controlled trial—the REFORM triallabsoneducationNo ratings yet
- Protocol Form ExamplesDocument6 pagesProtocol Form ExamplesSimina Florina BaltaNo ratings yet
- Blue Simple Professional CV Resume (2)Document2 pagesBlue Simple Professional CV Resume (2)labsoneducationNo ratings yet
- Section1Document35 pagesSection1labsoneducationNo ratings yet
- 1-s2.0-S2589004219301051-mainDocument49 pages1-s2.0-S2589004219301051-mainlabsoneducationNo ratings yet
- 1-s2.0-S1053811919304240-mainDocument10 pages1-s2.0-S1053811919304240-mainlabsoneducationNo ratings yet
- Spasticity After SCI PDFDocument10 pagesSpasticity After SCI PDFNovaria PuspitaNo ratings yet
- electrical stim dont read nowDocument11 pageselectrical stim dont read nowlabsoneducationNo ratings yet
- 1-s2.0-S1882761609000921-mainDocument11 pages1-s2.0-S1882761609000921-mainlabsoneducationNo ratings yet
- fnint-11-00002Document15 pagesfnint-11-00002labsoneducationNo ratings yet
- 08d91117-59ca-411f-b22b-0e2449878444Document7 pages08d91117-59ca-411f-b22b-0e2449878444labsoneducationNo ratings yet
- 2011_NeuroanatomicalaspectsofthebodyawarenessDocument5 pages2011_NeuroanatomicalaspectsofthebodyawarenesslabsoneducationNo ratings yet
- 1-s2.0-S1053811919304240-mainDocument10 pages1-s2.0-S1053811919304240-mainlabsoneducationNo ratings yet
- Seven Point Checklist and WelcomeDocument3 pagesSeven Point Checklist and WelcomelabsoneducationNo ratings yet
- Muscle Shortening Manoeuver in CPDocument6 pagesMuscle Shortening Manoeuver in CPlabsoneducationNo ratings yet
- 2020-0108-grant-writing presentationDocument71 pages2020-0108-grant-writing presentationlabsoneducationNo ratings yet
- neuromodulationstrokerecoverysig2023annualreportDocument5 pagesneuromodulationstrokerecoverysig2023annualreportlabsoneducationNo ratings yet
- 13-diagnosismanagementoftemporomandibulardisorderselly-180501180556Document108 pages13-diagnosismanagementoftemporomandibulardisorderselly-180501180556labsoneducationNo ratings yet
- AFP Ready Ref Develop Fund Policies 0119_1Document64 pagesAFP Ready Ref Develop Fund Policies 0119_1labsoneducationNo ratings yet
- UKPSC JE Civil 2024 Exam (Technical) - ScheduleDocument4 pagesUKPSC JE Civil 2024 Exam (Technical) - ScheduleIES-GATEWizNo ratings yet
- Defibrelator ch1Document31 pagesDefibrelator ch1د.محمد عبد المنعم الشحاتNo ratings yet
- Surveyquestionnaire 1Document6 pagesSurveyquestionnaire 1Almira IbarraNo ratings yet
- Introduction to Oil & Gas Drilling and Well OperationsDocument22 pagesIntroduction to Oil & Gas Drilling and Well OperationsMohammed Abdul SamiNo ratings yet
- Z22 Double-Suction Axially-Split Single-Stage Centrifugal PumpDocument2 pagesZ22 Double-Suction Axially-Split Single-Stage Centrifugal Pumpmartín_suárez_110% (1)
- Study of NanofibresDocument237 pagesStudy of NanofibresGerardo ZambranoNo ratings yet
- Katalog Ag-700 To Ag-800Document1 pageKatalog Ag-700 To Ag-800Iqbal AbugindaNo ratings yet
- Comparative ratings of heavy duty cablesDocument1 pageComparative ratings of heavy duty cablesshivani76% (25)
- Module 14 - Final FilesDocument1,042 pagesModule 14 - Final FilesMinami KotoriNo ratings yet
- MSC - Nastran 2014 Linear Static Analysis User's Guide PDFDocument762 pagesMSC - Nastran 2014 Linear Static Analysis User's Guide PDFFeiNo ratings yet
- Cars and Trucks With Mitsubishi TD04 TurbochargerDocument17 pagesCars and Trucks With Mitsubishi TD04 TurbochargersampapaNo ratings yet
- 909design of High Efficiency Pelton Turbine For Micro-HydropowerDocument13 pages909design of High Efficiency Pelton Turbine For Micro-HydropowerrachidtuNo ratings yet
- Customer Satisfaction Romania URTPDocument16 pagesCustomer Satisfaction Romania URTPGajanan PatilNo ratings yet
- Practical Research 2: Quarter 1 - Module 1Document35 pagesPractical Research 2: Quarter 1 - Module 1Alvin Sinel Belejerdo90% (10)
- Smart CityDocument4 pagesSmart CityRendi NafiahNo ratings yet
- Einas Mansour - Curriculum VitaeDocument3 pagesEinas Mansour - Curriculum VitaeEinas MansourNo ratings yet
- Warehouse Processes/OperationsDocument4 pagesWarehouse Processes/OperationsNhsyyNo ratings yet
- 8.4.3 Alien Genetics LabDocument2 pages8.4.3 Alien Genetics LabCharles KnightNo ratings yet
- Uncertainty in Measurements - Lab ReportDocument4 pagesUncertainty in Measurements - Lab ReportStaniaNo ratings yet
- Design of Base Slab of UGTDocument5 pagesDesign of Base Slab of UGTAamir SuhailNo ratings yet
- Lecture Notes (Chapter 2.3 Triple Integral)Document5 pagesLecture Notes (Chapter 2.3 Triple Integral)shinee_jayasila2080100% (1)
- ICs Interface and Motor DriversDocument4 pagesICs Interface and Motor DriversJohn Joshua MontañezNo ratings yet
- Articol S.brînza, V.stati Pag.96Document154 pagesArticol S.brînza, V.stati Pag.96crina1996No ratings yet
- Cultural Dimensions & EthnocentrismDocument38 pagesCultural Dimensions & EthnocentrismKatya Alexis SalitaNo ratings yet
- AlumaCore OPGWDocument1 pageAlumaCore OPGWlepouletNo ratings yet
- Acer Aspire 1710 (Quanta DT3) PDFDocument35 pagesAcer Aspire 1710 (Quanta DT3) PDFMustafa AkanNo ratings yet
- Pytania Do Obrony Spoza Pracy Dyplomowej Filologia Angielska Studia I StopniaDocument5 pagesPytania Do Obrony Spoza Pracy Dyplomowej Filologia Angielska Studia I StopniabartNo ratings yet
- 3G FactsDocument17 pages3G Factsainemoses5798No ratings yet
- LCD LG (M17,1917S-BNN E)Document34 pagesLCD LG (M17,1917S-BNN E)Ion IonutNo ratings yet
- Kaparewetec Farnctbk GbematasDocument37 pagesKaparewetec Farnctbk Gbematasriani antartikaNo ratings yet