You might also like
- Euroscience: Molecular, Cellular and Circuit Basis of Cholinergic Modulation of PainDocument14 pagesEuroscience: Molecular, Cellular and Circuit Basis of Cholinergic Modulation of PainPriyabrata HalderNo ratings yet
- Phantom Limb Pain: Subtle Energy PerspectivesDocument28 pagesPhantom Limb Pain: Subtle Energy PerspectivesMircea PocolNo ratings yet
- Pain Perception and Hypnosis Findings From Recent Functional Neuroimaging StudiesDocument28 pagesPain Perception and Hypnosis Findings From Recent Functional Neuroimaging StudiesAlberto AlbertiNo ratings yet
- Hypnosis & Neuroimaging 2009Document15 pagesHypnosis & Neuroimaging 2009malwinatmdNo ratings yet
- Pathophysiologyofpain 0899 p349-357Document12 pagesPathophysiologyofpain 0899 p349-357Barbara Sakura RiawanNo ratings yet
- Dealing With Phantom Limb Pain After AmputationDocument3 pagesDealing With Phantom Limb Pain After AmputationConnie SianiparNo ratings yet
- Pain Neuroscience EducationDocument26 pagesPain Neuroscience EducationGustavo Cabanas100% (1)
- Neurophysiology of the Migraine BrainFrom EverandNeurophysiology of the Migraine BrainGianluca CoppolaNo ratings yet
- Pain and fMRI2Document29 pagesPain and fMRI2Saad MotawéaNo ratings yet
- Link Between Emotional and PhysicalDocument5 pagesLink Between Emotional and PhysicalsumeetkantkaulNo ratings yet
- Managing Neuropathic PainDocument10 pagesManaging Neuropathic PainAgusBhakti100% (1)
- Pathophysiology of ParesthesiaDocument17 pagesPathophysiology of Paresthesiahardian0% (1)
- EFNS Guideline 2004 Neuropathic Pain AssessmentDocument10 pagesEFNS Guideline 2004 Neuropathic Pain AssessmentDeni Andre AtmadinataNo ratings yet
- Cambios Neuroplasticos en El Dolor Musculo Esqueletico Crónico Un Revision 2012Document18 pagesCambios Neuroplasticos en El Dolor Musculo Esqueletico Crónico Un Revision 2012Daniela Leyton PezoaNo ratings yet
- Hypnosis 0001 PDFDocument11 pagesHypnosis 0001 PDFalanNo ratings yet
- HipnosisDocument11 pagesHipnosisvalentina mierNo ratings yet
- Intralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?From EverandIntralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?No ratings yet
- Psychopathy and The Mirror Neuron System: Preliminary Findings From A Non-Psychiatric SampleDocument8 pagesPsychopathy and The Mirror Neuron System: Preliminary Findings From A Non-Psychiatric SampleAnca Gabriela CristeaNo ratings yet
- There Are Two Types of Nociceptors Corresponding ToDocument6 pagesThere Are Two Types of Nociceptors Corresponding ToPhilipus Putra RaharjoNo ratings yet
- Physiology of PainDocument30 pagesPhysiology of PainVaibhavJain100% (1)
- TENS2Document13 pagesTENS2Georgiana BunghiuzNo ratings yet
- PT's Guide to Understanding PainDocument39 pagesPT's Guide to Understanding PainJoaquin Ulloa100% (1)
- Topical Meds for Neuropathic Orofacial PainDocument13 pagesTopical Meds for Neuropathic Orofacial PainMarco Antonio Morales OsorioNo ratings yet
- The Effect of Spinal Manipulative Therapy OnDocument22 pagesThe Effect of Spinal Manipulative Therapy OncpfisioNo ratings yet
- Physiology of Pain - General Mechanisms and Individual DifferencesDocument3 pagesPhysiology of Pain - General Mechanisms and Individual DifferencesFaris MisbahulNo ratings yet
- FSP DolorDocument15 pagesFSP DoloranyNo ratings yet
- Descending Pain Modulation and Chronification of Pain: ReviewDocument9 pagesDescending Pain Modulation and Chronification of Pain: ReviewJose PerezNo ratings yet
- Integrando Terapia Manual e Neurociencia Da DorDocument274 pagesIntegrando Terapia Manual e Neurociencia Da DorÁtila HanemannNo ratings yet
- Implications On Hypnotherapy - Neuroplasticity, Epigenetics and PainDocument10 pagesImplications On Hypnotherapy - Neuroplasticity, Epigenetics and PainOlivier BenarrocheNo ratings yet
- Orofacial Musculoskeletal Pain. An Evidence-Based Bio-Psycho-Social Matrix ModelDocument27 pagesOrofacial Musculoskeletal Pain. An Evidence-Based Bio-Psycho-Social Matrix ModelAMBAR JOSEFA ALEJANDRA MORAGA VALENZUELANo ratings yet
- Basics of Pain ControlDocument22 pagesBasics of Pain ControlJailan IbrahimNo ratings yet
- a3affca78a327fcb928451d73effb001Document10 pagesa3affca78a327fcb928451d73effb001gipecNo ratings yet
- Toward A Unified Theory of NarcosisDocument17 pagesToward A Unified Theory of NarcosisLia JimenezNo ratings yet
- Pain Syndromes in Neurology: Butterworths International Medical ReviewsFrom EverandPain Syndromes in Neurology: Butterworths International Medical ReviewsHoward L. FieldsRating: 5 out of 5 stars5/5 (1)
- Dolor Radicular y Pseudo Dolor Radicular Freynhagen 2008Document10 pagesDolor Radicular y Pseudo Dolor Radicular Freynhagen 2008Victor Andrés Olivares IbarraNo ratings yet
- Tracey (2007) - The Cerebral Signature For Pain Perception and Its ModulationDocument15 pagesTracey (2007) - The Cerebral Signature For Pain Perception and Its ModulationLuciana AraújoNo ratings yet
- J JMPT 2012 09 003Document6 pagesJ JMPT 2012 09 003Tahira RajputNo ratings yet
- Fdocuments - in - The Puzzle of Pain Loss of Mobility Evasive Movements The Puzzle of PainDocument21 pagesFdocuments - in - The Puzzle of Pain Loss of Mobility Evasive Movements The Puzzle of PainMARIA TERAPEUTANo ratings yet
- AliliDocument3 pagesAliliSaf Tanggo DiampuanNo ratings yet
- Assessment of Chronic PainDocument7 pagesAssessment of Chronic PainFranciscoGarciaNo ratings yet
- Low Back Related Leg Pain Is The Nerve Guilty How To Differentiate The Underlying Pain MechanismDocument8 pagesLow Back Related Leg Pain Is The Nerve Guilty How To Differentiate The Underlying Pain Mechanism杨钦杰No ratings yet
- In The Spine or in The Brain? Recent Advances in Pain Neuroscience Applied in The Intervention For Low Back PainDocument8 pagesIn The Spine or in The Brain? Recent Advances in Pain Neuroscience Applied in The Intervention For Low Back PainVizaNo ratings yet
- Human Brain Mechanisms of Pain PerceptionDocument22 pagesHuman Brain Mechanisms of Pain Perceptionnynaeve_almeeraNo ratings yet
- Neuroscience of Pain, Stress, and Emotion: Psychological and Clinical ImplicationsFrom EverandNeuroscience of Pain, Stress, and Emotion: Psychological and Clinical ImplicationsMagne Arve FlatenRating: 4.5 out of 5 stars4.5/5 (5)
- 4 Pain ManagmentDocument45 pages4 Pain ManagmentBahar AliNo ratings yet
- TL 1Document4 pagesTL 1ĐôngNo ratings yet
- Pain ManuscriptDocument5 pagesPain ManuscriptGPaolo FauniNo ratings yet
- Axial Low Back Pain One Painful Area - Many Perceptions and Mechanisms - Förster Et Al '13Document8 pagesAxial Low Back Pain One Painful Area - Many Perceptions and Mechanisms - Förster Et Al '13Craig ChambersNo ratings yet
- Hingray 2016Document7 pagesHingray 2016syrieuxNo ratings yet
- Finnerup Et Al 2020 Neuropathic Pain From Mechanisms To TreatmentDocument44 pagesFinnerup Et Al 2020 Neuropathic Pain From Mechanisms To TreatmentintermediosamberesNo ratings yet
- Pain Essay - What Are The Pathways Involved in The Sensation of Pain and How Can We Manipulate Them For Our BenefitDocument5 pagesPain Essay - What Are The Pathways Involved in The Sensation of Pain and How Can We Manipulate Them For Our BenefitscholifyNo ratings yet
- Jop 157 445Document11 pagesJop 157 445Jon SNo ratings yet
- Acupuncture For Musculoskeletal Pain: A Meta-Analysis and Meta-Regression of Sham-Controlled Randomized Clinical TrialsDocument24 pagesAcupuncture For Musculoskeletal Pain: A Meta-Analysis and Meta-Regression of Sham-Controlled Randomized Clinical TrialsValeria Checa Sanchez-CarrionNo ratings yet
- 15-Kip Aaanalgesia Under AnaesthesiaDocument13 pages15-Kip Aaanalgesia Under AnaesthesiagospelcorpNo ratings yet
- Phantom Tooth PainDocument31 pagesPhantom Tooth PainMuchlis Fauzi ENo ratings yet
- Phatofisiology of Pain PDFDocument8 pagesPhatofisiology of Pain PDFmohd nor muhammadNo ratings yet
- PHDDocument309 pagesPHDAndré HipnotistaNo ratings yet
- MPDS-Multifactorial Etiology and Varied Pathophysiology: A ReviewDocument7 pagesMPDS-Multifactorial Etiology and Varied Pathophysiology: A Reviewsnehal jaiswalNo ratings yet
- Claudio Solaro Michele Messmer UccelliDocument12 pagesClaudio Solaro Michele Messmer UccelliEvangelos SpiridonNo ratings yet
- Forensic Hypnosis: Muktesh Chander, IPSDocument7 pagesForensic Hypnosis: Muktesh Chander, IPSPeter PunkyNo ratings yet
- Varieties of Attention in Hypnosis and M PDFDocument4 pagesVarieties of Attention in Hypnosis and M PDFCarlos CondeNo ratings yet
- Yoga-Nidra and HypnosisDocument10 pagesYoga-Nidra and HypnosisCarlos CondeNo ratings yet
- Effect of Hypnotic Suggestion On Fibromy PDFDocument6 pagesEffect of Hypnotic Suggestion On Fibromy PDFCarlos CondeNo ratings yet
- Analgesic HypnosisDocument3 pagesAnalgesic HypnosisCarlos CondeNo ratings yet
- The Forensic Evaluation of Traumatic Brain Injury A Handbook For Clinicians and AttorneysDocument168 pagesThe Forensic Evaluation of Traumatic Brain Injury A Handbook For Clinicians and AttorneysCarlos CondeNo ratings yet
- Thurs 100 Terrace Thompson Sokol CBT Competency 0 PDFDocument34 pagesThurs 100 Terrace Thompson Sokol CBT Competency 0 PDFCarlos CondeNo ratings yet
- 2011 Ten Year Revision of The Brief Behavioral Activation Treatment For Depression Revised Treatment Manual Lejuez Et AlDocument52 pages2011 Ten Year Revision of The Brief Behavioral Activation Treatment For Depression Revised Treatment Manual Lejuez Et AlCarlos CondeNo ratings yet
- Virtual Reality As Treatment For Fear of FlyingDocument8 pagesVirtual Reality As Treatment For Fear of FlyingCarlos CondeNo ratings yet
- Interpersonal Problems, Mindfulness, and Therapy Outcome in An Acceptance-Based Behavior Therapy For Generalized Anxiety DisorderDocument12 pagesInterpersonal Problems, Mindfulness, and Therapy Outcome in An Acceptance-Based Behavior Therapy For Generalized Anxiety DisorderCarlos Conde100% (1)
- Intro to Phenomenological ApproachesDocument11 pagesIntro to Phenomenological ApproachesToshi ToshiNo ratings yet
- Vicarious LiabilityDocument12 pagesVicarious LiabilitySoap MacTavishNo ratings yet
- English Club ConstitutionDocument27 pagesEnglish Club ConstitutionJude Martin AlvarezNo ratings yet
- Child Rights and Juvenile Justice in India MedhaDocument23 pagesChild Rights and Juvenile Justice in India MedhaLaw ColloquyNo ratings yet
- Stigmatization of Feminism: Gender Studies As "Gender Ideology" in Right-Wing Populist Political Discourse in HungaryDocument55 pagesStigmatization of Feminism: Gender Studies As "Gender Ideology" in Right-Wing Populist Political Discourse in HungaryAnubhav SinghNo ratings yet
- Device Test ModeDocument14 pagesDevice Test ModeNay SoeNo ratings yet
- 9th Science Mcqs PTB PDFDocument25 pages9th Science Mcqs PTB PDFUmar JuttNo ratings yet
- Group No 5 - Ultratech - Jaypee 20th Sep-1Document23 pagesGroup No 5 - Ultratech - Jaypee 20th Sep-1Snehal100% (1)
- Visa Vertical and Horizontal Analysis ExampleDocument9 pagesVisa Vertical and Horizontal Analysis Examplechad salcidoNo ratings yet
- KCIS 2nd Semester Science Fair ProjectsDocument2 pagesKCIS 2nd Semester Science Fair ProjectsCaT BlAcKNo ratings yet
- Automotive Plastic Product Design Interview QuestionsDocument13 pagesAutomotive Plastic Product Design Interview QuestionsAbhijith Alolickal100% (2)
- THE HOUSE ON ZAPOTE STREET - Lyka PalerDocument11 pagesTHE HOUSE ON ZAPOTE STREET - Lyka PalerDivine Lyka Ordiz PalerNo ratings yet
- Change Management HRDocument2 pagesChange Management HRahmedaliNo ratings yet
- Plattischemic Stroke Lesson PlanDocument18 pagesPlattischemic Stroke Lesson Planapi-216258123100% (3)
- EN Sample Paper 19 UnsolvedDocument12 pagesEN Sample Paper 19 UnsolvedRashvandhNo ratings yet
- The Tibetan Weather Magic Ritual of A MoDocument13 pagesThe Tibetan Weather Magic Ritual of A MoYORDIS PCNo ratings yet
- Business Plan Template For AfterSchool ProgramsDocument6 pagesBusiness Plan Template For AfterSchool Programsshelana BarzeyNo ratings yet
- Royalstone ReadmeDocument2 pagesRoyalstone ReadmeAdnan BrianNo ratings yet
- Everyman A Structural Analysis Thomas F. Van LaanDocument12 pagesEveryman A Structural Analysis Thomas F. Van LaanRodrigoCarrilloLopezNo ratings yet
- An Introduction To Insurance AccountingDocument86 pagesAn Introduction To Insurance AccountingTricia PrincipeNo ratings yet
- (English (Auto-Generated) ) Reviving The Labor Movement - Margaret Levi - TEDxSeattle (DownSub - Com)Document14 pages(English (Auto-Generated) ) Reviving The Labor Movement - Margaret Levi - TEDxSeattle (DownSub - Com)Surat PEHKTNo ratings yet
- GasGas TXT Racing 2014 Owner's ManualDocument60 pagesGasGas TXT Racing 2014 Owner's Manualstone chouNo ratings yet
- BeadsDocument8 pagesBeadsMukesh MonuNo ratings yet
- Mrs. Dunia Halawi HarbDocument18 pagesMrs. Dunia Halawi HarbsallykamareddineNo ratings yet
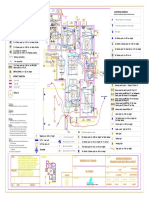
- Varun Valanjeri Electrical Layout-3Document1 pageVarun Valanjeri Electrical Layout-3ANOOP R NAIRNo ratings yet
- An Essay For The Glass Menagerie PDFDocument11 pagesAn Essay For The Glass Menagerie PDFBily ManNo ratings yet
- PDF Penstock Manual DLDocument160 pagesPDF Penstock Manual DLWilmer Fernando DuarteNo ratings yet
- Valvula ContraincendioDocument6 pagesValvula ContraincendiowidNo ratings yet
- 285519-35126-30-case-studyDocument12 pages285519-35126-30-case-studyapi-737834018No ratings yet
- Perceptions of Organizational Structure in The Hospitality IndustryDocument11 pagesPerceptions of Organizational Structure in The Hospitality IndustryLeah Williams100% (1)