You might also like
- Physiotherapy Methods To Facilitate Pelvic Floor Muscle Contraction: A Systematic ReviewDocument14 pagesPhysiotherapy Methods To Facilitate Pelvic Floor Muscle Contraction: A Systematic Reviewsamuel tapia pardoNo ratings yet
- International Journal of Osteopathic Medicine: Jacob Marten Switters, Stefan Podar, Luke Perraton, Zuzana MachotkaDocument8 pagesInternational Journal of Osteopathic Medicine: Jacob Marten Switters, Stefan Podar, Luke Perraton, Zuzana MachotkaElizabeth VivancoNo ratings yet
- Neurourology and Urodynamics - 2023 - B - Can You Breathe Yourself To A Better Pelvic Floor A Systematic ReviewDocument19 pagesNeurourology and Urodynamics - 2023 - B - Can You Breathe Yourself To A Better Pelvic Floor A Systematic ReviewDanielle GadelhaNo ratings yet
- Nau 24097Document9 pagesNau 24097Anonymous ovTI4eNo ratings yet
- Magnetic in Pelvic PainDocument16 pagesMagnetic in Pelvic PainNakarit SangsirinawinNo ratings yet
- Effects of Isometric, Eccentric, or Heavy Slow Resistance Exercises On Pain and Function With PTDocument15 pagesEffects of Isometric, Eccentric, or Heavy Slow Resistance Exercises On Pain and Function With PTTomBramboNo ratings yet
- Relação Entre Diástase Do Músculo Reto Abdominal e Disfunções MúsculoDocument11 pagesRelação Entre Diástase Do Músculo Reto Abdominal e Disfunções MúsculoAdilson MarquesNo ratings yet
- Ughreja Myofascial ReleaseDocument9 pagesUghreja Myofascial Releasecris.endo.ceNo ratings yet
- Oliveira 2007Document8 pagesOliveira 2007Carlos VieiraNo ratings yet
- Rodilla 8Document14 pagesRodilla 8AdosotoNo ratings yet
- Pelvic Floor Muscle Training Protocol For Stress Urinary Incontinence in Women: A Systematic ReviewDocument9 pagesPelvic Floor Muscle Training Protocol For Stress Urinary Incontinence in Women: A Systematic ReviewKarem FernandezNo ratings yet
- ICS Report On The Terminology For Pelvic Floor Muscle Assessment 2021Document44 pagesICS Report On The Terminology For Pelvic Floor Muscle Assessment 2021Rayhan Islam 1915281680No ratings yet
- Clinical Reliability - Middle Trapezius and Gluteus MedioDocument5 pagesClinical Reliability - Middle Trapezius and Gluteus MedioAlberto BeskowNo ratings yet
- Us SR PTJ, 2009Document15 pagesUs SR PTJ, 2009Ju ChangNo ratings yet
- Autonomic Effects of Spinal Manipulative therapie systematic reviewDocument12 pagesAutonomic Effects of Spinal Manipulative therapie systematic reviewbesombespierreNo ratings yet
- Kay M Crossley, Marienke Van Middelkoop, Michael J Callaghan, Natalie J Collins, Michael Skovdal Rathleff, Christian J BartonDocument11 pagesKay M Crossley, Marienke Van Middelkoop, Michael J Callaghan, Natalie J Collins, Michael Skovdal Rathleff, Christian J BartonAugusto SantosNo ratings yet
- Frazzitta Et AlDocument8 pagesFrazzitta Et Alalex ormazabalNo ratings yet
- Interventional Treatment For Myofascial Pelvic Floor...............Document10 pagesInterventional Treatment For Myofascial Pelvic Floor...............Andres MahechaNo ratings yet
- Journal Pre-Proof: Archives of Physical Medicine and RehabilitationDocument38 pagesJournal Pre-Proof: Archives of Physical Medicine and RehabilitationRudolfGerNo ratings yet
- Ijspt 14 845Document15 pagesIjspt 14 845Magno FilhoNo ratings yet
- Abstracts / Manual Therapy 25 (2016) E57 Ee169 E132Document2 pagesAbstracts / Manual Therapy 25 (2016) E57 Ee169 E132NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Neuromuscular Training in PFPS Protocol BMC 2014Document10 pagesNeuromuscular Training in PFPS Protocol BMC 2014Michele GonçalvesNo ratings yet
- Lúcia Spallanzani - Artigo 02Document8 pagesLúcia Spallanzani - Artigo 02Reeduca PelvicNo ratings yet
- Jurnal LBPDocument10 pagesJurnal LBPeka mei dianitaNo ratings yet
- Comparison of Three Types of Exc in The Treatment of Rotator Cuff TendinopathyShoulder Impingement SyndromeDocument7 pagesComparison of Three Types of Exc in The Treatment of Rotator Cuff TendinopathyShoulder Impingement SyndromeKholis RedcrossNo ratings yet
- 0207 ProlotherapyDocument36 pages0207 ProlotherapyRia PuputNo ratings yet
- Effectiveness of Manual Traction and Other Physiotherapy Treatment in The Management of Painful Cervical RadiculopathyDocument5 pagesEffectiveness of Manual Traction and Other Physiotherapy Treatment in The Management of Painful Cervical RadiculopathyAgus Dwiyana NMNo ratings yet
- Ijerph 19 11073Document14 pagesIjerph 19 11073Andreea ManeaNo ratings yet
- 1737 FullDocument9 pages1737 FullSiti RofatulNo ratings yet
- Masseter Muscle Measurement Performed by Ultrasound: A Systematic ReviewDocument9 pagesMasseter Muscle Measurement Performed by Ultrasound: A Systematic ReviewDerya İçözNo ratings yet
- Bjsports 2017 097547Document9 pagesBjsports 2017 097547lujoba1No ratings yet
- Aluko2013 2Document11 pagesAluko2013 2Dr Ahmed NabilNo ratings yet
- Endoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudyDocument6 pagesEndoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudySamuel0651No ratings yet
- Breathing Movements of The Chest and Abdominal Wall in Healthy SubjectsDocument10 pagesBreathing Movements of The Chest and Abdominal Wall in Healthy SubjectsAnandhu GNo ratings yet
- Environmental Research and Public Health: International Journal ofDocument10 pagesEnvironmental Research and Public Health: International Journal ofrestu pangestutiNo ratings yet
- Management Thoracic Pain 2019Document9 pagesManagement Thoracic Pain 2019Lotte WeggemanNo ratings yet
- Thoracic Spine Manipulation For The Management of Mechanical Neck Pain: A Systematic Review and Meta-AnalysisDocument28 pagesThoracic Spine Manipulation For The Management of Mechanical Neck Pain: A Systematic Review and Meta-AnalysisskNo ratings yet
- Effectiveness of Continuous and Pulsed Ultrasound For The Management of Knee Osteoarthritis A Systematic Review and Network Meta-AnalysisDocument10 pagesEffectiveness of Continuous and Pulsed Ultrasound For The Management of Knee Osteoarthritis A Systematic Review and Network Meta-Analysisnuttawat.runNo ratings yet
- JournalDocument15 pagesJournalMuhammad NauvalNo ratings yet
- JBM 2018051810335812Document7 pagesJBM 2018051810335812ARUN VNo ratings yet
- KT Revisão Sistemática, JOP 2014Document10 pagesKT Revisão Sistemática, JOP 2014Ju ChangNo ratings yet
- Pelvic Floor Muscle Training Improves Erectile Dysfunction and Premature Ejaculation A Systematic ReviewDocument9 pagesPelvic Floor Muscle Training Improves Erectile Dysfunction and Premature Ejaculation A Systematic ReviewNatacha CabeteNo ratings yet
- Effectiveness of Myofascial Release in The Management of Plantar Heel PainDocument6 pagesEffectiveness of Myofascial Release in The Management of Plantar Heel PainVeronica Di GiannantonioNo ratings yet
- ABJS Volume 8 Issue 4 Pages 479-501Document23 pagesABJS Volume 8 Issue 4 Pages 479-501Nurul Misna LestariNo ratings yet
- Consenso de Valoracion Dolor Patelofemoral 2016Document5 pagesConsenso de Valoracion Dolor Patelofemoral 2016Guillermo RecioNo ratings yet
- Pelvic Floor and Abdominal Muscle Cocontraction inDocument15 pagesPelvic Floor and Abdominal Muscle Cocontraction inChoirul AkbarNo ratings yet
- An Updated Meta Analysis of Laparoscopic Versus Open Repair For Perforated Peptic UlcerDocument13 pagesAn Updated Meta Analysis of Laparoscopic Versus Open Repair For Perforated Peptic UlcerSANDRA MILENA GUTIERREZ CAÑASNo ratings yet
- Brazilian Journal of Physical TherapyDocument9 pagesBrazilian Journal of Physical TherapyWahdina PratamaNo ratings yet
- Diagnostic Value of Five Clinical Tests in Patellofemoral Pain SyndromeDocument9 pagesDiagnostic Value of Five Clinical Tests in Patellofemoral Pain Syndromesridhar100% (1)
- 1806 3713 Jbpneu 46 03 E20180422Document7 pages1806 3713 Jbpneu 46 03 E20180422Sango AyraNo ratings yet
- Articulo BrasileroDocument8 pagesArticulo BrasileroLuis GalvanNo ratings yet
- Journal of ScienceDocument4 pagesJournal of ScienceEndang SetiawatiNo ratings yet
- Inducción MiofascialDocument11 pagesInducción MiofascialAlison Isabel ValleNo ratings yet
- Patello Femoral TappingDocument9 pagesPatello Femoral TappingainunNo ratings yet
- 2022 Article 14213Document16 pages2022 Article 14213Gabriel DelfinoNo ratings yet
- The Effectiveness of Proprioceptive-Based Exercise For Osteoarthritis of The Knee: A Systematic Review and Meta-AnalysisDocument13 pagesThe Effectiveness of Proprioceptive-Based Exercise For Osteoarthritis of The Knee: A Systematic Review and Meta-AnalysisHifza ArifNo ratings yet
- 1 s2.0 S2214687321000133 MainDocument7 pages1 s2.0 S2214687321000133 MainJuan David Arenas MendozaNo ratings yet
- Hypo PF functionDocument17 pagesHypo PF functionIvan Garcia OsorioNo ratings yet
- Wound Repair Regeneration - 2022 - Qiu - Effects of Physical Activity As An Adjunct Treatment On Healing Outcomes andDocument14 pagesWound Repair Regeneration - 2022 - Qiu - Effects of Physical Activity As An Adjunct Treatment On Healing Outcomes andnathan khendaNo ratings yet
- What Is A PronounDocument9 pagesWhat Is A PronounFanera JefferyNo ratings yet
- Sps 500 (STD) ProgramDocument164 pagesSps 500 (STD) Programwahyu100% (1)
- Quality Assurance in The Manufacture of Light Unmanned Aircraft SystemDocument4 pagesQuality Assurance in The Manufacture of Light Unmanned Aircraft SystemAhmad Zubair RasulyNo ratings yet
- Low Noise Pseudomorphic HEMT Technical DataDocument4 pagesLow Noise Pseudomorphic HEMT Technical Datahendpraz88No ratings yet
- TS68Document52 pagesTS68finandariefNo ratings yet
- Ventilation System Comparison - Constant Air Volume (CAV) and Variable Air Volume (VAV)Document15 pagesVentilation System Comparison - Constant Air Volume (CAV) and Variable Air Volume (VAV)ankurNo ratings yet
- M 200Document3 pagesM 200Rafael Capunpon VallejosNo ratings yet
- Entrepreneurs That Changed The Face of IndiaDocument4 pagesEntrepreneurs That Changed The Face of Indiamarykavitha_6No ratings yet
- GCS Guilford County Schools 2020 Staff Manual Omits Obesity From CDC Covid WarningsDocument26 pagesGCS Guilford County Schools 2020 Staff Manual Omits Obesity From CDC Covid WarningscitizenwellsNo ratings yet
- Conplast SP430Document2 pagesConplast SP430Tori Small100% (1)
- Wrap Book A4Document27 pagesWrap Book A4doscribe100% (1)
- The Suitcase ProjectDocument27 pagesThe Suitcase Projectshubhamkumar9211No ratings yet
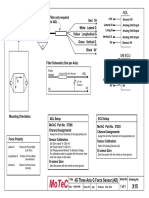
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Online Medicine Industry Competitor AnalysisDocument14 pagesOnline Medicine Industry Competitor Analysispawangadiya1210No ratings yet
- English Try Out UN 1 2008/2009Document4 pagesEnglish Try Out UN 1 2008/2009Cepiana Abas100% (10)
- ASME B16.5 Flange Rating CalculatorDocument10 pagesASME B16.5 Flange Rating Calculatorfaizal100% (2)
- BX10/BX10 MB: Weighing Terminals Technical ManualDocument60 pagesBX10/BX10 MB: Weighing Terminals Technical Manualfelipezambrano50% (2)
- Engineering ManualDocument27 pagesEngineering ManualThousif Rahman67% (3)
- Duarte Et Al - Resin CementsDocument28 pagesDuarte Et Al - Resin Cementsjfrascarolo100% (4)
- Understanding Immunomodulatory DrugsDocument4 pagesUnderstanding Immunomodulatory DrugsMark Russel Sean LealNo ratings yet
- Counter Argument Against Euthanasia (40Document4 pagesCounter Argument Against Euthanasia (40Daphniee PosingNo ratings yet
- 3023 History Cuisine WorksheetDocument6 pages3023 History Cuisine WorksheetFlor HenríquezNo ratings yet
- Uganda National Urban ProfileDocument74 pagesUganda National Urban ProfileUnited Nations Human Settlements Programme (UN-HABITAT)No ratings yet
- Effects of Cutting Classes For Grade 11 TEC Students of AMA Computer College Las PiñasDocument5 pagesEffects of Cutting Classes For Grade 11 TEC Students of AMA Computer College Las PiñasGgssNo ratings yet
- Hyperfunctional Voice DisordersDocument11 pagesHyperfunctional Voice DisordersJam PNo ratings yet
- Iupac 1Document15 pagesIupac 1Mayur Kumar GargNo ratings yet
- MYK Grout Card 2Document2 pagesMYK Grout Card 2Abdul Raheem SyedNo ratings yet
- 4 Dec - Elis Vs ElisDocument6 pages4 Dec - Elis Vs ElisRichard TenorioNo ratings yet
- Blood Bank Case Study 5bDocument2 pagesBlood Bank Case Study 5bbalqis jaberNo ratings yet
- 6 DLL HOPE 3 2019-2020 JulyDocument2 pages6 DLL HOPE 3 2019-2020 JulyCelia BautistaNo ratings yet