You might also like
- Student Grouping Tool: Section Name Mastery Reading Level Status GenderDocument8 pagesStudent Grouping Tool: Section Name Mastery Reading Level Status GendermattboschNo ratings yet
- Planificación Diaria Deberes PDFDocument2 pagesPlanificación Diaria Deberes PDFUxuaNo ratings yet
- HACCP Corrective Action LogDocument1 pageHACCP Corrective Action Logj KiizaNo ratings yet
- HandwritingDocument62 pagesHandwritingIrene fe ResojentoNo ratings yet
- HACCP Thermometer Calibration Log - Maintain Food SafetyDocument1 pageHACCP Thermometer Calibration Log - Maintain Food SafetyArman Al NasarNo ratings yet
- Program Syllabus Level 1 ConversationDocument15 pagesProgram Syllabus Level 1 ConversationMiguel Angel Juárez Estrada0% (1)
- Program Syllabus: Level 1Document4 pagesProgram Syllabus: Level 1Marcela CarpinelliNo ratings yet
- Medical and Surgical History Synact-Cs002Document1 pageMedical and Surgical History Synact-Cs002adriana gutanuNo ratings yet
- Life Skill - Module-9 - I Am RelaxedDocument11 pagesLife Skill - Module-9 - I Am RelaxedSahil ChaudharyNo ratings yet
- Data Presbiakusis Panti Werdha 28 Oktober 2017 NewDocument11 pagesData Presbiakusis Panti Werdha 28 Oktober 2017 NewAmelia GunawanNo ratings yet
- Reporte 1Document1 pageReporte 1Diego EmilianoNo ratings yet
- IMSLP588930 PMLP947525 PIANO Bella - CiaoDocument2 pagesIMSLP588930 PMLP947525 PIANO Bella - Ciaoahmad zulfikar75% (4)
- PCLA Temperature and COVID 19 Symptoms Record 2020-07-01 Ver0Document1 pagePCLA Temperature and COVID 19 Symptoms Record 2020-07-01 Ver0Joecel OlazoNo ratings yet
- FY20 Community VAR OffSite ENG With INSDocument2 pagesFY20 Community VAR OffSite ENG With INSJorge RodriguezNo ratings yet
- 6 Physical Exam Fill AbleDocument2 pages6 Physical Exam Fill AbleKaty SanchezNo ratings yet
- ACUAN kalibrasiDocument5 pagesACUAN kalibrasidody kurniaNo ratings yet
- Acessibilidade Da Pop. C.Delgado: Aldeias Us Distritos Aldeias - Distj 5 10 15 20 25 30Document1 pageAcessibilidade Da Pop. C.Delgado: Aldeias Us Distritos Aldeias - Distj 5 10 15 20 25 30Ryber KalosNo ratings yet
- Dexter Gordon Three O Clock Inn The MorningbbDocument3 pagesDexter Gordon Three O Clock Inn The MorningbbFilipe ValentimNo ratings yet
- Consult Excel SheetDocument7 pagesConsult Excel Sheetanika.w.leeNo ratings yet
- Smoked Salmon Lavash CrostiniDocument2 pagesSmoked Salmon Lavash Crostiniamyluft100% (1)
- DX and TX Protocols RegularDocument24 pagesDX and TX Protocols RegularRaymondNo ratings yet
- Things To Do in HawaiiDocument5 pagesThings To Do in HawaiiRaymondNo ratings yet
- Spe Aler 2016Document43 pagesSpe Aler 2016RaymondNo ratings yet
- Thank You AnchoredDocument1 pageThank You AnchoredRaymondNo ratings yet
- Spe Aler 2016Document43 pagesSpe Aler 2016RaymondNo ratings yet
- CrossiftProgramming June 2016Document31 pagesCrossiftProgramming June 2016Raymond100% (1)
- Clin Chem Lab FinalDocument3 pagesClin Chem Lab FinalRaymondNo ratings yet
- Xray Phys PDFDocument1 pageXray Phys PDFRaymondNo ratings yet
- CrossiftProgramming June 2016Document31 pagesCrossiftProgramming June 2016Raymond100% (1)
- Lower Extremity SlidesDocument14 pagesLower Extremity SlidesRaymondNo ratings yet
- Public Health MT#1Document3 pagesPublic Health MT#1RaymondNo ratings yet
- Crossfit Programming Feb 2016Document22 pagesCrossfit Programming Feb 2016RaymondNo ratings yet
- Lower Extremity SlidesDocument14 pagesLower Extremity SlidesRaymondNo ratings yet
- Public Health MT#1 PDFDocument3 pagesPublic Health MT#1 PDFRaymondNo ratings yet
- RAD ANAT I MT Practice Test Ap2017 PDFDocument11 pagesRAD ANAT I MT Practice Test Ap2017 PDFRaymondNo ratings yet
- DDX Low Back Review 1Document10 pagesDDX Low Back Review 1Raymond100% (1)
- Clin Chem Lab Final PDFDocument2 pagesClin Chem Lab Final PDFRaymondNo ratings yet
- Study Guide For The Thoracic Spine Technique and ManagementDocument5 pagesStudy Guide For The Thoracic Spine Technique and ManagementRaymondNo ratings yet
- Extra Credit Project - Spring 2016Document10 pagesExtra Credit Project - Spring 2016RaymondNo ratings yet
- Study Guide For The Thoracic Spine Technique and ManagementDocument5 pagesStudy Guide For The Thoracic Spine Technique and ManagementRaymondNo ratings yet
- Apom Fuchs (Dens) AP Post Oblique Ant Oblique Measure Filter/Shield SID Tube Angle Film Size ID Position Marker PositioningDocument4 pagesApom Fuchs (Dens) AP Post Oblique Ant Oblique Measure Filter/Shield SID Tube Angle Film Size ID Position Marker PositioningRaymondNo ratings yet
- DX Imaging 3 FinalDocument10 pagesDX Imaging 3 FinalRaymondNo ratings yet
- DDX Low Back Review 1Document10 pagesDDX Low Back Review 1Raymond100% (1)
- Clin Psyche MT2Document4 pagesClin Psyche MT2RaymondNo ratings yet
- DDX CSP MTDocument4 pagesDDX CSP MTRaymondNo ratings yet
- Open and Closed Packed Positions of JointsDocument1 pageOpen and Closed Packed Positions of JointsRaymond100% (4)
- Sample PT exam questions cover tendinopathy, CTS, MRT, balance, plyometricsDocument1 pageSample PT exam questions cover tendinopathy, CTS, MRT, balance, plyometricsRaymondNo ratings yet
- Geriatrics MT: Study Online atDocument7 pagesGeriatrics MT: Study Online atRaymondNo ratings yet
- Ethics Final: Study Online atDocument3 pagesEthics Final: Study Online atRaymondNo ratings yet
- Diff DX LB NotesDocument98 pagesDiff DX LB NotesRaymondNo ratings yet
- Clinical Nurse Judgment Paper 1Document7 pagesClinical Nurse Judgment Paper 1api-594625714No ratings yet
- CaNaMed 2022 - Versiunea 04.11.2021Document266 pagesCaNaMed 2022 - Versiunea 04.11.2021Claudia BlmNo ratings yet
- V ' Exgv 'Vex DG©: Health Insurance Claim FormDocument2 pagesV ' Exgv 'Vex DG©: Health Insurance Claim Formjakaria emtiajNo ratings yet
- Algorithm-PALS Ped Systematic Approach 200615Document1 pageAlgorithm-PALS Ped Systematic Approach 200615Erica Yamamoto100% (1)
- Speaker Dr. Annisa Tridamayanti, SPJP, Fiha Sesi 5Document3 pagesSpeaker Dr. Annisa Tridamayanti, SPJP, Fiha Sesi 5thiadinaNo ratings yet
- Baby Tooth Brushes, Vitamins, Medicines Inventory ManadoDocument2,918 pagesBaby Tooth Brushes, Vitamins, Medicines Inventory ManadoBENAYA TAMBENGINo ratings yet
- SynthesisPaper 1esparagozaDocument13 pagesSynthesisPaper 1esparagozaNewbieNo ratings yet
- Pt. Rania Jaya Farmarindo Daftar Harga Jual PersediaanDocument21 pagesPt. Rania Jaya Farmarindo Daftar Harga Jual PersediaanLalu EyiqNo ratings yet
- SPH Untuk Rsud BKKMDocument57 pagesSPH Untuk Rsud BKKMBagas PutranandaNo ratings yet
- Perfect Tens ManualDocument17 pagesPerfect Tens ManualBea100% (1)
- Raw Data To SDTM ConversionDocument1 pageRaw Data To SDTM ConversionKomalrawal RawalNo ratings yet
- Bio Data Form for Media Unit Alumni (Responses)Document1 pageBio Data Form for Media Unit Alumni (Responses)sojahjessica5No ratings yet
- Epidemiological Characterization of Tibial Plateau FracturesDocument7 pagesEpidemiological Characterization of Tibial Plateau FracturesArmando RodriguezNo ratings yet
- Ethnopharmacological Survey of Medicinal Plants Used in Treating Skin Diseases in The Province of Laguna, PhilippinesDocument10 pagesEthnopharmacological Survey of Medicinal Plants Used in Treating Skin Diseases in The Province of Laguna, PhilippinesMJ ColumbresNo ratings yet
- Handling Difficult Patients at HospitalsDocument2 pagesHandling Difficult Patients at HospitalsAbhi ThamminainaNo ratings yet
- Rajendra Dhawale Training NeedDocument10 pagesRajendra Dhawale Training NeedKunal PadamwarNo ratings yet
- Cold or Tepid Sponge BathDocument1 pageCold or Tepid Sponge BathJEROME CHRISTIAN ALMINAZANo ratings yet
- Fees and Charges - Summary From 1 July 2020 Version 1.0, June 2020Document51 pagesFees and Charges - Summary From 1 July 2020 Version 1.0, June 2020QualityMattersNo ratings yet
- DownloadDocument8 pagesDownloadGUILHERME DAS CHAGAS DE SOUSANo ratings yet
- Biology Kondez 3-4pmDocument3 pagesBiology Kondez 3-4pmQuezanda OndezNo ratings yet
- Assessment Guide: CHCCOM005 Communicate and Work in Health or Community ServicesDocument18 pagesAssessment Guide: CHCCOM005 Communicate and Work in Health or Community ServicesSamir Bhandari100% (1)
- Hafod Livery AgreementDocument10 pagesHafod Livery Agreementrgcy6dw6vgNo ratings yet
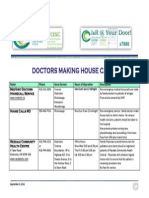
- Doctors Making House CallsDocument1 pageDoctors Making House Callspenthouse2No ratings yet
- Manual of Standards For Blood Collection Units in The PhilippinesDocument89 pagesManual of Standards For Blood Collection Units in The PhilippinesBlue PielagoNo ratings yet
- Anti-inflammatory Activity of Mangifera casturi FruitDocument6 pagesAnti-inflammatory Activity of Mangifera casturi FruitrabiatulNo ratings yet
- Health Checklist Form: (Nakakaranas Ka Ba NG:) (Pananakit NG Lalamunan / Masakit Lumunok)Document1 pageHealth Checklist Form: (Nakakaranas Ka Ba NG:) (Pananakit NG Lalamunan / Masakit Lumunok)Jhon Micheal AlicandoNo ratings yet
- Historia de Las Venopunciones Perifericas AMRivera ActaAnaesthBelg2005Document12 pagesHistoria de Las Venopunciones Perifericas AMRivera ActaAnaesthBelg2005Luis CruzNo ratings yet
- Bbraun - Urimed-Bag-BrochureDocument6 pagesBbraun - Urimed-Bag-BrochureCampaign MediaNo ratings yet
- Operating Room Form (Major and Minor) : University of The VisayasDocument16 pagesOperating Room Form (Major and Minor) : University of The VisayasJohn Mitchelle NNo ratings yet
- Silness-Löe Plaque Index ExplainedDocument3 pagesSilness-Löe Plaque Index Explainednuniatmanda100% (1)