You might also like
- Diabetes Mellitus-I: Garis Besar Kuliah Untuk Mahasiswa Semester-6 Fakultas Kedokteran Universitas Airlangga, SurabayaDocument40 pagesDiabetes Mellitus-I: Garis Besar Kuliah Untuk Mahasiswa Semester-6 Fakultas Kedokteran Universitas Airlangga, Surabaya'ifa Iffa100% (4)
- ModyDocument6 pagesModyandriopaNo ratings yet
- Pag 10Document11 pagesPag 10Jesús Adolfo Alarcón GómezNo ratings yet
- JFMK 05 00070 v2Document11 pagesJFMK 05 00070 v2Santy OktavianiNo ratings yet
- Hansen 2016 Impact of Endurance Exercise Training in The Fasted StateDocument14 pagesHansen 2016 Impact of Endurance Exercise Training in The Fasted StateYo Vivo Fit Pablo y KarlaNo ratings yet
- Clinical Aspects of Physical Exercise For Diabetes/metabolic SyndromeDocument5 pagesClinical Aspects of Physical Exercise For Diabetes/metabolic SyndromecokimasterNo ratings yet
- Research Article: Acute Whole Body Vibration Decreases The Glucose Levels in Elderly Diabetic WomenDocument8 pagesResearch Article: Acute Whole Body Vibration Decreases The Glucose Levels in Elderly Diabetic WomenStefanny AmahorsejaNo ratings yet
- Apnm 2014 0357Document8 pagesApnm 2014 0357adri20121989No ratings yet
- Clinical Aspects of Physical Exercise For Diabetes/metabolic SyndromeDocument5 pagesClinical Aspects of Physical Exercise For Diabetes/metabolic Syndromeprofesi nersNo ratings yet
- Exercise Intervention Under Hypoxic Condition As A New TherapeuticDocument14 pagesExercise Intervention Under Hypoxic Condition As A New TherapeuticnorazmiNo ratings yet
- 673 FullDocument4 pages673 FullIba SuprasabaNo ratings yet
- InglesDocument6 pagesInglesKuroKy KrausserNo ratings yet
- Diet and TherapyDocument3 pagesDiet and TherapyKatty AlevonNo ratings yet
- Babu-Positive Effects of Exercise Intervention Without Weight Loss 2021Document28 pagesBabu-Positive Effects of Exercise Intervention Without Weight Loss 2021markwsheppardhotmail.comNo ratings yet
- Malaysia JurnalDocument7 pagesMalaysia JurnalYuli RinawatiNo ratings yet
- Exercise and Adlib Eating in Obese Individuals Med Sci Sports Med Nov 2010Document8 pagesExercise and Adlib Eating in Obese Individuals Med Sci Sports Med Nov 2010Andrew OgundeleNo ratings yet
- JurnalDocument30 pagesJurnalnurul sya'binNo ratings yet
- Metabolic Risk Management, Physical Exercise and Lifestyle Counselling in Low-Active Adults: Controlled Randomized Trial (BELLUGAT)Document15 pagesMetabolic Risk Management, Physical Exercise and Lifestyle Counselling in Low-Active Adults: Controlled Randomized Trial (BELLUGAT)adrianNo ratings yet
- Editorial Article Exercise and Diabetes Mellitus: Polikandrioti MDocument2 pagesEditorial Article Exercise and Diabetes Mellitus: Polikandrioti Mladawantham_58372076No ratings yet
- The Effect of Walking Exercise On Blood Pressure and Blood Glucose in The ElderlyDocument6 pagesThe Effect of Walking Exercise On Blood Pressure and Blood Glucose in The ElderlyadindaNo ratings yet
- Functional High Intensity Exercise Training Ameliorates Insulin Resistance and Cardiometabolic Risk Factors in Type 2 DiabetesDocument22 pagesFunctional High Intensity Exercise Training Ameliorates Insulin Resistance and Cardiometabolic Risk Factors in Type 2 DiabetesDavid Ruiz GonzalezNo ratings yet
- Exercise and Type 2 Diabetes: Molecular Mechanisms Regulating Glucose Uptake in Skeletal MuscleDocument7 pagesExercise and Type 2 Diabetes: Molecular Mechanisms Regulating Glucose Uptake in Skeletal MuscleArie AnggaNo ratings yet
- Progressive Muscle Relaxation (PMR) Is Effective To Lower Blood Glucose Levels of Patients With Type 2 Diabetes MellitusDocument7 pagesProgressive Muscle Relaxation (PMR) Is Effective To Lower Blood Glucose Levels of Patients With Type 2 Diabetes Mellituseno wijayaNo ratings yet
- Progressive Muscle Relaxation (PMR) Is Effective To Lower Blood Glucose Levels of Patients With Type 2 Diabetes MellitusDocument7 pagesProgressive Muscle Relaxation (PMR) Is Effective To Lower Blood Glucose Levels of Patients With Type 2 Diabetes Mellituseno wijayaNo ratings yet
- Progressive Muscle Relaxation (PMR) Is Effective To Lower Blood Glucose Levels of Patients With Type 2 Diabetes MellitusDocument7 pagesProgressive Muscle Relaxation (PMR) Is Effective To Lower Blood Glucose Levels of Patients With Type 2 Diabetes MellitusNada SaskiaNo ratings yet
- Exercise CGM EASD Position Statement - FinalDocument72 pagesExercise CGM EASD Position Statement - FinalPatricia PalenqueNo ratings yet
- The Effect of High Intensity Physical Exercise and Hypoxia On Glycemia, Angiogenic Biomarkers and Cardiorespiratory Function in Patients With Type 1 DiabetesDocument9 pagesThe Effect of High Intensity Physical Exercise and Hypoxia On Glycemia, Angiogenic Biomarkers and Cardiorespiratory Function in Patients With Type 1 DiabetesRicky BooyNo ratings yet
- Physiology & Behavior: SciencedirectDocument8 pagesPhysiology & Behavior: SciencedirectScottNo ratings yet
- DANTAS 2020 Exercise-Induced Increases in Insulin Sensitivity After Bariatric Surgery Are Mediated by Muscle Extracellular Matrix RemodelingDocument17 pagesDANTAS 2020 Exercise-Induced Increases in Insulin Sensitivity After Bariatric Surgery Are Mediated by Muscle Extracellular Matrix RemodelingCris AquinoNo ratings yet
- Aerobic WalkingDocument17 pagesAerobic WalkingKedokteran Komunitas21No ratings yet
- Efectos Del Ejercicio en Pacientes Mayores Con Diabetes ECADocument13 pagesEfectos Del Ejercicio en Pacientes Mayores Con Diabetes ECAAndrés Araneda VásquezNo ratings yet
- Effects of Exercise Modality On Insulin Resistance and Ectopic Fat in Adolescents With Overweight and Obesity A Randomized Clinical Trial - PMCDocument19 pagesEffects of Exercise Modality On Insulin Resistance and Ectopic Fat in Adolescents With Overweight and Obesity A Randomized Clinical Trial - PMCKevin TorresNo ratings yet
- The Essential Role of Exercise in The Management of Type 2 DiabetesDocument11 pagesThe Essential Role of Exercise in The Management of Type 2 DiabetesRadu MaricicaNo ratings yet
- Resistance Training Is An Effective Tool Against Metabolic and Frailty SyndromesDocument7 pagesResistance Training Is An Effective Tool Against Metabolic and Frailty SyndromesgiannidietNo ratings yet
- Physical Activity Prevalence and Barriers Among Type 2 Diabetic Patients, Kudai and Al-Hijra Primary Health Care Center, Makkah, Saudi ArabiaDocument9 pagesPhysical Activity Prevalence and Barriers Among Type 2 Diabetic Patients, Kudai and Al-Hijra Primary Health Care Center, Makkah, Saudi ArabiaIJAR JOURNALNo ratings yet
- Exercise - Physical Activity in Individuals With Type 2 Diabet... - Medicine & Science in Sports & ExerciseDocument51 pagesExercise - Physical Activity in Individuals With Type 2 Diabet... - Medicine & Science in Sports & ExerciseRicardo Arellano GarcíaNo ratings yet
- Rehabilitation in Diabetic Patients.: PmidDocument3 pagesRehabilitation in Diabetic Patients.: PmidIoana PiticarNo ratings yet
- Lakka 2007Document13 pagesLakka 2007Neha RauhilaNo ratings yet
- Exercise and Type 2 DiabetesDocument15 pagesExercise and Type 2 Diabetespb.nakulaNo ratings yet
- The Importance of Exercise For Glycemic Control in Type 2 DiabetesDocument10 pagesThe Importance of Exercise For Glycemic Control in Type 2 DiabetesAhmed AmerNo ratings yet
- 2018 Timing of Exercise Affects Glycemic Control in Type 2 DiabetesDocument9 pages2018 Timing of Exercise Affects Glycemic Control in Type 2 DiabetesdilloniarbzNo ratings yet
- Lifestyle Modification: Weight Control, Exercise, and Smoking CessationDocument12 pagesLifestyle Modification: Weight Control, Exercise, and Smoking CessationsenthilNo ratings yet
- Nutrients 15 01174 v2Document12 pagesNutrients 15 01174 v2Rosmery SalasNo ratings yet
- MISS. MODERATE. Superior Quanto Á Insulina. The Effect of Vigorous - Versus Moderate-Intensity Aerobic Exercise On Insulin Action. Mcgarrah2016Document6 pagesMISS. MODERATE. Superior Quanto Á Insulina. The Effect of Vigorous - Versus Moderate-Intensity Aerobic Exercise On Insulin Action. Mcgarrah2016Paolo AltoéNo ratings yet
- Colberg 2009 2511457365Document8 pagesColberg 2009 2511457365fedelarru9No ratings yet
- Effects of Exercise On Insulin Sensitivity in Humans: John T. Devlin, MDDocument4 pagesEffects of Exercise On Insulin Sensitivity in Humans: John T. Devlin, MDgod4alllNo ratings yet
- Jurnal GerontikDocument8 pagesJurnal GerontikLIZBETH FEMMIL SAPUTRINo ratings yet
- Effects of Endurance Exercise and Vitamin D Supplementation On Insulin Resistance and Plasma Lipidome in Middle-Aged Adults With Type 2 DiabetesDocument19 pagesEffects of Endurance Exercise and Vitamin D Supplementation On Insulin Resistance and Plasma Lipidome in Middle-Aged Adults With Type 2 DiabetesFransiska FranshuidNo ratings yet
- Moving Toward Precision Medicine With Diabetes, ExDocument1 pageMoving Toward Precision Medicine With Diabetes, ExGustavo DelgadoNo ratings yet
- Physiotherapy DiabetesDocument5 pagesPhysiotherapy DiabetessalmanmohammedNo ratings yet
- Physical Activity For HealthDocument10 pagesPhysical Activity For HealthMaria Julia Ogna EgeaNo ratings yet
- 5 ArticuloDocument3 pages5 ArticuloKarina AngelNo ratings yet
- Lindberg 2018Document8 pagesLindberg 2018Elan R.S.No ratings yet
- Lee 2012Document6 pagesLee 2012jhomarlaiNo ratings yet
- Effectiveness and Safety of High-Intensity Interval Training in Patients With Type 2 DiabetesDocument6 pagesEffectiveness and Safety of High-Intensity Interval Training in Patients With Type 2 DiabetesMumtaz Maulana HidayatNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument7 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsGabriel GursenNo ratings yet
- 2 Diet, Exercise, and Pharmacotherapy For Sarcopenia in People With DiabetesDocument12 pages2 Diet, Exercise, and Pharmacotherapy For Sarcopenia in People With DiabetesPaola alvarezNo ratings yet
- HolidaysDocument12 pagesHolidaysGabriela PopescuNo ratings yet
- Concurrent TrainingDocument12 pagesConcurrent Trainingfelipe diazNo ratings yet
- Effectiveness of Acupressure at The Zusanli (ST-36) Acupoint As A Comfortable Treatment For Diabetes Mellitus: A Pilot Study in IndonesiaDocument8 pagesEffectiveness of Acupressure at The Zusanli (ST-36) Acupoint As A Comfortable Treatment For Diabetes Mellitus: A Pilot Study in IndonesiaSebastiano SerraNo ratings yet
- Exercise in Children and Adolescents With Diabetes: ISPAD Clinical Practice Consensus Guidelines 2009 CompendiumDocument15 pagesExercise in Children and Adolescents With Diabetes: ISPAD Clinical Practice Consensus Guidelines 2009 CompendiumAzul MarinoNo ratings yet
- EMRO COVID 19 National Survey Package RecordOfAchievementDocument1 pageEMRO COVID 19 National Survey Package RecordOfAchievementKamal JindalNo ratings yet
- Kamaldeep Jindal ResumeDocument1 pageKamaldeep Jindal ResumeKamal JindalNo ratings yet
- Kamaldeep Jindal ResumeDocument1 pageKamaldeep Jindal ResumeKamal JindalNo ratings yet
- Kamaldeep Jindal ResumeDocument1 pageKamaldeep Jindal ResumeKamal JindalNo ratings yet
- السكر والبوتاسيومDocument2 pagesالسكر والبوتاسيومdr.Hamsa FaridNo ratings yet
- Comparative Study of Change of Hba1C With Voglibose and Teneligliptin On Ongoing Metformin MonotherapyDocument6 pagesComparative Study of Change of Hba1C With Voglibose and Teneligliptin On Ongoing Metformin MonotherapyUttam BasakNo ratings yet
- DKA ProtocolDocument3 pagesDKA Protocolpinky222255554100% (1)
- Diabetes Students Fall21Document59 pagesDiabetes Students Fall21Ismael SerunjogiNo ratings yet
- 1-Insulin-Review 2019Document11 pages1-Insulin-Review 2019eki_herawatiNo ratings yet
- Antidiabetic Drug PDFDocument91 pagesAntidiabetic Drug PDFAlifia ainushNo ratings yet
- How To Completely Reverse Diabetes in As Little As 14 Days + 7 Bonuses (PDFDrive)Document537 pagesHow To Completely Reverse Diabetes in As Little As 14 Days + 7 Bonuses (PDFDrive)Kannammal SampathkumarNo ratings yet
- Types of Insulin: NOTE: Exact Onset, Action, and Duration Are Dependent On The Generic/brand UsedDocument3 pagesTypes of Insulin: NOTE: Exact Onset, Action, and Duration Are Dependent On The Generic/brand Usedask1400No ratings yet
- dm2 Non-InsulinDocument38 pagesdm2 Non-Insulinapi-649066372No ratings yet
- Nutrition and Chronic ConditionsDocument228 pagesNutrition and Chronic ConditionsLeni PurbasariNo ratings yet
- Concept 012 Glucose Regulation GiddensDocument19 pagesConcept 012 Glucose Regulation GiddensangieswensonNo ratings yet
- Diabetes MellitusDocument59 pagesDiabetes Mellituslailatul rofiahNo ratings yet
- Vertex Announces Positive Day 90 Data For The First Patient in The Phase 1 - 2 Clinical Trial Dosed With VX-880, A Novel Investigational Stem Cell-Derived Therapy For The Treatment of Type 1 DiabetesDocument3 pagesVertex Announces Positive Day 90 Data For The First Patient in The Phase 1 - 2 Clinical Trial Dosed With VX-880, A Novel Investigational Stem Cell-Derived Therapy For The Treatment of Type 1 Diabetesዘረአዳም ዘመንቆረርNo ratings yet
- Module EpidemiologiDocument7 pagesModule EpidemiologiTheodora Ferminarti JatyNo ratings yet
- Interpretation: S03 - FPSC DILSHAD COLONY (C004263143) J-50 Dilshad Colony, DelhiDocument6 pagesInterpretation: S03 - FPSC DILSHAD COLONY (C004263143) J-50 Dilshad Colony, DelhiAll VIDEOS TechNo ratings yet
- Diabetes/Understand-Your-Risk-for-Diabetes UCM 002034 Article JSPDocument2 pagesDiabetes/Understand-Your-Risk-for-Diabetes UCM 002034 Article JSPCita Laelika NovialiantiNo ratings yet
- Teaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIDocument3 pagesTeaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIkasjdkasNo ratings yet
- GlyburideDocument3 pagesGlyburideapi-3797941No ratings yet
- A Case Presentation On Diabetic KetoacidosisDocument13 pagesA Case Presentation On Diabetic Ketoacidosisrenie3245No ratings yet
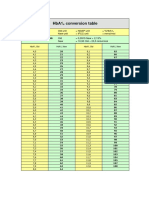
- HbA1cConversionTable PDFDocument1 pageHbA1cConversionTable PDFDarkoMaxNo ratings yet
- Insulin Drug StudyDocument2 pagesInsulin Drug StudyAziil Liiza100% (2)
- Leaflet-Befach Low GI White Rice From Essentials by AmwayDocument13 pagesLeaflet-Befach Low GI White Rice From Essentials by AmwayJordan harishNo ratings yet
- DiabeticwhitepapernamesDocument77 pagesDiabeticwhitepapernamesManishNo ratings yet
- BPT GTT & Diabetes MellitusDocument25 pagesBPT GTT & Diabetes MellitusBalajiNo ratings yet
- Ferrans and Powers Quality of Life Index Diabetes Version - IiiDocument4 pagesFerrans and Powers Quality of Life Index Diabetes Version - IiiDaniela IpateNo ratings yet
- RINGKASAN Kti MawapresDocument2 pagesRINGKASAN Kti MawapresdwiNo ratings yet
- GP Kaunseling 2019 Isbn FinalDocument90 pagesGP Kaunseling 2019 Isbn FinalAtiqah RamzanNo ratings yet
- Drugs Used To Treat Diabetes - MellitusDocument37 pagesDrugs Used To Treat Diabetes - MellitusjisooNo ratings yet