You might also like
- GIT DisordersDocument171 pagesGIT DisordersKatrina PonceNo ratings yet
- Obstacles On The Path of YogaDocument5 pagesObstacles On The Path of YogaYogacharya Dr Ananda Balayogi Bhavanani100% (2)
- Foam SclerotherapyDocument30 pagesFoam SclerotherapyRMR100% (1)
- Pranayama & The Art of BreathingDocument16 pagesPranayama & The Art of BreathingAnurrag KumarNo ratings yet
- PHYSIOLOGY AND PATHOLOGY OF DEFECATIONDocument57 pagesPHYSIOLOGY AND PATHOLOGY OF DEFECATIONMonica BellyndaNo ratings yet
- Fecal Elimination EnemaDocument5 pagesFecal Elimination EnemaVia Kristel ZapantaNo ratings yet
- Tips To Diagnose & Address Common Horse AilmentsDocument6 pagesTips To Diagnose & Address Common Horse AilmentsMark GebhardNo ratings yet
- Lecture 15 Bowl EliminationDocument72 pagesLecture 15 Bowl EliminationIsbelNo ratings yet
- Delivering Better Oral HealthDocument102 pagesDelivering Better Oral Healthsavrasx100% (1)
- Standard Treatment GuidelinesDocument468 pagesStandard Treatment GuidelinesHarshit ChempallilNo ratings yet
- Understanding ConstipationDocument10 pagesUnderstanding ConstipationAndy PurnomoNo ratings yet
- Irritable Bowel SyndromeDocument22 pagesIrritable Bowel SyndromeMarium NabeelNo ratings yet
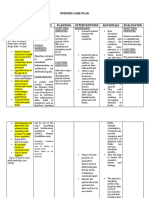
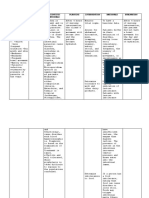
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrahNo ratings yet
- Cholecystitis and CholelithiasisDocument19 pagesCholecystitis and CholelithiasisChristine Salimbagat100% (1)
- NCM 116 W1 Reading HandoutDocument13 pagesNCM 116 W1 Reading Handoutriza sarmientoNo ratings yet
- ConstipationDocument4 pagesConstipationprincess_bee100% (1)
- NCM 116 - GIT (MODULE 5 Part II)Document6 pagesNCM 116 - GIT (MODULE 5 Part II)Meryville JacildoNo ratings yet
- KONSTIPASIDocument33 pagesKONSTIPASIalhidayahNo ratings yet
- DiareDocument5 pagesDiarefarisNo ratings yet
- Bowel Elimination and Urinary Incontinence ProblemsDocument5 pagesBowel Elimination and Urinary Incontinence ProblemsMegan Rose MontillaNo ratings yet
- 4 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionDocument10 pages4 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionKylle AlimosaNo ratings yet
- A. Related FactorsDocument10 pagesA. Related FactorsEva YuliaNo ratings yet
- Diarrhea (Diare)Document9 pagesDiarrhea (Diare)Eki MegaraniNo ratings yet
- Article 1540977249Document14 pagesArticle 1540977249merissa iglesias100% (1)
- Constipation: Jan M. ShoenbergerDocument5 pagesConstipation: Jan M. ShoenbergerS100% (1)
- Irritable Bowel Syndrome GuideDocument7 pagesIrritable Bowel Syndrome GuideHisyam DinGanuNo ratings yet
- ConstipationDocument22 pagesConstipationOsama ALGabriNo ratings yet
- Nursing management of acute gastrointestinal disordersDocument20 pagesNursing management of acute gastrointestinal disorderswyneNo ratings yet
- (Roselle Balicas) - Chrome - LNKDocument8 pages(Roselle Balicas) - Chrome - LNKRose CasBalNo ratings yet
- Gastrointestinal System: Diseases of The Digestive SystemDocument7 pagesGastrointestinal System: Diseases of The Digestive SystemhadrilkaNo ratings yet
- Constipation Diarrhea Fecal IncontinenceDocument40 pagesConstipation Diarrhea Fecal IncontinenceLiza Marie IgnacioNo ratings yet
- Digestive System DisordersDocument117 pagesDigestive System DisordersSusan Batan BandongNo ratings yet
- 7 - ET - LECT - Dietary ManagementDocument3 pages7 - ET - LECT - Dietary ManagementMa Ellen LumauagNo ratings yet
- Constipation and Bowel Obstructions PP Rat 10.2020Document20 pagesConstipation and Bowel Obstructions PP Rat 10.2020Vaidya M.R. PoornimaNo ratings yet
- Risk For Constipation-Cancer Nursing Care PlanDocument1 pageRisk For Constipation-Cancer Nursing Care PlanRnspeakcomNo ratings yet
- Constipation: Patient Name: Shehzad Age: 45 Ward: Emergency BDocument2 pagesConstipation: Patient Name: Shehzad Age: 45 Ward: Emergency BShafiq Ur RahmanNo ratings yet
- PHCP Lec Topic 4 To 10Document19 pagesPHCP Lec Topic 4 To 10armand bayoranNo ratings yet
- Understanding Medical Surgical Nursing (2) - 0001-0001Document1 pageUnderstanding Medical Surgical Nursing (2) - 0001-0001Anas TasyaNo ratings yet
- Case Study On DiarrheaDocument4 pagesCase Study On DiarrheaDalene Erika GarbinNo ratings yet
- ConstipationDocument12 pagesConstipationfrechel kimNo ratings yet
- Constipation (Sembelit)Document8 pagesConstipation (Sembelit)Eki MegaraniNo ratings yet
- MIDTERMSDocument24 pagesMIDTERMSCherish Marie HurbodaNo ratings yet
- Constipation and Bowel Obstructions PP Rat 10.2020Document26 pagesConstipation and Bowel Obstructions PP Rat 10.2020Osman Bin SaifNo ratings yet
- Unit Ix: Nursing Management of Patients With Gi Disorders: Topic: DiarrheaDocument13 pagesUnit Ix: Nursing Management of Patients With Gi Disorders: Topic: Diarrheaayushi rainaNo ratings yet
- Healthful Practices That Affect The Digestive System andDocument16 pagesHealthful Practices That Affect The Digestive System andNovie Jane HontiverosNo ratings yet
- Management of Patients With Intestinal and RectaldisordersDocument16 pagesManagement of Patients With Intestinal and RectaldisordersintotheunknownNo ratings yet
- Chronic Diarrhoea SaqlainDocument116 pagesChronic Diarrhoea SaqlainMohammed SaqlainNo ratings yet
- Nutrition Imbalance NCPDocument1 pageNutrition Imbalance NCPmawelNo ratings yet
- Constipation LeukemiaDocument1 pageConstipation LeukemiamawelNo ratings yet
- 22 Manuscript Intestinal ObstructionDocument8 pages22 Manuscript Intestinal Obstructionkint manlangitNo ratings yet
- p2277 PDFDocument8 pagesp2277 PDFGoran TomićNo ratings yet
- 9 Intestinal ObstructionDocument7 pages9 Intestinal ObstructionMAH pedNo ratings yet
- Daud Khan 1045Document31 pagesDaud Khan 1045Iqra BatoolNo ratings yet
- Diarrhea NCP Pedia WardDocument4 pagesDiarrhea NCP Pedia WardKyle DapulagNo ratings yet
- Consti Pati On: Evaluati On and Management: by Bhairvi Jani, MD & Elizabeth Marsicano, MDDocument5 pagesConsti Pati On: Evaluati On and Management: by Bhairvi Jani, MD & Elizabeth Marsicano, MDsavitri geminiNo ratings yet
- Pathophysiology of Acute DiarrheaDocument3 pagesPathophysiology of Acute DiarrheaFabiana TorresNo ratings yet
- NCM116 Prelim Week 1Document15 pagesNCM116 Prelim Week 1Loungayvan BatuyogNo ratings yet
- New Intestinal ObstructionDocument12 pagesNew Intestinal Obstructionmustafalotfy01No ratings yet
- Fecal EliminationDocument4 pagesFecal EliminationEzra MaeNo ratings yet
- Group 4 Case Presentation DiarrheaDocument46 pagesGroup 4 Case Presentation DiarrheaEphraim John QuichoNo ratings yet
- Age NCPDocument3 pagesAge NCPMartin Allen ClaudioNo ratings yet
- GI SlidesDDM1Document39 pagesGI SlidesDDM1Anonymous d3qpXcm4xVNo ratings yet
- Childhood Constipation: BackgroundDocument5 pagesChildhood Constipation: BackgroundJihan FaadhilahNo ratings yet
- CONTENTDocument17 pagesCONTENTEromobor OnobunNo ratings yet
- Constipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationFrom EverandConstipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationNo ratings yet
- Midterms - Electrolyte Renal DisordersDocument40 pagesMidterms - Electrolyte Renal DisordersRachelle DelantarNo ratings yet
- SummerTerm TopicOutline1Document20 pagesSummerTerm TopicOutline1Rachelle DelantarNo ratings yet
- Research BSN3G SetA Group1FINALDocument75 pagesResearch BSN3G SetA Group1FINALRachelle DelantarNo ratings yet
- NCM 116 G.I Trans Group 2Document30 pagesNCM 116 G.I Trans Group 2Rachelle DelantarNo ratings yet
- NCM116 Finals Assessment of The Nervous SystemDocument9 pagesNCM116 Finals Assessment of The Nervous SystemRachelle DelantarNo ratings yet
- Hemorraghic StrokeDocument4 pagesHemorraghic StrokeRachelle Delantar100% (1)
- Effectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisDocument9 pagesEffectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisrebeca paulinoNo ratings yet
- Liver Case - Hepatic ToxicologyDocument2 pagesLiver Case - Hepatic Toxicologysaya001No ratings yet
- Peripheral Vascular System Anatomy Exam TechniquesDocument2 pagesPeripheral Vascular System Anatomy Exam TechniquesAngelica Mae Dela CruzNo ratings yet
- One Form Should Be Completed by An Adult Member of Each Family. Print in Capital (UPPERCASE) Letters. Leave Blank Boxes For SpacesDocument1 pageOne Form Should Be Completed by An Adult Member of Each Family. Print in Capital (UPPERCASE) Letters. Leave Blank Boxes For SpacesDiana CharvinskayaNo ratings yet
- Chapter 6 - Nutrition (Part 1)Document41 pagesChapter 6 - Nutrition (Part 1)Ema FatimahNo ratings yet
- Genetic Analysis An Integrated Approach 2nd Edition Sanders Test BankDocument15 pagesGenetic Analysis An Integrated Approach 2nd Edition Sanders Test Bankjenniferedwardsmpnidwyjkb100% (48)
- Freelesson1endhairloss EulastversionDocument7 pagesFreelesson1endhairloss EulastversionDezant MiradzNo ratings yet
- Vitamins enable body processes and energy useDocument70 pagesVitamins enable body processes and energy usecon_orenseNo ratings yet
- AHP Matlab software calculates weights for network analysisDocument9 pagesAHP Matlab software calculates weights for network analysisAllahyarNo ratings yet
- Instructional PlanningDocument3 pagesInstructional PlanningRadino Bryan C. SardidoNo ratings yet
- Respiratory Effects of Amyotrophic Lateral Sclerosis, Problems and SolutionsDocument14 pagesRespiratory Effects of Amyotrophic Lateral Sclerosis, Problems and SolutionsMarcelaNo ratings yet
- Vet Pathol 2011 2011 ACVP Annual Meeting E1 E51Document52 pagesVet Pathol 2011 2011 ACVP Annual Meeting E1 E51Haroon RashidNo ratings yet
- The Design and Synthesis of Novel BarbituratesDocument333 pagesThe Design and Synthesis of Novel BarbituratesLucas Timmer100% (1)
- Conservative TreatmentDocument30 pagesConservative TreatmentAlessandro AnceschiNo ratings yet
- 3 Steps To Reverse Aging 1Document3 pages3 Steps To Reverse Aging 1santosh MaliNo ratings yet
- Mercaptan Fact SheetDocument6 pagesMercaptan Fact SheetPravin GowardunNo ratings yet
- EM200 Clerkship Packet - November, 2012Document139 pagesEM200 Clerkship Packet - November, 2012jtsk2No ratings yet
- A Project Report On Banana PlantationDocument10 pagesA Project Report On Banana Plantationkim shinNo ratings yet
- Tuesday, December 09, 2014 EditionDocument16 pagesTuesday, December 09, 2014 EditionFrontPageAfricaNo ratings yet
- Adaptation For Life After Birth A Review of Neonatal PhysiologyDocument9 pagesAdaptation For Life After Birth A Review of Neonatal PhysiologyGrifanda HumairahNo ratings yet
- Ectopic Pregnancy - CSDocument14 pagesEctopic Pregnancy - CSMASII100% (1)
- Infant Formulas. Pediatr Rev 2011Document13 pagesInfant Formulas. Pediatr Rev 2011Zeniff ArciveNo ratings yet
- COVID-19 Reflection - Pengosro, YzahDocument5 pagesCOVID-19 Reflection - Pengosro, Yzahyzah graceNo ratings yet
- Utah KidneyDocument16 pagesUtah KidneyChristineGonzalesNo ratings yet