You might also like
- Manajemen StrokeDocument253 pagesManajemen StrokeHappy Pramanda100% (2)
- Fulminant Myocarditis (Springer, 2022)Document375 pagesFulminant Myocarditis (Springer, 2022)Phuoc NguyenNo ratings yet
- Transalveolar Extraction of The Mandibular Third MolarsDocument221 pagesTransalveolar Extraction of The Mandibular Third MolarsTheo_96No ratings yet
- Quick Guide To Paedriatric Cardiopulmonary CareDocument258 pagesQuick Guide To Paedriatric Cardiopulmonary CareLouvern MoodleyNo ratings yet
- 7172.ALL CardioQuickGuide 9Document95 pages7172.ALL CardioQuickGuide 9jan.headley9915No ratings yet
- Nursing Care Plan For HypertensionDocument5 pagesNursing Care Plan For Hypertensionanon_9189425950% (2)
- CPG Unstable AnginaDocument58 pagesCPG Unstable AnginaAmir HassenNo ratings yet
- Pathophysiology of CVADocument7 pagesPathophysiology of CVAsarzlasco0967% (3)
- Degenerate FibroidDocument3 pagesDegenerate FibroidYuuki Chitose (tai-kun)No ratings yet
- Autism BrahmiDocument3 pagesAutism BrahmiOlga RodriguesNo ratings yet
- 7-Steps For DI Systematic ApproachDocument8 pages7-Steps For DI Systematic ApproachDrDeepak Pawar71% (7)
- Diagnostic Procedures in Ophthalmology Full ColourDocument488 pagesDiagnostic Procedures in Ophthalmology Full ColourAnquito100% (4)
- Science and Technology GR 5Document187 pagesScience and Technology GR 5Juliet Govatson100% (1)
- Bataan General Hospital and Medical Center: Department of Pathology and LaboratoryDocument2 pagesBataan General Hospital and Medical Center: Department of Pathology and LaboratoryJoan Santiago - GonzagaNo ratings yet
- Complications of Chronic Kidney Disease Current STDocument32 pagesComplications of Chronic Kidney Disease Current STmetaNo ratings yet
- MFD Part 2 - Pediatric Dentistry Exams Questions & AnswersDocument17 pagesMFD Part 2 - Pediatric Dentistry Exams Questions & AnswersDental Knowledge School100% (1)
- DCA Vantage HgbA1C Procedure - LTR19683Document10 pagesDCA Vantage HgbA1C Procedure - LTR19683dianNo ratings yet
- Updated ELSO Pediatric Guidelines 1617997662Document13 pagesUpdated ELSO Pediatric Guidelines 1617997662Useful StuffNo ratings yet
- 05 N501 28766Document23 pages05 N501 28766Rumela Ganguly ChakrabortyNo ratings yet
- Updates On CRPDocument15 pagesUpdates On CRPhabibfmNo ratings yet
- Sellarsetal 2018-ESKDaudit PDFDocument21 pagesSellarsetal 2018-ESKDaudit PDFmetha khairinaNo ratings yet
- Guidelines Extracorporeal Membrane Oxygenation For COVID-19Document11 pagesGuidelines Extracorporeal Membrane Oxygenation For COVID-19bacharelado2010No ratings yet
- CPG in Heart FailureDocument62 pagesCPG in Heart FailureCoffee TeeNo ratings yet
- Percutaneous Circulatory Assist Devices For High-Risk Coronary InterventionDocument16 pagesPercutaneous Circulatory Assist Devices For High-Risk Coronary Interventionamir aliNo ratings yet
- ESC Heart Failure - 2014 - Ponikowski - Heart Failure Preventing Disease and Death WorldwideDocument22 pagesESC Heart Failure - 2014 - Ponikowski - Heart Failure Preventing Disease and Death WorldwideMinh Hai TranNo ratings yet
- Frailty SicaDocument16 pagesFrailty SicaSandra AlRoNo ratings yet
- Establishing A Dedicated Difficult Vascular Access Team in The Emergency DepartmentDocument6 pagesEstablishing A Dedicated Difficult Vascular Access Team in The Emergency DepartmentOnur KNo ratings yet
- Cathet Cardio Intervent - 2019 - Baran - SCAI Clinical Expert Consensus Statement On The Classification of CardiogenicDocument9 pagesCathet Cardio Intervent - 2019 - Baran - SCAI Clinical Expert Consensus Statement On The Classification of CardiogenicvaleriaNo ratings yet
- Chest EgdtDocument6 pagesChest EgdtDhanny AdhityaNo ratings yet
- Dispositivo Assistência VentricularDocument7 pagesDispositivo Assistência Ventricularjuliane gavazziNo ratings yet
- ECS 2024 HandoutDocument5 pagesECS 2024 HandoutucsdlliuNo ratings yet
- Destete y Retiro Ventilación Mecánica. Chest 2001Document23 pagesDestete y Retiro Ventilación Mecánica. Chest 2001alexgonzalezherNo ratings yet
- Rajivgandhi University of Health Sciences, Karnataka: 1. Name of The Candidate and AddressDocument29 pagesRajivgandhi University of Health Sciences, Karnataka: 1. Name of The Candidate and Addresssr.kumariNo ratings yet
- Hemostasis Management of the Pediatric Surgical PatientFrom EverandHemostasis Management of the Pediatric Surgical PatientNina A. GuzzettaNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationAngela Giselle Garcia RuizNo ratings yet
- 2016 GuidelinesDocument6 pages2016 Guidelinesamrit koiralaNo ratings yet
- Journal Reading Anestesi - Alfatun JamiahDocument26 pagesJournal Reading Anestesi - Alfatun JamiahAlfatun JamiahNo ratings yet
- 2001 120 375-396 Neil R. Macintyre: ChestDocument23 pages2001 120 375-396 Neil R. Macintyre: ChestAlberto MHNo ratings yet
- Knowledge of Post Discharge Home Care Management Among Patients With Myocardial InfarctionDocument49 pagesKnowledge of Post Discharge Home Care Management Among Patients With Myocardial InfarctionRumela Ganguly ChakrabortyNo ratings yet
- The DENALI Trial: An Interim Analysis of A Prospective, Multicenter Study of The Denali Retrievable Inferior Vena Cava FilterDocument10 pagesThe DENALI Trial: An Interim Analysis of A Prospective, Multicenter Study of The Denali Retrievable Inferior Vena Cava FilterMostafaNo ratings yet
- Perioperative Management of Heart Transplantation A Clinical ReviewDocument18 pagesPerioperative Management of Heart Transplantation A Clinical ReviewMichael PimentelNo ratings yet
- Ijmsv 14 P 1241Document10 pagesIjmsv 14 P 1241Milan PetrikNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationMarcela ZerilloNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationFandoko ChaniagoNo ratings yet
- CHD Indian GuidelinesDocument15 pagesCHD Indian GuidelinesDhiraj Kr GauravNo ratings yet
- AnotherDocument11 pagesAnotherTudor DumitrascuNo ratings yet
- Cardiorenal Syndromes Advances in Determining Diagnosis, Prognosis and TheraphyDocument29 pagesCardiorenal Syndromes Advances in Determining Diagnosis, Prognosis and TheraphynanreNo ratings yet
- Prepublication ReleaseDocument15 pagesPrepublication ReleaseSangNo ratings yet
- Rickard 156612Document23 pagesRickard 156612NELLY VAZQUEZ FLORESNo ratings yet
- Optimization of Cutting Fluid Using VIKOR MethodDocument9 pagesOptimization of Cutting Fluid Using VIKOR MethodEditor IJTSRDNo ratings yet
- Prolonged Mechanical Ventilation Alters Diaphragmatic Structure and FunctionDocument17 pagesProlonged Mechanical Ventilation Alters Diaphragmatic Structure and FunctionmvmarentesNo ratings yet
- MEDICAL BUZZ VOLUME 7 Final Edition - Compressed PDFDocument28 pagesMEDICAL BUZZ VOLUME 7 Final Edition - Compressed PDFJoelNo ratings yet
- 2020 Canadian Cardiovascular SocietyCanadian Heart Rhythm Society Position Statement On The Management of Ventricular Tachycardia and Fibrillation in Patients With Structural Heart Disease PDFDocument15 pages2020 Canadian Cardiovascular SocietyCanadian Heart Rhythm Society Position Statement On The Management of Ventricular Tachycardia and Fibrillation in Patients With Structural Heart Disease PDFDiego MerchánNo ratings yet
- Collateral Growth in The Peripheral Circulation: A Review: Vascular and Endovascular Surgery July 2004Document24 pagesCollateral Growth in The Peripheral Circulation: A Review: Vascular and Endovascular Surgery July 2004ChavdarNo ratings yet
- Ijnrd 8 125Document13 pagesIjnrd 8 125Muhammad Halil GibranNo ratings yet
- Peripartum Cardiomyopathy A Review ArticleDocument8 pagesPeripartum Cardiomyopathy A Review ArticleAnggi saputriNo ratings yet
- Weaning Infants From Mechanical Ventilation: Clinics in Perinatology September 2012Document21 pagesWeaning Infants From Mechanical Ventilation: Clinics in Perinatology September 2012MALIK MANASRAHNo ratings yet
- Cir 0000000000000909Document28 pagesCir 0000000000000909zhida liuNo ratings yet
- 2017TheSwan GanzCatheterRemainsaCriticallyImpoDocument7 pages2017TheSwan GanzCatheterRemainsaCriticallyImpoCarlos Henrique FerreiraNo ratings yet
- Wide, Complex and Troublesome • LITFL • Cardiovascular curveballDocument7 pagesWide, Complex and Troublesome • LITFL • Cardiovascular curveballsilver silvaNo ratings yet
- Ip Pals2020Document7 pagesIp Pals2020Mario AlexanderNo ratings yet
- Enfermedad Valvular CardiacaDocument10 pagesEnfermedad Valvular CardiacaBrayan HuayraNo ratings yet
- 05 - N031 - 38796 ThesisDocument22 pages05 - N031 - 38796 ThesisdrtareksNo ratings yet
- Chapter FourDocument3 pagesChapter Fourkhadijahkabir0706No ratings yet
- Septic Shock Carcillo PDFDocument14 pagesSeptic Shock Carcillo PDFjesus_berber_2No ratings yet
- Screening and Management of Atrial Fibrillation in Primary Care InglesDocument18 pagesScreening and Management of Atrial Fibrillation in Primary Care InglesIvan VelasquezNo ratings yet
- J Jacc 2022 09 044Document17 pagesJ Jacc 2022 09 044Ivan BitunjacNo ratings yet
- Circulation-2014-Donofrio-01 Cir 0000437597 44550 5dDocument61 pagesCirculation-2014-Donofrio-01 Cir 0000437597 44550 5debriceno2211No ratings yet
- HCM Guidelines Slide Set GL HCMDocument117 pagesHCM Guidelines Slide Set GL HCMjohnweakNo ratings yet
- 1 s2.0 S1071916423003743 MainDocument13 pages1 s2.0 S1071916423003743 MainArunNo ratings yet
- 1 s2.0 S2772930322004367 MainDocument15 pages1 s2.0 S2772930322004367 MainVimal NishadNo ratings yet
- BPH and Its Scope in HomeopathyDocument3 pagesBPH and Its Scope in HomeopathyEditor IJTSRDNo ratings yet
- Talk by DR - Judy JeyakumarDocument5 pagesTalk by DR - Judy JeyakumarKalmunai Mental Health AssociationNo ratings yet
- Multiple Skin Ulcers From Malignant SyphilisDocument1 pageMultiple Skin Ulcers From Malignant SyphilisMuhammad AkrimNo ratings yet
- ABG ExamplesDocument31 pagesABG ExamplesKEROLOS MAHROUSNo ratings yet
- Presepsin 6Document189 pagesPresepsin 6donkeyendutNo ratings yet
- Preguntas Sobre Varios TemasDocument4 pagesPreguntas Sobre Varios TemasGerardo Davalos GuzmanNo ratings yet
- Medica CatalogueDocument61 pagesMedica CatalogueMarysia BurekNo ratings yet
- Mod 9 CC of Proteins Part 1Document9 pagesMod 9 CC of Proteins Part 1Benson PaglinawanNo ratings yet
- BodyDocument29 pagesBodyYa RabNo ratings yet
- Role of Nutraceuticals in Health and Disease PreventionDocument7 pagesRole of Nutraceuticals in Health and Disease PreventionIJRASETPublicationsNo ratings yet
- Mental Illness Assessment Data Via KahootDocument107 pagesMental Illness Assessment Data Via Kahootapi-384598186No ratings yet
- Aborsion: Spontaneou SDocument214 pagesAborsion: Spontaneou Sorkaido berisha (Addisu)No ratings yet
- Difficult Airway Management During Anesthesia A Review of The Incidence and SolutionsDocument6 pagesDifficult Airway Management During Anesthesia A Review of The Incidence and SolutionsSudar Pecinta ParawaliNo ratings yet
- Jurnal Intadialitic ExerciseDocument9 pagesJurnal Intadialitic Exercisedwi nurdianingtyasNo ratings yet
- Decipher Final Year Updates-1Document10 pagesDecipher Final Year Updates-1Dr NnuNo ratings yet
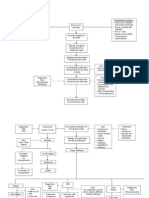
- Pathophysiology of ALL DiagramDocument3 pagesPathophysiology of ALL DiagramErika DellosaNo ratings yet
- Mututho Leah NjeriDocument138 pagesMututho Leah NjeriNandhini ShreeNo ratings yet
- Bullous DiseaseDocument42 pagesBullous DiseaseErika KusumawatiNo ratings yet
- Embryo Biopsy: M. Boada and A. Veiga M. Boada and A. VeigaDocument32 pagesEmbryo Biopsy: M. Boada and A. Veiga M. Boada and A. VeigaTrang Nguyễn NhưNo ratings yet