You might also like
- 10 1038@sj BDJ 2016 855Document8 pages10 1038@sj BDJ 2016 855Sofia PereiraNo ratings yet
- Banerjee 2017Document8 pagesBanerjee 2017FFDFNo ratings yet
- Ray 2017Document10 pagesRay 2017Chris MartinNo ratings yet
- Dental Practicality IndexDocument4 pagesDental Practicality Indexdorasani99No ratings yet
- Interprofessionalism Education in DentistryDocument6 pagesInterprofessionalism Education in DentistryRuxi Moraru BottrillNo ratings yet
- A Guide to Managing Tooth WearDocument9 pagesA Guide to Managing Tooth WearNajeeb UllahNo ratings yet
- The Process of Care: EditorialDocument1 pageThe Process of Care: EditorialGarry B GunawanNo ratings yet
- Tooth Bleaching Questions AnsweredDocument12 pagesTooth Bleaching Questions AnsweredleiddyNo ratings yet
- Mehta, 2018Document9 pagesMehta, 2018GOOSI666No ratings yet
- Failure of Eruption Central IncisorDocument7 pagesFailure of Eruption Central Incisor9fxhktdqy8No ratings yet
- Digital Implant Planning and Guided Implant Surgery Workflow and ReliabilityDocument8 pagesDigital Implant Planning and Guided Implant Surgery Workflow and ReliabilityDenisa CorneaNo ratings yet
- New Perio ClassificationDocument8 pagesNew Perio ClassificationLauraNo ratings yet
- Atraumatic Restorative Treatment and Minimal Intervention DentistryDocument7 pagesAtraumatic Restorative Treatment and Minimal Intervention DentistryKalpanaNo ratings yet
- Guidelines For The Selection, Use, and Maintenance of LED Light-Curing Units - Part IIDocument4 pagesGuidelines For The Selection, Use, and Maintenance of LED Light-Curing Units - Part IIpoojaNo ratings yet
- Rubber Dam May Increase The Survival Time of Dental RestorationsDocument2 pagesRubber Dam May Increase The Survival Time of Dental Restorationsjhon valdiviezoNo ratings yet
- Articulo Hospitalaria 7 PDFDocument7 pagesArticulo Hospitalaria 7 PDFJulia Rodríguez VegaNo ratings yet
- ESTÉTICA. Magne Histo Anatomic 3D Printing of Dental StructuresDocument6 pagesESTÉTICA. Magne Histo Anatomic 3D Printing of Dental StructuresKenigal14No ratings yet
- B DJ Team 2018199654297Document3 pagesB DJ Team 2018199654297abhinavNo ratings yet
- Jurnal DentistDocument8 pagesJurnal DentistAnugrah AztriNo ratings yet
- Dietschi 2016 PDFDocument7 pagesDietschi 2016 PDFPanchyRojasNo ratings yet
- The Oral Health of Individuals With Dental Phobia: A Multivariate Analysis of The Adult Dental Health Survey, 2009Document10 pagesThe Oral Health of Individuals With Dental Phobia: A Multivariate Analysis of The Adult Dental Health Survey, 2009Sung Soon ChangNo ratings yet
- 2017 Systmatic ReviewDocument10 pages2017 Systmatic ReviewSara MoustafaNo ratings yet
- SJ BDJ 2016 914Document5 pagesSJ BDJ 2016 914Benítez García Leonardo Axel. 3IM9No ratings yet
- Paper Bulk-Fill Resin-Based Composite Restorative Materials A ReviewDocument8 pagesPaper Bulk-Fill Resin-Based Composite Restorative Materials A ReviewkaidehxcNo ratings yet
- Meeting IFSTTAR VTTI TRB 2017 - Living Lab in Bordeaux V3Document14 pagesMeeting IFSTTAR VTTI TRB 2017 - Living Lab in Bordeaux V3Jaja OcochatNo ratings yet
- Gingival Overgrowth: Part 1: Aetiology and Clinical DiagnosisDocument7 pagesGingival Overgrowth: Part 1: Aetiology and Clinical Diagnosiswafiqah izzatul auliahNo ratings yet
- Costs: Input Costs, Cost of Other Resources, Economies of Scale and ScopeDocument5 pagesCosts: Input Costs, Cost of Other Resources, Economies of Scale and ScopeRaunaq DashNo ratings yet
- The Orthodontic-Oral Surgery Interface.Document6 pagesThe Orthodontic-Oral Surgery Interface.jing.zhao222No ratings yet
- Al-Harbi - 2018 - A Guide To Minimally Invasive Crown Lengthening and Tooth Preparation For Rehabilitating Pink and White AeDocument7 pagesAl-Harbi - 2018 - A Guide To Minimally Invasive Crown Lengthening and Tooth Preparation For Rehabilitating Pink and White AefishribbonNo ratings yet
- PDCL Model: A 4-Step Process for Problem-SolvingDocument3 pagesPDCL Model: A 4-Step Process for Problem-SolvingFraz RazaNo ratings yet
- Course Outline - Finance and Accounting - CS CourseDocument11 pagesCourse Outline - Finance and Accounting - CS Courseab3754795No ratings yet
- Dialysis Nurse Responsibilities and DutiesDocument22 pagesDialysis Nurse Responsibilities and DutiesWyn Agustin0% (1)
- 219-ACW-49-Marketing ManagementDocument24 pages219-ACW-49-Marketing ManagementKISHANINo ratings yet
- Jurnal Nilai Kritis LabDocument16 pagesJurnal Nilai Kritis LabAmalia EnggarNo ratings yet
- Selection Structures and Looping in CDocument25 pagesSelection Structures and Looping in CSarahmei MeiNo ratings yet
- How To Use The Scores Achieved by University Graduates Under CEPAS As Reference in Hiring The Right EmployeesDocument38 pagesHow To Use The Scores Achieved by University Graduates Under CEPAS As Reference in Hiring The Right EmployeesmxiixmNo ratings yet
- ISO/IEC 15504-Evolution To An International Standard: Software Process Improvement and Practice January 2003Document21 pagesISO/IEC 15504-Evolution To An International Standard: Software Process Improvement and Practice January 2003wendyNo ratings yet
- Nature Comment - Triangulation Instead of ReplicationDocument3 pagesNature Comment - Triangulation Instead of ReplicationfacefaceNo ratings yet
- WITS - EAP Client Guide EpubublicationDocument102 pagesWITS - EAP Client Guide EpubublicationRon WatermeyerNo ratings yet
- Self-Adhesive Resin Cements: A Literature ReviewDocument8 pagesSelf-Adhesive Resin Cements: A Literature ReviewOke Soe MoeNo ratings yet
- Assessment: Understanding TransformativeDocument12 pagesAssessment: Understanding Transformativetherond7No ratings yet
- News in Focus: Giant Health Studies Try To Tap Wearable ElectronicsDocument2 pagesNews in Focus: Giant Health Studies Try To Tap Wearable ElectronicsLuiz Folha FlaskNo ratings yet
- A biologist talks to a physicistDocument4 pagesA biologist talks to a physicistBzar Blue ClnNo ratings yet
- Comment: Clean Up Energy InnovationDocument3 pagesComment: Clean Up Energy InnovationCesar NietoNo ratings yet
- Inter-Proximal Enamel Reduction in Contemporary OrthodonticsDocument7 pagesInter-Proximal Enamel Reduction in Contemporary OrthodonticsAly OsmanNo ratings yet
- Digital Marketing, Analytics and Storytelling With Data Individual Portfolio - Storytelling With DataDocument13 pagesDigital Marketing, Analytics and Storytelling With Data Individual Portfolio - Storytelling With DatarajeshNo ratings yet
- Clinical Audit ReportDocument6 pagesClinical Audit Reportjhonron100% (1)
- Healthcare Marketing MixDocument4 pagesHealthcare Marketing Mixjain8687No ratings yet
- The Academic Experience of Students in English Universities: Higher Education Policy Institute September 2007Document75 pagesThe Academic Experience of Students in English Universities: Higher Education Policy Institute September 2007Liu ZiheNo ratings yet
- New Pedagogical Possi Bilities in post-COVID Higher Ed Ucation and Impact On Student EngagementDocument24 pagesNew Pedagogical Possi Bilities in post-COVID Higher Ed Ucation and Impact On Student EngagementAmit DeyNo ratings yet
- No Confidence That Success Rates of Self-Drilling and Self-Tapping Insertion Techniques of Orthodontic Mini-Implants Are SimilarDocument3 pagesNo Confidence That Success Rates of Self-Drilling and Self-Tapping Insertion Techniques of Orthodontic Mini-Implants Are SimilarAndres CoboNo ratings yet
- B.tech Project Stage-II Presentation - MidsemDocument26 pagesB.tech Project Stage-II Presentation - Midsemkaalin bhaiyaNo ratings yet
- National Footprint and Biocapacity Accounts 2005: The Underlying Calculation MethodDocument33 pagesNational Footprint and Biocapacity Accounts 2005: The Underlying Calculation MethodJames McQuaidNo ratings yet
- Tufr!: DepartmentDocument10 pagesTufr!: DepartmentLevi CalubagNo ratings yet
- Infection Control Measures in Dental Clinics in Kingdom of Saudi ArabiaDocument4 pagesInfection Control Measures in Dental Clinics in Kingdom of Saudi Arabiaاحمد القحطانيNo ratings yet
- Cultural, Political, Legal, and Economical Analysis of India For Carbon Engineering CompanyDocument19 pagesCultural, Political, Legal, and Economical Analysis of India For Carbon Engineering CompanySandesh Sunil BoraNo ratings yet
- QA T VN HRD Local - Induction - Guide 0Document21 pagesQA T VN HRD Local - Induction - Guide 0Khosbayar PurevsurenNo ratings yet
- Antibiotics - Small Molecule - Not - B - Developed d41586-020-02884-3Document3 pagesAntibiotics - Small Molecule - Not - B - Developed d41586-020-02884-3SHINDY ARIESTA DEWIADJIENo ratings yet
- The Goals of Customer Relationship ManagementDocument13 pagesThe Goals of Customer Relationship Managementadei667062No ratings yet
- PolymerizationDocument5 pagesPolymerizationAlex KwokNo ratings yet
- Merin ClassificationDocument2 pagesMerin ClassificationPatphajong Limteerakul100% (11)
- CH 9Document13 pagesCH 9dadingafgiNo ratings yet
- Dental Bridge Failure Treatment OptionsDocument62 pagesDental Bridge Failure Treatment OptionsMahad Mostapha IbrahimNo ratings yet
- BDS Examiners Panel List 2013Document391 pagesBDS Examiners Panel List 2013Suman KashyapNo ratings yet
- 48763finalfile FIK PF1AB SL PNKM1Document5 pages48763finalfile FIK PF1AB SL PNKM1Dr. Shaili MehtaNo ratings yet
- ICX Instructiuni de UtilizareDocument16 pagesICX Instructiuni de UtilizareanaNo ratings yet
- Roane, James B. - The Balanced Force Concept, JOE, 11, 5, May 1985Document9 pagesRoane, James B. - The Balanced Force Concept, JOE, 11, 5, May 1985Nataly ZuñigaNo ratings yet
- SybronEndo PDFDocument8 pagesSybronEndo PDFAnn M.No ratings yet
- Efektivitas Pasta Gigi Herbal Dan Non-Herbal Terhadap Penurunan Plak Gigi Anak Usia 12-14 TahunDocument7 pagesEfektivitas Pasta Gigi Herbal Dan Non-Herbal Terhadap Penurunan Plak Gigi Anak Usia 12-14 Tahunfadhilah nurNo ratings yet
- Medical Supplies and Equipment Names in EnglishDocument8 pagesMedical Supplies and Equipment Names in EnglishPatricia PierreNo ratings yet
- Dental Hygiene Thesis TopicsDocument9 pagesDental Hygiene Thesis Topicsoabfziiig100% (2)
- Letter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Document10 pagesLetter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Cristina EneNo ratings yet
- Development of FaceDocument17 pagesDevelopment of FaceDr Billa AishwaryaNo ratings yet
- Orthognathic Surgery: This Chapter AddressesDocument40 pagesOrthognathic Surgery: This Chapter AddressesJ.A.C.No ratings yet
- Print Kuesioner WhostepwiseDocument2 pagesPrint Kuesioner WhostepwiseRinaldi InalNo ratings yet
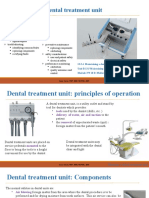
- CM Dental Treatment Unit PPDocument13 pagesCM Dental Treatment Unit PPSofwan SukmalanaNo ratings yet
- Pharmaceutical Sciences: Diagnostic Accuracy of Conventional and Digital Radiography in Periapical Bone LesionsDocument4 pagesPharmaceutical Sciences: Diagnostic Accuracy of Conventional and Digital Radiography in Periapical Bone LesionsiajpsNo ratings yet
- Ear Nose Throat Exam Features GuideDocument4 pagesEar Nose Throat Exam Features GuideMawj MandwieNo ratings yet
- 2020 Naldeman Premature Loss of Primary Anterior TeethDocument26 pages2020 Naldeman Premature Loss of Primary Anterior TeethDiego Andres Hincapie HerreraNo ratings yet
- Shade Guides Used in The Dental PracticeDocument6 pagesShade Guides Used in The Dental PracticeNurul Khadijah HannbNo ratings yet
- 2-Eruption of TeethDocument9 pages2-Eruption of TeethAhmed AbdNo ratings yet
- Periodontitis Consensus Report of Workgroup 2 of The 2017 14Document9 pagesPeriodontitis Consensus Report of Workgroup 2 of The 2017 14Naye AntonioNo ratings yet
- An Investigation Into The Effect of A Resin Infiltrant On The Micromechanical Properties of Hypomineralised EnamelDocument13 pagesAn Investigation Into The Effect of A Resin Infiltrant On The Micromechanical Properties of Hypomineralised Enamelzubair ahmedNo ratings yet
- Posterior Scissor Bite and Lateral Open Bite With Missing Lower First Molar and Second PremolarDocument9 pagesPosterior Scissor Bite and Lateral Open Bite With Missing Lower First Molar and Second PremolarJohn PulgarinNo ratings yet
- RCT Procedure ExplainedDocument8 pagesRCT Procedure ExplainedStanislavNemtanuNo ratings yet
- Social Sciences in DentistryDocument39 pagesSocial Sciences in DentistryPrabhu AypaNo ratings yet
- Productividad y Calidad Metodológica de Artículos Clínicos en Cirugía Oral y Maxilofacial en Chile. Período 2001-2012Document7 pagesProductividad y Calidad Metodológica de Artículos Clínicos en Cirugía Oral y Maxilofacial en Chile. Período 2001-2012DANIELA RINCÓN BELLONo ratings yet
- Physical and Chemical Injuries of The Oral CavityDocument124 pagesPhysical and Chemical Injuries of The Oral CavityAman KankariaNo ratings yet
- AntibiotikDocument10 pagesAntibiotikGeubrina FitrianandaNo ratings yet