You might also like
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka. Performa For Registration of Subject For DissertationDocument21 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka. Performa For Registration of Subject For DissertationSri HariNo ratings yet
- Outlook Group Written AssignmentDocument34 pagesOutlook Group Written Assignmentashish9dubey-1680% (10)
- 1 s2.0 S2093791120302687 MainDocument8 pages1 s2.0 S2093791120302687 MainMasyfuk ZainNo ratings yet
- The Greenock HangingsDocument5 pagesThe Greenock HangingsInverclyde Community Development Trust100% (2)
- Review of Ultrasonic Irrigation in Endodontics Increasing Action of Irrigating SolutionsDocument10 pagesReview of Ultrasonic Irrigation in Endodontics Increasing Action of Irrigating SolutionsayoubNo ratings yet
- Aircraft Strategy and Operations of The Soviet Air Force 1986 CompressDocument280 pagesAircraft Strategy and Operations of The Soviet Air Force 1986 CompressMatthew Guest100% (1)
- LESSON EXEMPLAR in ENGLISHDocument4 pagesLESSON EXEMPLAR in ENGLISHFelices Christy C. CorderoNo ratings yet
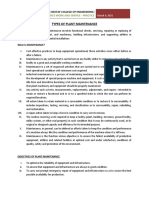
- Types of Plant MaintenanceDocument7 pagesTypes of Plant MaintenanceTHEOPHILUS ATO FLETCHERNo ratings yet
- 585 600 HellemanDocument17 pages585 600 HellemanBudi Darmawan DiswanNo ratings yet
- Audiologic Characteristics of Hearing and Tinnitus in Occupational Noise-Induced Hearing Loss PDFDocument5 pagesAudiologic Characteristics of Hearing and Tinnitus in Occupational Noise-Induced Hearing Loss PDFKaty Marlen GongoraNo ratings yet
- Ultrasonic Scaling: Associated Risks.: Review ArticleDocument5 pagesUltrasonic Scaling: Associated Risks.: Review Articlevivi alfiyani noorNo ratings yet
- Association Between Shift Work and Hearing Loss The Dongfeng-TongjiDocument7 pagesAssociation Between Shift Work and Hearing Loss The Dongfeng-TongjiKaty Marlen GongoraNo ratings yet
- SarantisDocument1 pageSarantisMixindo OfficialNo ratings yet
- In Uence of The Major Connector in A Maxillary Denture On Phonetic FunctionDocument10 pagesIn Uence of The Major Connector in A Maxillary Denture On Phonetic FunctionZachary DuongNo ratings yet
- Cochlear Dysfunction With Acoustic Trauma in Fire Shooting TrainingDocument5 pagesCochlear Dysfunction With Acoustic Trauma in Fire Shooting TrainingDesywinNo ratings yet
- InstrumentationDocument12 pagesInstrumentationMaiush JbNo ratings yet
- Vacuum Aerosol 6Document7 pagesVacuum Aerosol 6khamilatusyNo ratings yet
- 63D17 391 Nyi Mas Siti PurwaningsihDocument4 pages63D17 391 Nyi Mas Siti PurwaningsihAstridNo ratings yet
- Anthropometry of External Auditory Canal by Non-Contactable MeasurementDocument6 pagesAnthropometry of External Auditory Canal by Non-Contactable MeasurementMusdah MMNo ratings yet
- Extrusion of Debris From Primary Molar Root Canals Following Instrumentation With Traditional and New File SystemsDocument6 pagesExtrusion of Debris From Primary Molar Root Canals Following Instrumentation With Traditional and New File Systemssyed fazluddinNo ratings yet
- English AnIntroductiontoSoundSpectrumLevel-SpectrumAnalysisDocument5 pagesEnglish AnIntroductiontoSoundSpectrumLevel-SpectrumAnalysisDharmendra ChoudharyNo ratings yet
- Brainsci 10 00732Document11 pagesBrainsci 10 00732Nur Rahmi SeptiantyNo ratings yet
- Listening With Our Teeth! The Soundbite Hearing Aid: A New Technology For Single-Sided DeafnessDocument2 pagesListening With Our Teeth! The Soundbite Hearing Aid: A New Technology For Single-Sided Deafnessはじめ ましてNo ratings yet
- Progressive Asymmetry in Occupational Noise-Induced Hearing Loss A Large Population-Based Cohort Study With A 15-Year Follow-Up PDFDocument6 pagesProgressive Asymmetry in Occupational Noise-Induced Hearing Loss A Large Population-Based Cohort Study With A 15-Year Follow-Up PDFKaty Marlen GongoraNo ratings yet
- A Wheeze Recognition Algorithm For Practical Implementation in ChildrenDocument12 pagesA Wheeze Recognition Algorithm For Practical Implementation in ChildrenSophia RoseNo ratings yet
- Brushing Force of Manual and Sonic Toothbrushes Affects Dental Hard Tissue AbrasionDocument25 pagesBrushing Force of Manual and Sonic Toothbrushes Affects Dental Hard Tissue AbrasionLeonardo AlcotaNo ratings yet
- New Possibilities On The Application of Violet Light in Dentistry Combining Aesthetics and Microbiological Control Report of Two Clinical CasesDocument10 pagesNew Possibilities On The Application of Violet Light in Dentistry Combining Aesthetics and Microbiological Control Report of Two Clinical CasesAthenaeum Scientific PublishersNo ratings yet
- Applying Kurtosis As An Indirect Metric of Noise Temporal Structure in The Assessment of Hearing Loss Associated With Occupational Complex Noise Exposure PDFDocument15 pagesApplying Kurtosis As An Indirect Metric of Noise Temporal Structure in The Assessment of Hearing Loss Associated With Occupational Complex Noise Exposure PDFKaty Marlen GongoraNo ratings yet
- Study of The Effect of Mobile Phones On HearingDocument5 pagesStudy of The Effect of Mobile Phones On HearingPranay DasNo ratings yet
- Effects of Preprocedural Mouth Rinse On Microbial.12Document7 pagesEffects of Preprocedural Mouth Rinse On Microbial.12samanvi badriNo ratings yet
- Occupational Noise Exposure and Risk For Noise-Induced Hearing Loss Due To Temporal Bone DrillingDocument7 pagesOccupational Noise Exposure and Risk For Noise-Induced Hearing Loss Due To Temporal Bone DrillingAnanda Chaerunnisa PattisahusiwaNo ratings yet
- Auditory System Rehabilitation Available TechnologDocument6 pagesAuditory System Rehabilitation Available TechnologCalugareanu MadalinaNo ratings yet
- A Clinical Audit On The Compliance of Ultrasound Users To The Standard Operating Procedure of Ultrasonography in A Private Radiologic AcademyDocument9 pagesA Clinical Audit On The Compliance of Ultrasound Users To The Standard Operating Procedure of Ultrasonography in A Private Radiologic AcademyEsther YekoNo ratings yet
- Noise Reduction in Hospital With Help of Sound Absorbing MaterialsDocument7 pagesNoise Reduction in Hospital With Help of Sound Absorbing MaterialsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Article WJPR 14779097973Document8 pagesArticle WJPR 14779097973Lakshmi PriyaNo ratings yet
- Obstacle Detection Using Utltasonic Sensor: November 2020Document39 pagesObstacle Detection Using Utltasonic Sensor: November 2020vishwasNo ratings yet
- Make A Report Writing - BellaDocument3 pagesMake A Report Writing - BellaBella Naziel IqmaliaNo ratings yet
- Jurnal Kesehatan Lingkungan IndonesiaDocument6 pagesJurnal Kesehatan Lingkungan IndonesiaNuriemayaniNo ratings yet
- 2020 Cai - Efficacy of Aromatherapy On Dental Anxiety A Systematic Review of Randomised andDocument19 pages2020 Cai - Efficacy of Aromatherapy On Dental Anxiety A Systematic Review of Randomised andfabian.balazs.93No ratings yet
- Middle Ear ImplantsDocument5 pagesMiddle Ear ImplantsPrakashNo ratings yet
- Ozone Hand Out WD 1Document1 pageOzone Hand Out WD 1api-522938055No ratings yet
- A Comparative Evaluation of An Ultrasonic and A Manual Toothbrush On The Oral Hygiene Status and Stain Removing EfficacyDocument3 pagesA Comparative Evaluation of An Ultrasonic and A Manual Toothbrush On The Oral Hygiene Status and Stain Removing EfficacyMayurNo ratings yet
- tmp41D3 TMPDocument3 pagestmp41D3 TMPFrontiersNo ratings yet
- Occupational NoiseDocument17 pagesOccupational NoiseHAVIRRNA A/P ANBALAGAN HaviNo ratings yet
- JOEH 22 0227 Proof HiDocument25 pagesJOEH 22 0227 Proof HiFioriAmeliaHathawayNo ratings yet
- Blockmate: A Practical Guide for Ultrasound Guided Regional AnaesthesiaFrom EverandBlockmate: A Practical Guide for Ultrasound Guided Regional AnaesthesiaArunangshu ChakrabortyNo ratings yet
- Hubungan Antara Lama Kerja Dengan Terjadinya Noise Induced Hearing Loss (NIHL) Pada Masinis DAOP-IV SemarangDocument10 pagesHubungan Antara Lama Kerja Dengan Terjadinya Noise Induced Hearing Loss (NIHL) Pada Masinis DAOP-IV Semaranghanindyo rizkyNo ratings yet
- Use of Otoacoustic Emissions (OAE) To Detect Sub-Clinical Inner Ear Damage in Divers of The Indian NavyDocument5 pagesUse of Otoacoustic Emissions (OAE) To Detect Sub-Clinical Inner Ear Damage in Divers of The Indian Navyarum manisNo ratings yet
- Hearing Research: Arwa Kurabi, Elizabeth M. Keithley, Gary D. Housley, Allen F. Ryan, Ann C.-Y. WongDocument9 pagesHearing Research: Arwa Kurabi, Elizabeth M. Keithley, Gary D. Housley, Allen F. Ryan, Ann C.-Y. WongflorensiaNo ratings yet
- Printhandler AshxDocument17 pagesPrinthandler AshxALINA LAMICHHANENo ratings yet
- Dampak Penggunaan HeadseatDocument7 pagesDampak Penggunaan HeadseatLucya WulandariNo ratings yet
- QNDE2009 PerioProbe PDFDocument9 pagesQNDE2009 PerioProbe PDFPame FloresNo ratings yet
- Acoustic Analysis of Speech Under StressDocument16 pagesAcoustic Analysis of Speech Under Stresshhakim32No ratings yet
- Ozone: The Revolution in Dentistry: January 2004Document5 pagesOzone: The Revolution in Dentistry: January 2004José Antonio López Maldonado0% (1)
- Hearing Loss: Mechanisms, Prevention and Cure: Huawei Li Renjie Chai EditorsDocument182 pagesHearing Loss: Mechanisms, Prevention and Cure: Huawei Li Renjie Chai EditorsFernando Cárdenas WongNo ratings yet
- Assessment of Exposure To Voices and Noise Via Earphones in JAPANDocument7 pagesAssessment of Exposure To Voices and Noise Via Earphones in JAPANYAINo ratings yet
- Relationship of Noise and The Use of Ear Plugs WitDocument8 pagesRelationship of Noise and The Use of Ear Plugs WitIlmiMardatillahNo ratings yet
- Printhandler AshxDocument17 pagesPrinthandler AshxALINA LAMICHHANENo ratings yet
- FULLTEXT01Document100 pagesFULLTEXT01ewiodjewNo ratings yet
- IEEE Proof Web VersionDocument26 pagesIEEE Proof Web VersionmancstNo ratings yet
- Efficacy of Aromatherapy On Dental AnxietyDocument39 pagesEfficacy of Aromatherapy On Dental AnxietyDafne MendozaNo ratings yet
- AAF en AdultosDocument8 pagesAAF en AdultosJennifer ArévaloNo ratings yet
- Vacuum Aerosol 5Document6 pagesVacuum Aerosol 5khamilatusyNo ratings yet
- Levels of Noise in A Public Hospital LaundryDocument8 pagesLevels of Noise in A Public Hospital LaundryNur Ainatun NadrahNo ratings yet
- Angle Orthod 2014 84 5 839-45Document7 pagesAngle Orthod 2014 84 5 839-45brookortontiaNo ratings yet
- Screenshot 2024-02-14 at 11.35.01 PMDocument32 pagesScreenshot 2024-02-14 at 11.35.01 PMemaantejani10No ratings yet
- Present Tenses RevisionDocument1 pagePresent Tenses RevisionJasmina LatinovicNo ratings yet
- An Introduction To Uhde Oil & Gas: Thyssenkrupp Uhde - Engineering With IdeasDocument40 pagesAn Introduction To Uhde Oil & Gas: Thyssenkrupp Uhde - Engineering With IdeasHany FathyNo ratings yet
- Machinery's Handbook 27th Edition: Tooling and ToolmakingDocument3 pagesMachinery's Handbook 27th Edition: Tooling and ToolmakingOmkar KshirsagarNo ratings yet
- Holy Is The Lord-GDocument1 pageHoly Is The Lord-Gmolina.t4613No ratings yet
- ACT 1, SCENE 7: Macbeth's CastleDocument3 pagesACT 1, SCENE 7: Macbeth's CastleViranthi CoorayNo ratings yet
- IFAS - Presentation - S2Document21 pagesIFAS - Presentation - S2Abinash BiswalNo ratings yet
- Deutscher National-KatechismusDocument3 pagesDeutscher National-KatechismusitsgabbywanNo ratings yet
- Job Offer Electrical EngineerDocument3 pagesJob Offer Electrical EngineerAbner ZaldivarNo ratings yet
- Walt Disney BiographyDocument8 pagesWalt Disney BiographyIsaacRodríguezNo ratings yet
- Bacc Form 02Document2 pagesBacc Form 02Jeanpaul PorrasNo ratings yet
- International Human Resource ManagementDocument24 pagesInternational Human Resource ManagementBharath ChootyNo ratings yet
- Print Book FinalDocument25 pagesPrint Book FinalKhurram AliNo ratings yet
- Information Processing 2Document6 pagesInformation Processing 2Owen RamiscalNo ratings yet
- Human Rights RapDocument4 pagesHuman Rights Rapapi-264123803No ratings yet
- Surfactants and Emulsifying Agents: January 2009Document7 pagesSurfactants and Emulsifying Agents: January 2009Jocc Dee LightNo ratings yet
- Normalization ExercisesDocument2 pagesNormalization ExercisesAnh DiệuNo ratings yet
- Drugs: Samkox Productions 0774852021Document2 pagesDrugs: Samkox Productions 0774852021MichaelNo ratings yet
- ASA 105: Coastal Cruising Curriculum: Prerequisites: NoneDocument3 pagesASA 105: Coastal Cruising Curriculum: Prerequisites: NoneWengerNo ratings yet
- CV EnglishDocument1 pageCV EnglishVijay AgrahariNo ratings yet
- Wimod Ic iC880A: DatasheetDocument26 pagesWimod Ic iC880A: DatasheetJulian CamiloNo ratings yet
- PPP Projects at A Glance. Madhya PradeshDocument7 pagesPPP Projects at A Glance. Madhya PradeshPPPnewsNo ratings yet
- Decanal Working Group On Indigenous Teaching and Learning ReportDocument73 pagesDecanal Working Group On Indigenous Teaching and Learning ReportIlya BanaresNo ratings yet
- Loan Modifications - Workout Plans and ModificationDocument43 pagesLoan Modifications - Workout Plans and ModificationSudershan ThaibaNo ratings yet
- Potter's House Christian FellowshipDocument12 pagesPotter's House Christian Fellowshipwattssteve21No ratings yet