You might also like
- Cranial Nerves 1Document89 pagesCranial Nerves 1Amare GetnetNo ratings yet
- 9d Orbit-Blood Vessels & Nerves-Dr-GosaiDocument8 pages9d Orbit-Blood Vessels & Nerves-Dr-GosaiDr.B.B.GosaiNo ratings yet
- Head, Cranial Nerves Part 1Document53 pagesHead, Cranial Nerves Part 1raegan.farbodNo ratings yet
- 4.development of CNSDocument90 pages4.development of CNSdenekeNo ratings yet
- 12 - Nervous System DevelopmentDocument76 pages12 - Nervous System DevelopmentIRENE SEBASTIANNo ratings yet
- Central Nervous System: Brain & Spinal CordDocument36 pagesCentral Nervous System: Brain & Spinal Cordthe_jokosNo ratings yet
- The OrbitDocument115 pagesThe OrbitPhilip McNelson100% (1)
- The Midbrain and Important ConnectionsDocument118 pagesThe Midbrain and Important ConnectionsBaguma MichaelNo ratings yet
- Olfactory NerveDocument65 pagesOlfactory NerveBahadur BalochNo ratings yet
- Anatomy of Brain Stem: ANA 313 Neuro-Anatomy LectureDocument41 pagesAnatomy of Brain Stem: ANA 313 Neuro-Anatomy LectureSaidu TanimuNo ratings yet
- Seminar Cranial NervesDocument97 pagesSeminar Cranial NervesferozeferoNo ratings yet
- HNF 20 Cranial Nerves III, IV, VIDocument23 pagesHNF 20 Cranial Nerves III, IV, VIthugsena39No ratings yet
- Feb 2015 - BJO - EMBRIOLOGY OF THE CNSDocument39 pagesFeb 2015 - BJO - EMBRIOLOGY OF THE CNSihwan Ukhrawi AlyNo ratings yet
- Pyramidal SystemDocument52 pagesPyramidal SystemKowsalya SelvarajNo ratings yet
- The Spinal CordDocument59 pagesThe Spinal CordbegeerizikNo ratings yet
- Cranial Nerves Part ADocument60 pagesCranial Nerves Part Asana kayaniNo ratings yet
- Cranial Nerve Part 2 (V, VII) : By: Fajri Mohammed (MD)Document51 pagesCranial Nerve Part 2 (V, VII) : By: Fajri Mohammed (MD)abo kooNo ratings yet
- Brainstem - Pons MidbrainDocument24 pagesBrainstem - Pons MidbrainjabirNo ratings yet
- Nervous SystemDocument98 pagesNervous Systemsolomonchinagorom152No ratings yet
- BrainDocument33 pagesBrainGeoffreyNo ratings yet
- Medulla Oblongata Anatomy: Abbas A. A. Shawka Medical Student 2nd GradeDocument40 pagesMedulla Oblongata Anatomy: Abbas A. A. Shawka Medical Student 2nd Gradetuhin100% (1)
- Facial Nerve: BY Alvi Fatima Mds 1 Year Dept of Prevantive and Pediatric DentistryDocument69 pagesFacial Nerve: BY Alvi Fatima Mds 1 Year Dept of Prevantive and Pediatric DentistryHarees ShabirNo ratings yet
- Embryology of Cns and AnomaliesDocument111 pagesEmbryology of Cns and AnomaliesBaguma MichaelNo ratings yet
- Midbrain - 2-18-07-2020Document26 pagesMidbrain - 2-18-07-2020Vinod SharmaNo ratings yet
- CEREBELUMDocument48 pagesCEREBELUMMarian GeorgeNo ratings yet
- Trigeminal Nerve: Nikita Sebastian Mds I Department of Conservative Dentistry and Endodontics JSSDCHDocument63 pagesTrigeminal Nerve: Nikita Sebastian Mds I Department of Conservative Dentistry and Endodontics JSSDCHNikita SebastianNo ratings yet
- Brainstem (Yuni)Document34 pagesBrainstem (Yuni)Ayi Abdul Basith100% (2)
- Nervous System IIIDocument24 pagesNervous System IIIأمال داودNo ratings yet
- Anatomy of BrainstemDocument66 pagesAnatomy of BrainstemFitria OctavianiNo ratings yet
- Oculomotor Nerve: DR / Hytham NafadyDocument52 pagesOculomotor Nerve: DR / Hytham NafadyGetLyricsNo ratings yet
- Cranial Nerves 2021Document105 pagesCranial Nerves 2021May KimNo ratings yet
- Brainstem - Activity SheetDocument12 pagesBrainstem - Activity SheetlindaNo ratings yet
- Nerves of The OrbitDocument6 pagesNerves of The OrbitAshifa SahiraNo ratings yet
- Worksheet 2016Document6 pagesWorksheet 2016Laura TapiaNo ratings yet
- Termin SarafDocument26 pagesTermin SarafSyifa KaniaNo ratings yet
- Oculomotor Nerve 3Document30 pagesOculomotor Nerve 3Sanreet RandhawaNo ratings yet
- Phpapp02Document52 pagesPhpapp02tauseefNo ratings yet
- Brain Stem: - Located BTWN The Cerebrum and The SCDocument41 pagesBrain Stem: - Located BTWN The Cerebrum and The SCnkuligowskiNo ratings yet
- Neuro 3 Brainstem and Spinal Cord BriefDocument68 pagesNeuro 3 Brainstem and Spinal Cord BriefYasimini Ramadhani100% (1)
- Spinal Cord: Prof DR Nasaruddin Abdul AzizDocument54 pagesSpinal Cord: Prof DR Nasaruddin Abdul Azizkyoko08No ratings yet
- Brain Anatomy: Diencephalon, Brain Stem and Medulla SpinalisDocument36 pagesBrain Anatomy: Diencephalon, Brain Stem and Medulla SpinalisAngela FovinaNo ratings yet
- Cranial Nerves I-VI: NeuroanatomyDocument36 pagesCranial Nerves I-VI: NeuroanatomyGolden TamonNo ratings yet
- Spinal Cord: Prof DR Nasaruddin Abdul AzizDocument54 pagesSpinal Cord: Prof DR Nasaruddin Abdul AzizBJKines BjmcNo ratings yet
- Cranialnerve GokulDocument58 pagesCranialnerve Gokulgokulraja850No ratings yet
- 6 CerebellumDocument61 pages6 CerebellumNishanth LakshmanNo ratings yet
- FaceDocument74 pagesFacehazell_aseronNo ratings yet
- Anatomi Dan Fisiologi Sistem PersyarafanDocument37 pagesAnatomi Dan Fisiologi Sistem PersyarafanAnonymous xfBKTQfNo ratings yet
- Accessory &hypoglossal Nerve 2023Document19 pagesAccessory &hypoglossal Nerve 2023GanapathyGaneshNo ratings yet
- Cranial Nerves and Its ExaminationDocument136 pagesCranial Nerves and Its ExaminationNileshNo ratings yet
- Nervous TissueDocument34 pagesNervous TissueSameer MohammedNo ratings yet
- Cranial NervesDocument29 pagesCranial NervesMadalina DutanNo ratings yet
- Week 3 Spinal Cord, Spinal NervesDocument53 pagesWeek 3 Spinal Cord, Spinal NervesCyril Jay G. OrtegaNo ratings yet
- Week 3 Spinal Cord, Spinal NervesDocument53 pagesWeek 3 Spinal Cord, Spinal NervesHephzibah JaporNo ratings yet
- The Spinal CordDocument22 pagesThe Spinal Cordcy lifeNo ratings yet
- Sensory: Sensory (Ascending) Spinal TractsDocument24 pagesSensory: Sensory (Ascending) Spinal Tractsعبد الله الإمامNo ratings yet
- Presentation 1Document53 pagesPresentation 1rgroup331No ratings yet
- Cranial NervesDocument60 pagesCranial Nervestemesgen belayNo ratings yet
- Veterinary SanyiDocument576 pagesVeterinary SanyiHABTEMARIAM ERTBANNo ratings yet
- Knes 360 - 2021 Spring SyllabusDocument5 pagesKnes 360 - 2021 Spring SyllabusAbdullah KhanNo ratings yet
- Postural Orientation During Standing in Children With Bilateral Cerebral PalsyDocument7 pagesPostural Orientation During Standing in Children With Bilateral Cerebral PalsyRaul Vieira VillarroelNo ratings yet
- 3.03 Understand Structures, Functions and Disorders of The Nervous SystemDocument38 pages3.03 Understand Structures, Functions and Disorders of The Nervous SystemLoriwinchesterNo ratings yet
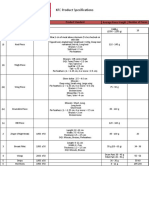
- KFC Poultry Product SpecificationsDocument1 pageKFC Poultry Product SpecificationsInaam Ur RehmanNo ratings yet
- Prolotherapy 101 - Dr. BrowningDocument51 pagesProlotherapy 101 - Dr. BrowningBRYAN GUZMAN BARRAGANNo ratings yet
- Lower Limb Neurological Examination OSCE GuideDocument15 pagesLower Limb Neurological Examination OSCE GuideLeen abusarhanNo ratings yet
- MAUREEN HVEGHOLM v. TIMOTHY EGANDocument9 pagesMAUREEN HVEGHOLM v. TIMOTHY EGANBen MargiottNo ratings yet
- Ajr 178 6 1781517Document5 pagesAjr 178 6 1781517आयुष चौधरीNo ratings yet
- 15 Minute Mat Challenge - Classic Flow 3 LongDocument4 pages15 Minute Mat Challenge - Classic Flow 3 Longma celine villoNo ratings yet
- Pointers To ReviewDocument18 pagesPointers To ReviewHegi Ann AlcalaNo ratings yet
- Systematically Attacking From Open Guard Seated Position-FlowChart 1.1Document1 pageSystematically Attacking From Open Guard Seated Position-FlowChart 1.1Josh Wexler0% (1)
- sm10 Hand Anatomy LessonDocument6 pagessm10 Hand Anatomy Lessonapi-383568582No ratings yet
- A Systematic Review of Evidence For Anterior Cruciate Ligament Rehabilitation How Much and What TDocument21 pagesA Systematic Review of Evidence For Anterior Cruciate Ligament Rehabilitation How Much and What TRuben CapelaNo ratings yet
- Ins510 Group Project ReportDocument17 pagesIns510 Group Project Reportradia amalin99No ratings yet
- Nursing Care Plans For Cruris Fracture: Case 1Document9 pagesNursing Care Plans For Cruris Fracture: Case 1susanti santaliaNo ratings yet
- CHAPTER III L-2 Dangers of StretchingDocument5 pagesCHAPTER III L-2 Dangers of StretchingJohn Mark PeñafielNo ratings yet
- NeoReviews January 2023Document58 pagesNeoReviews January 2023Ronald MHNo ratings yet
- Quadrimalleolar Fractures of The Ankle: Think 360°-A Step-By-Step Guide On Evaluation and FixationDocument3 pagesQuadrimalleolar Fractures of The Ankle: Think 360°-A Step-By-Step Guide On Evaluation and FixationFRANCISCONo ratings yet
- HemingwayDocument3 pagesHemingwayRemuló CustomNo ratings yet
- Splint Sling and TractionDocument43 pagesSplint Sling and TractionBisoy CincoNo ratings yet
- KBB 40X 201407Document11 pagesKBB 40X 20140723522352No ratings yet
- Analysis of Skeletal Remains - Worksheet: Sex Ancestry Age HeightDocument14 pagesAnalysis of Skeletal Remains - Worksheet: Sex Ancestry Age HeightMylan GastonNo ratings yet
- Duty Holder Review (DHR) : The Organisation/sDocument11 pagesDuty Holder Review (DHR) : The Organisation/sRob DouglasNo ratings yet
- Types of Bones Powerpoint Ver 1Document16 pagesTypes of Bones Powerpoint Ver 1mrejcrewsNo ratings yet
- Operating Instruction AG 500 A18 01 Operating Instruction PUB 5223807 000Document60 pagesOperating Instruction AG 500 A18 01 Operating Instruction PUB 5223807 000Nyein ZawNo ratings yet
- Spinal Stenosis 3Document8 pagesSpinal Stenosis 3hunter_axl01No ratings yet
- Orthopedic: Lec.11 DR - Hasan Abdulhadi.MDocument10 pagesOrthopedic: Lec.11 DR - Hasan Abdulhadi.MninaNo ratings yet
- Workbook I Semester ENGDocument228 pagesWorkbook I Semester ENGSuneel ReddyNo ratings yet
- Course Specification Emergency NursingDocument6 pagesCourse Specification Emergency NursingWael LotfyNo ratings yet