You might also like
- 4.1 Pemphigus: Case 38 Pemphigus Vulgaris (Involving The Skin and Oral Mucosa) BDocument16 pages4.1 Pemphigus: Case 38 Pemphigus Vulgaris (Involving The Skin and Oral Mucosa) BIrma NovitasariNo ratings yet
- Ulcerative Lesions of The Oral Mucosa: Yu Zhou, Xiaoying Li, Xin Jin, and Qianming ChenDocument20 pagesUlcerative Lesions of The Oral Mucosa: Yu Zhou, Xiaoying Li, Xin Jin, and Qianming ChenIrma NovitasariNo ratings yet
- Case 50 Oral Lichen Planus (Non-Erosive Type)Document19 pagesCase 50 Oral Lichen Planus (Non-Erosive Type)Irma NovitasariNo ratings yet
- Diskusi Kasus Epulis Granulomatosa - Danny Tandean - 2013Document16 pagesDiskusi Kasus Epulis Granulomatosa - Danny Tandean - 2013Danny TandeanNo ratings yet
- General Surgery SEQDocument15 pagesGeneral Surgery SEQFatima Arshad100% (1)
- FK Unpad - Draft Case 1.comulative ICDDocument30 pagesFK Unpad - Draft Case 1.comulative ICDVirgi AhmadNo ratings yet
- JIMENEZKaycelyn-Drus StudyDocument11 pagesJIMENEZKaycelyn-Drus Studykaycelyn jimenezNo ratings yet
- Pruritusani:Etiology Andmanagement: Katharine W. Markell,, Richard P. BillinghamDocument11 pagesPruritusani:Etiology Andmanagement: Katharine W. Markell,, Richard P. BillinghamSinue PumaNo ratings yet
- Acrodermatitis Enteropathica - A Case Report: Rashmi Mittal, Sudha R, Murugan S, Adikrishnan, Shobana S, Anandan SDocument3 pagesAcrodermatitis Enteropathica - A Case Report: Rashmi Mittal, Sudha R, Murugan S, Adikrishnan, Shobana S, Anandan SMarcelitaTaliaDuwiriNo ratings yet
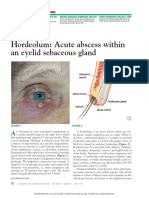
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Draft Case 2. Acne VulgarisDocument30 pagesDraft Case 2. Acne VulgarisVirgi AhmadNo ratings yet
- 1 s2.0 S2095754816301508 MainDocument4 pages1 s2.0 S2095754816301508 MainAnastasia PérezNo ratings yet
- KuretaseDocument3 pagesKuretaserindaNo ratings yet
- Lesi Dan Ulkus Dalam MulutDocument73 pagesLesi Dan Ulkus Dalam Mulutmega anggunNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
- Neonatal Sespsis - Drug StudyDocument5 pagesNeonatal Sespsis - Drug StudyAlvincent D. BinwagNo ratings yet
- Case History For ReferenceDocument24 pagesCase History For ReferenceSheethel MenonNo ratings yet
- Allergic Contact Stomatitis: A Case Report and Review of LiteratureDocument5 pagesAllergic Contact Stomatitis: A Case Report and Review of LiteratureFajar RamadhanNo ratings yet
- Treatment Plan 2Document11 pagesTreatment Plan 2api-547661785No ratings yet
- KMB III Kel 1 KonjungtivitisDocument19 pagesKMB III Kel 1 Konjungtivitisrkpngnz4xwNo ratings yet
- Paprsb Institute of Health Sciences Universiti Brunei DarussalamDocument10 pagesPaprsb Institute of Health Sciences Universiti Brunei DarussalamMasayuni_Fairu_6240No ratings yet
- 4th L-2, Gingival EnlargementDocument32 pages4th L-2, Gingival EnlargementReber ZebariNo ratings yet
- Jurnal PruritusDocument4 pagesJurnal Pruritusdvunsrat agt2021No ratings yet
- Drug Study FormatDocument4 pagesDrug Study Formatcabagnot.vanzjomariluizNo ratings yet
- LK - Alergi 1Document8 pagesLK - Alergi 1DewiSartikaNo ratings yet
- Gingival Enlargement - DelDocument64 pagesGingival Enlargement - DeldelsaNo ratings yet
- Prospective Aetiological Study of Diaper Dermatitis in The ElderlyDocument6 pagesProspective Aetiological Study of Diaper Dermatitis in The ElderlySamuel SammyNo ratings yet
- Ijpi 2 (2) 61-63Document3 pagesIjpi 2 (2) 61-63Tiara HapkaNo ratings yet
- Case Report Aphtous 2016Document4 pagesCase Report Aphtous 2016AbimsFardiansaNo ratings yet
- Treatment Plan Case #3 I. Assessment: Eshraga Abdelrazig DHIII AssignmentDocument11 pagesTreatment Plan Case #3 I. Assessment: Eshraga Abdelrazig DHIII Assignmentapi-547661785No ratings yet
- 2007 - Exfoliative Cheilitis A Case ReportDocument5 pages2007 - Exfoliative Cheilitis A Case ReportramaNo ratings yet
- Dentino Jurnal Kedokteran Gigi: Vol IV. No 1. Maret 2019Document4 pagesDentino Jurnal Kedokteran Gigi: Vol IV. No 1. Maret 2019Lidya DiandraNo ratings yet
- Crusted (Norwegian) Scabies Following Systemic and Topical Corticosteroid TherapyDocument4 pagesCrusted (Norwegian) Scabies Following Systemic and Topical Corticosteroid TherapysfiahyusnitaNo ratings yet
- Anti-Infective Therapy "Antibiotics": Definitions Chemotherapeutic Agent Anti-Microbial AgentDocument8 pagesAnti-Infective Therapy "Antibiotics": Definitions Chemotherapeutic Agent Anti-Microbial AgentMohamed EbrahimNo ratings yet
- DermatologyDocument3 pagesDermatologyDrkhslid890% (1)
- Drug Study Case PresDocument9 pagesDrug Study Case PresDaisy Jane TabonNo ratings yet
- Pharma S02 SBR05 Le02Document14 pagesPharma S02 SBR05 Le02sky vallartaNo ratings yet
- 7 CR 2 ArjunDocument4 pages7 CR 2 Arjunkiara wardanaNo ratings yet
- Dermatology CasesDocument4 pagesDermatology Casesejikieru03No ratings yet
- Assignment 2Document4 pagesAssignment 2AlabalaNo ratings yet
- DERMA Finals SamplexesDocument7 pagesDERMA Finals SamplexesKAREN MAE PADILLANo ratings yet
- Infectious Diseases Tabelle (Examen 6. Jahr)Document34 pagesInfectious Diseases Tabelle (Examen 6. Jahr)Aastha SethNo ratings yet
- JR IPM - Comprehensive Management of Oral Frailty in Multiple Systemic Disease Geriatric Patient (Case Report)Document30 pagesJR IPM - Comprehensive Management of Oral Frailty in Multiple Systemic Disease Geriatric Patient (Case Report)NUR HAYUNINGTYASNo ratings yet
- DocumentDocument5 pagesDocumentPRECIOUS LOVE LAGRIMASNo ratings yet
- JR IpmDocument85 pagesJR IpmNUR HAYUNINGTYASNo ratings yet
- 2024-Article Text-6560-1-10-20230128Document4 pages2024-Article Text-6560-1-10-20230128Adniana NareswariNo ratings yet
- Care Plan Template 1Document7 pagesCare Plan Template 1api-706689599No ratings yet
- Endo Assignment: Q1 / Write About Weeping CanalsDocument3 pagesEndo Assignment: Q1 / Write About Weeping Canalsعبد الرحمن خالد الزميليNo ratings yet
- 7a. Caria Complicata-PulpotomiaDocument64 pages7a. Caria Complicata-PulpotomiaNia AdibNo ratings yet
- Role of Zinc in Acne: A Study of 77 Patients: Original Research ArticleDocument5 pagesRole of Zinc in Acne: A Study of 77 Patients: Original Research ArticleEninta SriNo ratings yet
- Impaired Skin IntegrityDocument2 pagesImpaired Skin IntegrityEli AyaseNo ratings yet
- Weebly Care PlanDocument8 pagesWeebly Care Planapi-470528180No ratings yet
- Proton Pump Inhibitors vs. Histamine - Receptor Antagonists For Stress Ulcer ProphylaxisDocument19 pagesProton Pump Inhibitors vs. Histamine - Receptor Antagonists For Stress Ulcer ProphylaxisfbihansipNo ratings yet
- Metode SOAP 1Document19 pagesMetode SOAP 1rahmaNo ratings yet
- 6179 13644 1 SMDocument7 pages6179 13644 1 SMirma jovitaNo ratings yet
- Acad Dermatol Venereol - 2019 - Nowak - Rosacea Fulminans Coincidence of The Disease With Inflammatory Bowel DiseaseDocument2 pagesAcad Dermatol Venereol - 2019 - Nowak - Rosacea Fulminans Coincidence of The Disease With Inflammatory Bowel DiseasecamilabettiomatosNo ratings yet
- GIT OSPE Pathology - Final-2 PDFDocument29 pagesGIT OSPE Pathology - Final-2 PDFafaq alismailiNo ratings yet
- Benign Migratory Glossitis Report of A Rare Case With Review of LiteratureDocument3 pagesBenign Migratory Glossitis Report of A Rare Case With Review of LiteratureOjanNo ratings yet
- BDJ Paper On DentalDocument5 pagesBDJ Paper On DentalZihao WuNo ratings yet
- Lichen Planus, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandLichen Planus, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- 24 Hour Urine CollectionDocument11 pages24 Hour Urine CollectionKRIZIA ANE A. SULONGNo ratings yet
- True PDFDocument459 pagesTrue PDFAmna MmfNo ratings yet
- Rheumatoid Arthritis: Muhammad Afif Bin Mansor Andini Pratiwi Islami SupervisorDocument19 pagesRheumatoid Arthritis: Muhammad Afif Bin Mansor Andini Pratiwi Islami SupervisorAfif MansorNo ratings yet
- Bag Valve Mask Ventilation: Topic OutlineDocument4 pagesBag Valve Mask Ventilation: Topic OutlineDan Dan ManaoisNo ratings yet
- Changes in Preventive Care Benefits Due To Health Care ReformDocument3 pagesChanges in Preventive Care Benefits Due To Health Care Reformv4meetNo ratings yet
- MCP AbxDocument34 pagesMCP AbxShynne RPhNo ratings yet
- ConjunctivitisDocument2 pagesConjunctivitist304pkNo ratings yet
- Gerontology Mastery Ronald-Librando PDFDocument2 pagesGerontology Mastery Ronald-Librando PDFARISNo ratings yet
- An Observational Study Use of Systemic Antibiotics For Endodontic Infections TreatmentDocument17 pagesAn Observational Study Use of Systemic Antibiotics For Endodontic Infections TreatmentAthenaeum Scientific PublishersNo ratings yet
- Laparoscopic Correction of Perforated Peptic Ulcer First Choice A Review of LiteratureDocument9 pagesLaparoscopic Correction of Perforated Peptic Ulcer First Choice A Review of LiteratureLe Hu ThaNo ratings yet
- Feline Panleukopenia Virus Infection and Other Viral EnteritidesDocument8 pagesFeline Panleukopenia Virus Infection and Other Viral EnteritidesjohanNo ratings yet
- Lung MycosisDocument80 pagesLung MycosisWisnu Omadi100% (2)
- Marshall 2015Document13 pagesMarshall 2015MalikinNadalNo ratings yet
- Paper 3 Argumentative Essay Alexis-2Document9 pagesPaper 3 Argumentative Essay Alexis-2api-314832012No ratings yet
- 10-Week Physical Activity Program For A Hypertensive Obese AdultDocument19 pages10-Week Physical Activity Program For A Hypertensive Obese AdultPhysiotherapist AliNo ratings yet
- Disease Impact 2Document31 pagesDisease Impact 2Seed Rock ZooNo ratings yet
- ParasitesDocument22 pagesParasitesJames LeeNo ratings yet
- Philippine CPG-2013-uti in Adults-Part1 PDFDocument82 pagesPhilippine CPG-2013-uti in Adults-Part1 PDFVirginia AbalosNo ratings yet
- CLD CaseDocument12 pagesCLD Casemed.student657No ratings yet
- Mẫu giấy KSK song ngữDocument3 pagesMẫu giấy KSK song ngữNguyen LawlietNo ratings yet
- Microbiology Module 7 - BacilliDocument87 pagesMicrobiology Module 7 - BacilliArt Arts100% (1)
- Fitness Choices and First Aid Study NotesDocument11 pagesFitness Choices and First Aid Study NotesAlan VanNo ratings yet
- Anisocoria: What Is It?Document6 pagesAnisocoria: What Is It?Cristina ScerbatiucNo ratings yet
- Nso 24 Hour Urine Collection-FormillezaDocument4 pagesNso 24 Hour Urine Collection-FormillezaPatricia FormillezaNo ratings yet
- Chapter 64:: Morphea and Lichen SclerosusDocument21 pagesChapter 64:: Morphea and Lichen Sclerosuss02579No ratings yet
- Coronary Artery DiseaseDocument3 pagesCoronary Artery DiseaseMarta Luquez RNo ratings yet
- Bosu 2015Document24 pagesBosu 2015José Carlos Sánchez-RamirezNo ratings yet
- OPT B1 EE Units5-6 WorksheetDocument2 pagesOPT B1 EE Units5-6 WorksheetANA CORTESNo ratings yet
- Leukemia CaseDocument28 pagesLeukemia CasehilalNo ratings yet
- Mitral Valve SurgeryDocument2 pagesMitral Valve SurgeryLena MarieNo ratings yet