You might also like
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionFrom EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNo ratings yet
- HIV Prevention in Primary Care Practice: A PrEP PrimerFrom EverandHIV Prevention in Primary Care Practice: A PrEP PrimerNo ratings yet
- Local Studies and LiteratureDocument9 pagesLocal Studies and LiteratureKarl GutierrezNo ratings yet
- 1 s2.0 S2666535222000349 MainDocument7 pages1 s2.0 S2666535222000349 Mainشهد موسىNo ratings yet
- A Cross-National Study of Factors Associated With Women's Perinatal Mental Health and Wellbeing During The COVID-19 PandemicDocument3 pagesA Cross-National Study of Factors Associated With Women's Perinatal Mental Health and Wellbeing During The COVID-19 PandemicLaili MasrurohNo ratings yet
- Acceptability For COVID-19 Vaccination - Perspectives From MuslimsDocument9 pagesAcceptability For COVID-19 Vaccination - Perspectives From MuslimsPediatrics Department OPD CRMCNo ratings yet
- Discussion: Beier ME, 2003Document5 pagesDiscussion: Beier ME, 2003Sanghita MayalaganNo ratings yet
- ვაქცინაცია სტუდებტებშDocument6 pagesვაქცინაცია სტუდებტებშTengiz VerulavaNo ratings yet
- RESEARCH 1 Fi 2Document20 pagesRESEARCH 1 Fi 2Alondra SagarioNo ratings yet
- Health System Quality and COVID-19 Vaccination. A Cross-Sectional Analysis in 14 CountriesDocument10 pagesHealth System Quality and COVID-19 Vaccination. A Cross-Sectional Analysis in 14 Countriesluis sanchezNo ratings yet
- Assessment of Attitude of Nursing Mothers Towards Childhood Immunization in Some Selected Communities in Bali, LGA of Taraba StateDocument56 pagesAssessment of Attitude of Nursing Mothers Towards Childhood Immunization in Some Selected Communities in Bali, LGA of Taraba StateJoshua Bature SamboNo ratings yet
- My ProjectDocument38 pagesMy ProjectfaizamuhammadaligmlNo ratings yet
- Factors Affecting Covid 19 Vaccine Hesitancy Final Manuscript PDFDocument60 pagesFactors Affecting Covid 19 Vaccine Hesitancy Final Manuscript PDFMark Gideon WallisNo ratings yet
- Badr DKK 2021Document17 pagesBadr DKK 2021WoogyuNo ratings yet
- Final PaperDocument32 pagesFinal PaperGabriel AntolinNo ratings yet
- 299 ArabicDocument9 pages299 ArabicTinkhaniMbichilaNo ratings yet
- Literature Review ImmunizationDocument6 pagesLiterature Review Immunizationaflskdwol100% (1)
- Vaccine Willing-WPS OfficeDocument14 pagesVaccine Willing-WPS OfficeNorhani PanayamanNo ratings yet
- According To CSS Conducted By, in Partnership With The University of Maryland Conducted in 200 CountriesDocument3 pagesAccording To CSS Conducted By, in Partnership With The University of Maryland Conducted in 200 CountriesShipra BaruaNo ratings yet
- RRL 01 07 22Document9 pagesRRL 01 07 22Ponce GuerreroNo ratings yet
- Lived Experiences of Individuals With Sexually Transmitted Infections (STIs) : An Input To Infectious Disease Awareness and PreventionDocument12 pagesLived Experiences of Individuals With Sexually Transmitted Infections (STIs) : An Input To Infectious Disease Awareness and PreventionPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Chapter I-1Document3 pagesChapter I-1Secret AdmirerNo ratings yet
- The Nature and Extent of COVID 19 Vaccination Hesitancy in Healthcare WorkersDocument8 pagesThe Nature and Extent of COVID 19 Vaccination Hesitancy in Healthcare WorkersamiryahiaNo ratings yet
- The World Health OrganizationDocument4 pagesThe World Health Organizationampal100% (1)
- Knoweledge Perception and Attitudes of Mothers Having Children Undren Five About Vaccination in PunjabDocument14 pagesKnoweledge Perception and Attitudes of Mothers Having Children Undren Five About Vaccination in PunjabKinzaNo ratings yet
- Interventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsDocument10 pagesInterventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsMariaNo ratings yet
- Vaccines 09 01348Document12 pagesVaccines 09 01348Healthcare Pro LearningNo ratings yet
- Research Paper On Child VaccinationsDocument7 pagesResearch Paper On Child Vaccinationspwvgqccnd100% (1)
- Knowledge, Attitudes and Practices (KAP) Towards Vaccinations in The School Settings: An Explorative SurveyDocument13 pagesKnowledge, Attitudes and Practices (KAP) Towards Vaccinations in The School Settings: An Explorative Surveymary ann masayonNo ratings yet
- Final PaperDocument44 pagesFinal PaperForshia Antonette BañaciaNo ratings yet
- COVID-19 Vaccine Brand Hesitancy and Other Challenges To Vaccination in The Philippines - PLOS Global Public HealthDocument15 pagesCOVID-19 Vaccine Brand Hesitancy and Other Challenges To Vaccination in The Philippines - PLOS Global Public Healthprincess catherine PabellanoNo ratings yet
- 2371 - Parents' Attitudes Regarding Childhood Vaccination With Focus On Rotavirus Vaccination in Bishkek, KyrgyzstanDocument8 pages2371 - Parents' Attitudes Regarding Childhood Vaccination With Focus On Rotavirus Vaccination in Bishkek, KyrgyzstanMustafa YılmazNo ratings yet
- Synopsis FinalDocument9 pagesSynopsis FinalHira AliNo ratings yet
- Kaisa Study Final Paper Super FinalDocument114 pagesKaisa Study Final Paper Super FinalEunice RiveraNo ratings yet
- Factors Impacting Antiretroviral Therapy Adherence Among Human Immunodeficiency Virus-Positive Adolescents in Sub-Saharan AfricaDocument12 pagesFactors Impacting Antiretroviral Therapy Adherence Among Human Immunodeficiency Virus-Positive Adolescents in Sub-Saharan AfricaDouglas ChukwuNo ratings yet
- Knowledge and Preventive Practices of Mother To Child Transmission (PMTCT) Services Among Pregnant Women in Calabar MunicipalityDocument38 pagesKnowledge and Preventive Practices of Mother To Child Transmission (PMTCT) Services Among Pregnant Women in Calabar MunicipalitySolomonNo ratings yet
- Wagner 2020Document10 pagesWagner 2020Sue TudtudNo ratings yet
- The Awareness Level On The Benefit1Document12 pagesThe Awareness Level On The Benefit1Joshua ValledorNo ratings yet
- Degree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentDocument24 pagesDegree of Acceptance of Residents Barangay Bibincahan To Vaccination Program of The Philippine GovernmentRJ DealcaNo ratings yet
- The Challenges of Success: Adolescents With Perinatal HIV InfectionDocument3 pagesThe Challenges of Success: Adolescents With Perinatal HIV InfectionWardiati YusufNo ratings yet
- Knowledge, Attitude and Practice of Mothers Toward Children's Obligatory VaccinationDocument7 pagesKnowledge, Attitude and Practice of Mothers Toward Children's Obligatory VaccinationkrishnasreeNo ratings yet
- Factors Affecting COVID-19 Vaccine Acceptance: An International Survey Among Low-And Middle-Income CountriesDocument19 pagesFactors Affecting COVID-19 Vaccine Acceptance: An International Survey Among Low-And Middle-Income Countriesmercadia5997No ratings yet
- Parental Decision Making On Childhood Vaccine - Final PaperDocument105 pagesParental Decision Making On Childhood Vaccine - Final PaperOH WELL100% (1)
- Vaccines 08 00124 PDFDocument21 pagesVaccines 08 00124 PDFSaúl Alberto Kohan BocNo ratings yet
- Pediatric Melatonin IngestionsDocument5 pagesPediatric Melatonin IngestionsNational Content DeskNo ratings yet
- Pediatr Clin North Am 2023 Tabla de ContenidoDocument4 pagesPediatr Clin North Am 2023 Tabla de ContenidocdsaludNo ratings yet
- Related-LitDocument4 pagesRelated-LitBianca Alexy MataNo ratings yet
- Reviw of LiteratureDocument8 pagesReviw of LiteratureSarika RaneNo ratings yet
- Vaccine Access and Hesitancy: The Public Health Importance of VaccinesDocument30 pagesVaccine Access and Hesitancy: The Public Health Importance of VaccinesJmarie Brillantes PopiocoNo ratings yet
- Tmp320e TMPDocument6 pagesTmp320e TMPFrontiersNo ratings yet
- DISCUSSION-WPS OfficeDocument11 pagesDISCUSSION-WPS OfficeNorhani PanayamanNo ratings yet
- Tugas Ulang Metodologi PenelitianDocument55 pagesTugas Ulang Metodologi PenelitianMuhammad Candra R.ANo ratings yet
- Chelsey (Chapter 2 RRL) LocalDocument3 pagesChelsey (Chapter 2 RRL) LocalChester ArenasNo ratings yet
- Research PCM 4 Group 2Document23 pagesResearch PCM 4 Group 2Busay VelosoNo ratings yet
- Topics For MCNDocument5 pagesTopics For MCNHulyenNo ratings yet
- Pagpahiangay Sa Programang Pagbakuna Adaptive Immunization Program XUJPRSM 1Document34 pagesPagpahiangay Sa Programang Pagbakuna Adaptive Immunization Program XUJPRSM 1aerahengNo ratings yet
- 1-5 CombineDocument72 pages1-5 CombineDan Agyemang NketiahNo ratings yet
- VasavanSharangi Assign1Document4 pagesVasavanSharangi Assign1sharangiivNo ratings yet
- Knowledge About Obstetric Danger Signs and Associated Factors Among Antenatal Care AttendantsDocument7 pagesKnowledge About Obstetric Danger Signs and Associated Factors Among Antenatal Care AttendantsIJPHSNo ratings yet
- The Awareness Level On The Benefit1Document10 pagesThe Awareness Level On The Benefit1Joshua ValledorNo ratings yet
- 80 RecommendationDocument16 pages80 Recommendationarthik603No ratings yet
- SPTL Ohs&e 40 Ohse MPR AbrarDocument22 pagesSPTL Ohs&e 40 Ohse MPR AbrarRanjeet Kumar SinghNo ratings yet
- 6 Dayu+Agung+Sawitri Galley FinalDocument9 pages6 Dayu+Agung+Sawitri Galley FinalNicholas PratamaNo ratings yet
- Sample Survey - HMO Study - 20HMO - 20studyDocument19 pagesSample Survey - HMO Study - 20HMO - 20studyHebatallah FahmyNo ratings yet
- 5014-Prescription Regulation TableDocument3 pages5014-Prescription Regulation Tableritchelle abigail mataNo ratings yet
- LPN CourseworkDocument7 pagesLPN Courseworkbcqvdfyg100% (2)
- Affiliated Institutes Public (Technologies)Document3 pagesAffiliated Institutes Public (Technologies)ahsanNo ratings yet
- Care Freedom (Health Insurance Product) - Policy T&C (Effective From 01 October 2020)Document44 pagesCare Freedom (Health Insurance Product) - Policy T&C (Effective From 01 October 2020)rakesh08nagarNo ratings yet
- Law550:Labour and Industrial Laws-Ii: Session 2020-21 Page:1/1Document1 pageLaw550:Labour and Industrial Laws-Ii: Session 2020-21 Page:1/1Mansi MalikNo ratings yet
- Convenios Colectivos de TrabajoDocument4 pagesConvenios Colectivos de TrabajoRosmary Cahuana ContrerasNo ratings yet
- OKAY SA DEPED DIVISION KICK OFF Technical Working GroupDocument3 pagesOKAY SA DEPED DIVISION KICK OFF Technical Working Groupalelie santosNo ratings yet
- SickLeaveCertificate With and Without Diagnosis 20240227 144109Document2 pagesSickLeaveCertificate With and Without Diagnosis 20240227 144109Sawad SawaNo ratings yet
- Providers 202310200719Document26 pagesProviders 202310200719Vamsi Krishna GarimellaNo ratings yet
- 2010-0019-A (Amendment) Establishment of A National Progr - Am For Sharing of Organs From Deceased Donors Pertinent To Section VII.5Document2 pages2010-0019-A (Amendment) Establishment of A National Progr - Am For Sharing of Organs From Deceased Donors Pertinent To Section VII.5Bea MagbanuaNo ratings yet
- Form 2A. Laboratory Request and Result Form: To Be Filled Out by Health WorkerDocument1 pageForm 2A. Laboratory Request and Result Form: To Be Filled Out by Health WorkerJuvy Micutuan100% (2)
- Post Basic Pharmacist Assistant Learnership OpportunityDocument1 pagePost Basic Pharmacist Assistant Learnership Opportunitynonduduzo ntombi kheswaNo ratings yet
- Out Patient Department OPD PDFDocument64 pagesOut Patient Department OPD PDFDAD SHOTS100% (1)
- Systems Approach To Medication Safety CSMC Final 2023Document67 pagesSystems Approach To Medication Safety CSMC Final 2023Keltian LaurenteNo ratings yet
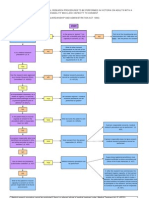
- Approval Process For Medical Research FlowchartDocument1 pageApproval Process For Medical Research FlowchartabcdcattigerNo ratings yet
- CH 1 Primary Health Care-VleDocument47 pagesCH 1 Primary Health Care-VleErnie SyarinaNo ratings yet
- De Castrofamily-NcpDocument2 pagesDe Castrofamily-NcpGwen De CastroNo ratings yet
- Wait Times To Medical Care and Treatment in Canada: LAWS-6046 - (34) - 22S - Emily PassanhaDocument10 pagesWait Times To Medical Care and Treatment in Canada: LAWS-6046 - (34) - 22S - Emily Passanhaemily passanhaNo ratings yet
- MR HQ Doctor Name Gender Area/Patch UIN Speciality UIN QualificationDocument18 pagesMR HQ Doctor Name Gender Area/Patch UIN Speciality UIN QualificationMeeraNo ratings yet
- RIANDINI PRAMUDITA RIYANTI ResultDocument1 pageRIANDINI PRAMUDITA RIYANTI ResultRiandini Pramudita RNo ratings yet
- Annalea Jamin: BSN, RN, CCM, CCRN-KDocument1 pageAnnalea Jamin: BSN, RN, CCM, CCRN-Kapi-613472231No ratings yet
- Policy On Complementary and Alternative Therapies in Nursing and Midwifery PracticeDocument3 pagesPolicy On Complementary and Alternative Therapies in Nursing and Midwifery Practicelilahgreeny100% (1)
- Skills Laboratory Cyclical RotationDocument17 pagesSkills Laboratory Cyclical RotationFau Fau DheoboNo ratings yet
- NCP Palliative Care Model of Care 24 04 0219Document175 pagesNCP Palliative Care Model of Care 24 04 0219Inggrit SuniNo ratings yet
- Who Is A ScientistDocument7 pagesWho Is A ScientistTianna MorganNo ratings yet
- 3021 Reflective JournalDocument5 pages3021 Reflective Journalapi-660581645No ratings yet