You might also like
- Clinical PharmacyDocument16 pagesClinical Pharmacyblossoms_diyya299850% (6)
- SOL Diploma NursingDocument22 pagesSOL Diploma NursingNonso NwakaNo ratings yet
- An Exploratory Metasynthesis of Midwifery Practice in The United StatesDocument13 pagesAn Exploratory Metasynthesis of Midwifery Practice in The United Statesintan megaNo ratings yet
- Midwifery Evidence Based Practice March 2013 PDFDocument11 pagesMidwifery Evidence Based Practice March 2013 PDFFthrahmawatiNo ratings yet
- Research Priorities in Obstetrics SeminarDocument7 pagesResearch Priorities in Obstetrics SeminarSharmistha Debnath83% (6)
- The Double-Edged Scalpel: Experiences and Perceptions of Pregnancy and Parenthood During Canadian Surgical Residency TrainingDocument11 pagesThe Double-Edged Scalpel: Experiences and Perceptions of Pregnancy and Parenthood During Canadian Surgical Residency TrainingNikhil ChoudharyNo ratings yet
- 2A Review of Gynecologic Oncology in TheDocument10 pages2A Review of Gynecologic Oncology in TheRaul A UrbinaNo ratings yet
- Impact of Gender Bias On Male Nursing Students Competence of SkillsDocument13 pagesImpact of Gender Bias On Male Nursing Students Competence of Skillsapi-526815418No ratings yet
- Barriers Prenatal Care For Low-Income: Articles ToDocument6 pagesBarriers Prenatal Care For Low-Income: Articles ToSteph PaulinoNo ratings yet
- Perception of Child Bearing Women Towards Male Involvement in Midwifery Practice in Family Support Programme (FSP) Clinic Yenagoa, NigeriaDocument8 pagesPerception of Child Bearing Women Towards Male Involvement in Midwifery Practice in Family Support Programme (FSP) Clinic Yenagoa, NigeriaIOSRjournal100% (1)
- Obstetric Care Consensus No2Document14 pagesObstetric Care Consensus No2Marco DiestraNo ratings yet
- Performance of Male Midwives in The Different Hospitals and Clinics in KalingaDocument8 pagesPerformance of Male Midwives in The Different Hospitals and Clinics in KalingaIJELS Research JournalNo ratings yet
- Xepoleas2020 Article TheExperiencesOfFemaleSurgeonsDocument28 pagesXepoleas2020 Article TheExperiencesOfFemaleSurgeonsOpeyemi OyeyemiNo ratings yet
- Presentation ON Parse'S Human Becoming Theory: Submitted To, Submitted byDocument10 pagesPresentation ON Parse'S Human Becoming Theory: Submitted To, Submitted byJeevana RoseNo ratings yet
- Women's Perceptions of Access To Prenatal Care in The United States: A Literature ReviewDocument7 pagesWomen's Perceptions of Access To Prenatal Care in The United States: A Literature ReviewOncología CdsNo ratings yet
- Challenges in Older Women’s Health: A Guide for CliniciansFrom EverandChallenges in Older Women’s Health: A Guide for CliniciansHeidi W. BrownNo ratings yet
- Kennedy 2018Document8 pagesKennedy 2018rahma nuril ilmiNo ratings yet
- Contemporary Issue PaperDocument6 pagesContemporary Issue Paperapi-641793379No ratings yet
- Literature Review On StillbirthDocument6 pagesLiterature Review On Stillbirthaflsvagfb100% (1)
- Health Issues Paper Nursing ShortageDocument11 pagesHealth Issues Paper Nursing Shortageapi-570216075No ratings yet
- Breastfeeding Disparities and Their Mediators in An Urban Birth Cohort of Black and White MothersDocument11 pagesBreastfeeding Disparities and Their Mediators in An Urban Birth Cohort of Black and White Mothersapi-625120170No ratings yet
- Research 1Document7 pagesResearch 1hala yehiaNo ratings yet
- Health Professionals ' Views On Maternity Care For Women With Physical Disabilities: A Qualitative StudyDocument11 pagesHealth Professionals ' Views On Maternity Care For Women With Physical Disabilities: A Qualitative StudyNabilaNo ratings yet
- Mod 5 - Issue PaperDocument9 pagesMod 5 - Issue Paperapi-569838480No ratings yet
- The Ethics of Perinatal Care For Black WomenDocument8 pagesThe Ethics of Perinatal Care For Black Womenapi-625120170No ratings yet
- Group Apa PaperDocument10 pagesGroup Apa Paperapi-268209871No ratings yet
- Generational Differences in Nurses' Characteristics, Job Satisfaction, Quality of Work Life, and Psychological EmpowermentDocument11 pagesGenerational Differences in Nurses' Characteristics, Job Satisfaction, Quality of Work Life, and Psychological EmpowermentPurnama YunusNo ratings yet
- 10.7556 Jaoa.2005.105.8.369Document11 pages10.7556 Jaoa.2005.105.8.369Usman AR VainceNo ratings yet
- Implications For Nursing and Childbearing Beliefs and PracticesDocument8 pagesImplications For Nursing and Childbearing Beliefs and Practicesعبدالمحسن علي ENo ratings yet
- Maternal Health Organizations Announce New CoalitionDocument1 pageMaternal Health Organizations Announce New CoalitionNatasha HuntNo ratings yet
- Chapter 5 (Maternal)Document47 pagesChapter 5 (Maternal)Veloria AbegailNo ratings yet
- Family Support and Self-Esteem of Patient With Breast CancerDocument5 pagesFamily Support and Self-Esteem of Patient With Breast CancerDean Rex Azriel TelaumbanuaNo ratings yet
- 05 N293 28654Document22 pages05 N293 28654piyush0751No ratings yet
- The Role of Nursing in Cervical Cancer Prevention and TreatmentDocument5 pagesThe Role of Nursing in Cervical Cancer Prevention and TreatmentLytiana WilliamsNo ratings yet
- Lit Review NealeDocument9 pagesLit Review Nealeapi-726948535No ratings yet
- Midwifery Care at A Freestanding Birth Center: A Safe and Effective Alternative To Conventional Maternity CareDocument20 pagesMidwifery Care at A Freestanding Birth Center: A Safe and Effective Alternative To Conventional Maternity CareYulinda AswanNo ratings yet
- Global Health Paper 2Document18 pagesGlobal Health Paper 2Chelsea RuthrauffNo ratings yet
- Improving Mammography ScreeningDocument8 pagesImproving Mammography ScreeningsylviaramisNo ratings yet
- Use of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelDocument7 pagesUse of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelEndahNo ratings yet
- J Midwife Womens Health - 2019 - Carlson - Preventing Cesarean Birth in Women With Obesity Influence of Unit LevelDocument12 pagesJ Midwife Womens Health - 2019 - Carlson - Preventing Cesarean Birth in Women With Obesity Influence of Unit LevelArny MoscosoNo ratings yet
- Use of and Attitudes and Knowledge About Pap Smears Among Women in KuwaitDocument18 pagesUse of and Attitudes and Knowledge About Pap Smears Among Women in KuwaitHanisha EricaNo ratings yet
- Hiring Foreign Nurses FinalDocument12 pagesHiring Foreign Nurses Finalapi-444844610No ratings yet
- ComparisonofcnmvsmdcareDocument9 pagesComparisonofcnmvsmdcarePandora HardtmanNo ratings yet
- Nursing Baccalaurate Comp PDFDocument22 pagesNursing Baccalaurate Comp PDFNoor AzizahNo ratings yet
- Estimating The Period Prevalence of Mothers Who Have Abortions: A Population Based Study of Inclusive Pregnancy OutcomesDocument7 pagesEstimating The Period Prevalence of Mothers Who Have Abortions: A Population Based Study of Inclusive Pregnancy OutcomesGiulianaNo ratings yet
- MCN 12520Document9 pagesMCN 12520Michael ThomasNo ratings yet
- Psychological Evaluations For Assisted Reproductive Intervention: Guidelines For Clinical PracticeDocument8 pagesPsychological Evaluations For Assisted Reproductive Intervention: Guidelines For Clinical PracticeandreaNo ratings yet
- Midwifery: Kelly Ackerson, PHD, RN, WHNP-BC, Ruth Zielinski, PHD, CNM, FacnmDocument26 pagesMidwifery: Kelly Ackerson, PHD, RN, WHNP-BC, Ruth Zielinski, PHD, CNM, FacnmMILANo ratings yet
- Abel Man 2020Document6 pagesAbel Man 2020Redouane idrissiNo ratings yet
- 2020 Article 5890Document779 pages2020 Article 5890desa jotonNo ratings yet
- Contraception Counseling and Use Among AdolescentDocument6 pagesContraception Counseling and Use Among AdolescentAbdulrahman Al-otaibiNo ratings yet
- Nursing ShortageDocument6 pagesNursing Shortageapi-455530517No ratings yet
- Literature Evaluation Table: Student Name Lecturers Name Institution Course DateDocument7 pagesLiterature Evaluation Table: Student Name Lecturers Name Institution Course DateTony MutisyaNo ratings yet
- The Feminine Vs Masculine Nurse - The Effects of Gender StereotypeDocument37 pagesThe Feminine Vs Masculine Nurse - The Effects of Gender Stereotypeannni9955No ratings yet
- Mja16 00844Document5 pagesMja16 00844Farah SajidahNo ratings yet
- The Evolving Role of Midwives As Laborists: Original ReviewDocument8 pagesThe Evolving Role of Midwives As Laborists: Original Reviewmnazri98No ratings yet
- Maternal and Infant HealthDocument7 pagesMaternal and Infant Healthintellectual_masterNo ratings yet
- Kem MaternitasDocument8 pagesKem MaternitassherlyNo ratings yet
- Knowledge Attitude and Practice of ContraceptiveDocument5 pagesKnowledge Attitude and Practice of ContraceptiveSam AdeNo ratings yet
- Acog Distrrict Xi and CTCNM PolicyDocument4 pagesAcog Distrrict Xi and CTCNM Policyapi-260169062No ratings yet
- Lactation Induction in A Transgender WomanDocument6 pagesLactation Induction in A Transgender WomanM S de BarrosNo ratings yet
- Picopaper FinalDocument10 pagesPicopaper Finalapi-238698438No ratings yet
- Domain 3 Population Health DRAFTDocument2 pagesDomain 3 Population Health DRAFTthersaNo ratings yet
- Upload - PDs - 35717-KPI Guide For StaffDocument5 pagesUpload - PDs - 35717-KPI Guide For StaffBilal Salameh100% (1)
- Compassion Fatigue Are You at RiskDocument1 pageCompassion Fatigue Are You at RisknitistudyaccNo ratings yet
- Acutebrainfailure: Pathophysiology, Diagnosis, Management, and Sequelae of DeliriumDocument59 pagesAcutebrainfailure: Pathophysiology, Diagnosis, Management, and Sequelae of DeliriumdarlingcarvajalduqueNo ratings yet
- Daguay, Sibal (Prelims)Document10 pagesDaguay, Sibal (Prelims)April Mergelle LapuzNo ratings yet
- MensahDocument2 pagesMensahapi-604656125No ratings yet
- The Role of The Physical Environment in The Hospital of The 21st Century: A Oncein - A-Lifetime OpportunityDocument100 pagesThe Role of The Physical Environment in The Hospital of The 21st Century: A Oncein - A-Lifetime OpportunityPamela A. Sanz AbarcaNo ratings yet
- Rapid Assessment of Patients in Distress: CommentaryDocument2 pagesRapid Assessment of Patients in Distress: CommentarydwiyantoroNo ratings yet
- Safe Administrations of Medications (Draft Chapter)Document74 pagesSafe Administrations of Medications (Draft Chapter)Caleb FellowesNo ratings yet
- Corporate Culture and Health Care Organization:, IncludingDocument25 pagesCorporate Culture and Health Care Organization:, IncludingizzykhalNo ratings yet
- Bag Technique 2 UCDocument2 pagesBag Technique 2 UCSoleil Maxwell0% (1)
- BAP Guidelines PerinatalDocument34 pagesBAP Guidelines Perinatalrocsa11No ratings yet
- Health NotesDocument2 pagesHealth NotesKEICHIE QUIMCONo ratings yet
- Brgy Health Plan 2019Document18 pagesBrgy Health Plan 2019Napieh Bulalaque Polistico100% (1)
- PartogramDocument20 pagesPartogramKasumba ChandaNo ratings yet
- 18-294 - CDG CSD Hba1c (1 X 2 M) Pull-Up (Diastika) - Ind - PrintDocument1 page18-294 - CDG CSD Hba1c (1 X 2 M) Pull-Up (Diastika) - Ind - PrintHinama ChenNo ratings yet
- Letter To HDC Re Medical Code of Ethics by Roger BrookingDocument7 pagesLetter To HDC Re Medical Code of Ethics by Roger BrookingRoger BrookingNo ratings yet
- Radiotherapy For Locally Advanced Resectable T3 - T4 Laryngeal Cancer - Does Laryngeal Preservation Strategy Compromise Survival?Document14 pagesRadiotherapy For Locally Advanced Resectable T3 - T4 Laryngeal Cancer - Does Laryngeal Preservation Strategy Compromise Survival?andre halimNo ratings yet
- Leading Causes of Preventable Death: Secondary PreventionDocument3 pagesLeading Causes of Preventable Death: Secondary PreventionAriel GonzalesNo ratings yet
- CV For NMHDocument3 pagesCV For NMHmorganmicah6No ratings yet
- Develop Med Child Neuro - 2021 - Noten - ICF Core Sets For The Assessment of Functioning of Adults With Cerebral PalsyDocument9 pagesDevelop Med Child Neuro - 2021 - Noten - ICF Core Sets For The Assessment of Functioning of Adults With Cerebral Palsysandra garcia molinaNo ratings yet
- Clinical Perspectives On Psychological Disorders 5e: Richard P. Halgin Susan Krauss WhitbourneDocument22 pagesClinical Perspectives On Psychological Disorders 5e: Richard P. Halgin Susan Krauss WhitbourneElaine Joyce PasiaNo ratings yet
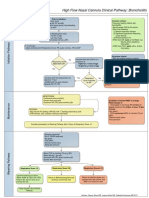
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDocument1 pageHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoNo ratings yet
- National Voluntary Blood Services Program (Philippines)Document2 pagesNational Voluntary Blood Services Program (Philippines)Charm Arroyo71% (7)
- Ambulatory AnesthesiaDocument45 pagesAmbulatory AnesthesiacardiacanesthesiaNo ratings yet
- IPCRF 1 NewDocument1 pageIPCRF 1 NewMARY JERICA OCUPENo ratings yet
- Pre Hospital CareDocument8 pagesPre Hospital Careshinichi kudoNo ratings yet
- Ayurvedic Medicine vs. Traditional Chinese MedicineDocument2 pagesAyurvedic Medicine vs. Traditional Chinese MedicineVolcana JupiterNo ratings yet