You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Management of Patients On Systemic Steroids - An Oral Surgery PerspectiveDocument7 pagesManagement of Patients On Systemic Steroids - An Oral Surgery PerspectiveMohammad Abdulmon’emNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 7sj61 ManualDocument29 pages7sj61 Manualpaari506No ratings yet
- Table 3-1. Project Management Process Group and Knowledge Area MappingDocument1 pageTable 3-1. Project Management Process Group and Knowledge Area MappingbuttgeeNo ratings yet
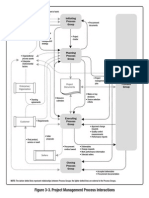
- PMI Process FlowDocument1 pagePMI Process FlowbuttgeeNo ratings yet
- MG Transformers and Packaged Substations TX5299.V2Document20 pagesMG Transformers and Packaged Substations TX5299.V2engnajeeb75No ratings yet
- PDC PMPHandbookDocument28 pagesPDC PMPHandbooksardarmkhanNo ratings yet
- Reactive Power CompensationDocument2 pagesReactive Power CompensationbuttgeeNo ratings yet
- Guia Espondilolistesis ÍstmicaDocument8 pagesGuia Espondilolistesis ÍstmicaELAR NAUN CARI CONDORINo ratings yet
- Ayush 341655Document7 pagesAyush 341655ਅਰਪਣਸਿੰਘNo ratings yet
- Nerve GlidingDocument11 pagesNerve GlidingnurfitriaNo ratings yet
- Community Health Nursing Course OutlinesDocument20 pagesCommunity Health Nursing Course OutlinesMATTHEW KIRARIT100% (1)
- Nursing Care Plan For Client With Ineffective Tissue PerfusionDocument2 pagesNursing Care Plan For Client With Ineffective Tissue PerfusionThe Right WayNo ratings yet
- Phenylephrine HydrochlorideDocument5 pagesPhenylephrine HydrochlorideSean Amir S. Savellano100% (1)
- Kardiotokografi Ppds (DR - JKS)Document68 pagesKardiotokografi Ppds (DR - JKS)Aditya PrabawaNo ratings yet
- Homeopathic Remedies: Remedy Traditional Use by Homeopaths NotesDocument8 pagesHomeopathic Remedies: Remedy Traditional Use by Homeopaths NotesAcharla SatyanarayanaNo ratings yet
- Epilepsy Overview and Revised Classification of Seizures and EpilepsiesDocument16 pagesEpilepsy Overview and Revised Classification of Seizures and EpilepsiesfabioNo ratings yet
- 2003 - Most Commony Used DrugsDocument376 pages2003 - Most Commony Used DrugsasdNo ratings yet
- Case Study-Incomplete AbortionDocument15 pagesCase Study-Incomplete AbortionJane Vi50% (6)
- Gordons 11 Health Pattern Guide Format and Questions Converted 1Document11 pagesGordons 11 Health Pattern Guide Format and Questions Converted 1Kim BadillesNo ratings yet
- Parkinsonism and Related DisordersDocument7 pagesParkinsonism and Related DisordersnellieauthorNo ratings yet
- Ebook Diagnostic Imaging Genitourinary PDF Full Chapter PDFDocument67 pagesEbook Diagnostic Imaging Genitourinary PDF Full Chapter PDFjade.burrow118100% (26)
- CS PresentationDocument38 pagesCS PresentationMarriam Malik100% (3)
- Lara Nasser: EducationDocument2 pagesLara Nasser: Educationapi-389185831No ratings yet
- Keerthana Kamboji Research Assesment 4 3a 10Document7 pagesKeerthana Kamboji Research Assesment 4 3a 10api-353150081No ratings yet
- A. Maternity and Newborn Medications: (MINT) MDocument4 pagesA. Maternity and Newborn Medications: (MINT) MErica Williams0% (1)
- Clinical Medicine 2Document231 pagesClinical Medicine 2Sree DharNo ratings yet
- Laboratory Request Form - TemplateDocument2 pagesLaboratory Request Form - TemplateShafiq Azam RumiNo ratings yet
- Paediatric Syrup-Injection-DropsDocument13 pagesPaediatric Syrup-Injection-DropsAminulNo ratings yet
- Cleft Lip Operation Tennison-Randall Vs MillardDocument25 pagesCleft Lip Operation Tennison-Randall Vs MillardIka.M.phoebe Alexander Lie100% (2)
- Nursing Management of Diabetes Mellitus: by Richard A. GuthrieDocument2 pagesNursing Management of Diabetes Mellitus: by Richard A. GuthrieStella GašparušNo ratings yet
- 7 Rights of Vaccine AdministrationDocument26 pages7 Rights of Vaccine AdministrationAnania ClementNo ratings yet
- BVGH-University of Rwanda Virtual Gynecologic Oncology CourseDocument43 pagesBVGH-University of Rwanda Virtual Gynecologic Oncology CourseEmmanuel NdikuryayoNo ratings yet
- Abrevieri V2Document9 pagesAbrevieri V2Smaranda-Elena MateiNo ratings yet
- Laser SafetyDocument3 pagesLaser SafetyEbaa BarghouthiNo ratings yet
- Module 4-Ethical Issues in Genetic TestingDocument65 pagesModule 4-Ethical Issues in Genetic Testingstlcajun55No ratings yet
- Lista de PreçoDocument10 pagesLista de PreçoEll AtalaiaNo ratings yet