You might also like
- Hazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleFrom EverandHazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleNo ratings yet
- Urban Rural Disparity Global Estimation of PM2.5Document13 pagesUrban Rural Disparity Global Estimation of PM2.5yohanes0gadiNo ratings yet
- The Nexus Between Energy and Health in Rural AreasDocument33 pagesThe Nexus Between Energy and Health in Rural AreasOlgaNo ratings yet
- Inhalation Exposure To Size-Segregated Fine Particles and Particulate PAHsDocument8 pagesInhalation Exposure To Size-Segregated Fine Particles and Particulate PAHsMuhammed yousufNo ratings yet
- Lung IndiaDocument8 pagesLung IndiaJitendra RajputNo ratings yet
- Er Celebi 2009Document10 pagesEr Celebi 2009Mr PolashNo ratings yet
- 1 s2.0 S0045653519301948 MainDocument6 pages1 s2.0 S0045653519301948 MainJohn Fernando Galeano MurciaNo ratings yet
- SCH Eepers 2019Document12 pagesSCH Eepers 2019Yoselin GomezNo ratings yet
- GJESM Volume 7 Issue 1 Pages 15-32Document18 pagesGJESM Volume 7 Issue 1 Pages 15-32GJESMNo ratings yet
- 1 s2.0 S026974911632718X MainDocument10 pages1 s2.0 S026974911632718X Mainmateo guerra londoñoNo ratings yet
- Life Cycle Environmental Impacts of InhalersDocument19 pagesLife Cycle Environmental Impacts of Inhalersstardust.m002No ratings yet
- Article in PressDocument13 pagesArticle in PressAndika ReinaldyNo ratings yet
- Environmental Pollution: Mengsi Deng, Pengchao Li, Ming Shan, Xudong YangDocument9 pagesEnvironmental Pollution: Mengsi Deng, Pengchao Li, Ming Shan, Xudong YangAksaralangit BudiyartoNo ratings yet
- Environmental Research: Jimyung Park, Hyung-Jun Kim, Chang-Hoon Lee, Chang Hyun Lee, Hyun Woo LeeDocument8 pagesEnvironmental Research: Jimyung Park, Hyung-Jun Kim, Chang-Hoon Lee, Chang Hyun Lee, Hyun Woo LeeJoaquim Lorenzetti BrancoNo ratings yet
- Jurnal Pembanding (Internasional)Document8 pagesJurnal Pembanding (Internasional)Elisabeth Anggelika NahampunNo ratings yet
- Generalized Additive Models Building Evidence of Air Pollution, ClimateDocument10 pagesGeneralized Additive Models Building Evidence of Air Pollution, ClimateblackalamzNo ratings yet
- J Apr 2020 01 008Document12 pagesJ Apr 2020 01 008Ashnab Zahid KhanNo ratings yet
- Literature Review ON Report On Indoor Air Quality Associated With WoodburningDocument21 pagesLiterature Review ON Report On Indoor Air Quality Associated With WoodburningEustache NIJEJENo ratings yet
- Chemical Burns - An Historical Comparison and Review of The LiteratureDocument5 pagesChemical Burns - An Historical Comparison and Review of The LiteratureAdharaaNo ratings yet
- Heliyon: Abinaya Sekar, George K. Varghese, M.K. Ravi VarmaDocument15 pagesHeliyon: Abinaya Sekar, George K. Varghese, M.K. Ravi VarmaYoselin GomezNo ratings yet
- The Effect of Propanolol and Metformin On Clinical Outcomes in Bu 2023 BurnsDocument9 pagesThe Effect of Propanolol and Metformin On Clinical Outcomes in Bu 2023 BurnsAdrian MoralesNo ratings yet
- Jurnal Sistem Pernafasan PDFDocument8 pagesJurnal Sistem Pernafasan PDFNOVALIA ROZA -No ratings yet
- Wei HuangDocument6 pagesWei Huangjulian rafael paez mauricioNo ratings yet
- Fullerton Et Al. - 2008 - Indoor Air Pollution From Biomass Fuel Smoke Is ADocument9 pagesFullerton Et Al. - 2008 - Indoor Air Pollution From Biomass Fuel Smoke Is ADawit DebashNo ratings yet
- Numerical Investigation of The Effect of Air Supply On Cook Stove PerformanceDocument12 pagesNumerical Investigation of The Effect of Air Supply On Cook Stove Performancesuraj ghiweNo ratings yet
- Biomonitoring Human Exposure To Household Air Pollution and Association With Self-Reported Health Symptoms - A Stove Intervention Study in PeruDocument9 pagesBiomonitoring Human Exposure To Household Air Pollution and Association With Self-Reported Health Symptoms - A Stove Intervention Study in Perualejandro toro riveraNo ratings yet
- Journal of Development Economics: ImeldaDocument18 pagesJournal of Development Economics: ImeldaMuhammad ImranNo ratings yet
- Halios Etal (2014) EMASDocument14 pagesHalios Etal (2014) EMASChristosNo ratings yet
- Dioxins 2007bDocument4 pagesDioxins 2007bBondi GevaoNo ratings yet
- 03 CE311A Source Apportionment of Indoor Air Pollutants in IIT Kanpur CampusDocument35 pages03 CE311A Source Apportionment of Indoor Air Pollutants in IIT Kanpur CampusRahul ChoudharyNo ratings yet
- 241 251 Gavriil - 401 - 8 3Document11 pages241 251 Gavriil - 401 - 8 3qbich37No ratings yet
- Drivers of The Adoption and Exclusive Use of Clean Fuel For Cooking in Sub-Saharan Africa: Learnings and Policy Considerations From CameroonDocument24 pagesDrivers of The Adoption and Exclusive Use of Clean Fuel For Cooking in Sub-Saharan Africa: Learnings and Policy Considerations From CameroonPyie Sone LinNo ratings yet
- Ap Effect On Lung FunctionDocument39 pagesAp Effect On Lung FunctionTechno CratNo ratings yet
- 1 s2.0 S0048969723054050 MainDocument10 pages1 s2.0 S0048969723054050 MainSurya HadiNo ratings yet
- Health in The Green Economy Briefing Energy enDocument6 pagesHealth in The Green Economy Briefing Energy enEmilline Law KwangNo ratings yet
- Toxicological Comparison of Cigarette Smoke and E-Cigarette Aerosol Using A 3D in Vitro Human Respiratory ModelDocument11 pagesToxicological Comparison of Cigarette Smoke and E-Cigarette Aerosol Using A 3D in Vitro Human Respiratory ModelGina Marcela Chaves HenriquezNo ratings yet
- Effects of The Occupational Exposure On Health Status Among Petroleum Station WorkersDocument6 pagesEffects of The Occupational Exposure On Health Status Among Petroleum Station WorkersTín TôNo ratings yet
- Energy EconomicsDocument11 pagesEnergy EconomicsCarlos AlvarezNo ratings yet
- Atmospheric EnvironmentDocument10 pagesAtmospheric EnvironmentbassbngNo ratings yet
- PHD ProposalDocument21 pagesPHD ProposalHAIMANOTNo ratings yet
- ECH Module2 Part1 ENDocument13 pagesECH Module2 Part1 ENHassanahmad445No ratings yet
- Using A LCA Approach To Estimate The Net GHG Emissions of BioenergyDocument20 pagesUsing A LCA Approach To Estimate The Net GHG Emissions of BioenergymohsinamanNo ratings yet
- Separations 08 00035 v2Document17 pagesSeparations 08 00035 v2Khánh Linh LêNo ratings yet
- Benefits of Future Clean Air Policies in Europe .5Document6 pagesBenefits of Future Clean Air Policies in Europe .5Khaled ChekroubaNo ratings yet
- Environmental Pollution: Lanyu Li, Aiming Yang, Xiaotao He, Jiangtao Liu, Yueling Ma, Jingping Niu, Bin LuoDocument9 pagesEnvironmental Pollution: Lanyu Li, Aiming Yang, Xiaotao He, Jiangtao Liu, Yueling Ma, Jingping Niu, Bin LuoMuhammad ImranNo ratings yet
- Articulo N°1 PDFDocument8 pagesArticulo N°1 PDFvaleriaNo ratings yet
- Global Mortality From Outdoor Fine Particle by FossilDocument8 pagesGlobal Mortality From Outdoor Fine Particle by FossilAHMAD BALFAQIHNo ratings yet
- Effect of Ventilation Strategies and Air Purifiers On The Children's Exposure To AirbornDocument10 pagesEffect of Ventilation Strategies and Air Purifiers On The Children's Exposure To AirbornMariaNo ratings yet
- Intercomparison of Methods To Estimate Black Carbon EmissionsDocument8 pagesIntercomparison of Methods To Estimate Black Carbon EmissionsJoy RoyNo ratings yet
- 00 Naeher 1Document6 pages00 Naeher 1puskesmasNo ratings yet
- 20230818CT01 Particles Size On Hepa FilterDocument9 pages20230818CT01 Particles Size On Hepa FilterMlx HoNo ratings yet
- Applied Mathematical ModellingDocument13 pagesApplied Mathematical ModellinghawNo ratings yet
- Importance of Transboundary Transport of Biomass BDocument11 pagesImportance of Transboundary Transport of Biomass Bdiljit nayakNo ratings yet
- Liu 2018Document11 pagesLiu 2018Jimmy NarvaezNo ratings yet
- Journal of Cereal Science: S. Serrano, F. Rincón, J. García-OlmoDocument6 pagesJournal of Cereal Science: S. Serrano, F. Rincón, J. García-OlmoGuisela Carbajal RomeroNo ratings yet
- COPD AsiapacificDocument8 pagesCOPD AsiapacificJan HatolNo ratings yet
- 1 s2.0 S001393512101389X MainDocument5 pages1 s2.0 S001393512101389X MainYusril Ihza TachririNo ratings yet
- Halios Etal (2009) STOTENDocument8 pagesHalios Etal (2009) STOTENChristosNo ratings yet
- Indoor Air Quality Index and Chronic Health DiseaseDocument5 pagesIndoor Air Quality Index and Chronic Health DiseaseesatjournalsNo ratings yet
- Atmospheric Pollution Research: Iman Parseh, Hakimeh Teiri, Yaghoub Hajizadeh, Karim EbrahimpourDocument5 pagesAtmospheric Pollution Research: Iman Parseh, Hakimeh Teiri, Yaghoub Hajizadeh, Karim EbrahimpourMaharghya BiswasNo ratings yet
- Lesson Plan - The V LanguageDocument4 pagesLesson Plan - The V LanguageLê Thị Ái NhiNo ratings yet
- PokeDex ChecklistDocument7 pagesPokeDex ChecklistJosh StrıkeNo ratings yet
- Surface Vehicle Standard: Rev. AUG1997Document6 pagesSurface Vehicle Standard: Rev. AUG1997anupthattaNo ratings yet
- Prosperity Power Signature PDFDocument31 pagesProsperity Power Signature PDFOscar NygrenNo ratings yet
- BLUE COLLAR JOBS Vs WHITE COLLAR JOBS.Document2 pagesBLUE COLLAR JOBS Vs WHITE COLLAR JOBS.Nelson VersozaNo ratings yet
- Er9000en 21204 1.00Document106 pagesEr9000en 21204 1.00Alexandru AnghelNo ratings yet
- Glenbard East Lesson PlanDocument8 pagesGlenbard East Lesson Planapi-608726850No ratings yet
- List of Engineering Colleges in PakistanDocument7 pagesList of Engineering Colleges in PakistanFahad Bin ImtiazNo ratings yet
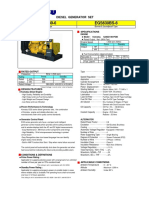
- Egs630-6 Komatsu GensetDocument2 pagesEgs630-6 Komatsu GensetimamfadiliNo ratings yet
- Ethics 5Document3 pagesEthics 5MANINGO, EDRIAN JAY M.No ratings yet
- MindmapDocument2 pagesMindmapapi-545246569No ratings yet
- Fredkin Introduction To Digital PhilosophyDocument59 pagesFredkin Introduction To Digital PhilosophyEdoardo MatteiNo ratings yet
- Annual Report Final 2017-18 enDocument232 pagesAnnual Report Final 2017-18 enNidhi DesaiNo ratings yet
- S1-1054/2 10kV Digital Insulation Tester: User ManualDocument24 pagesS1-1054/2 10kV Digital Insulation Tester: User ManualHoracio BobedaNo ratings yet
- Sogc AssignmentDocument2 pagesSogc Assignmentapi-573219210No ratings yet
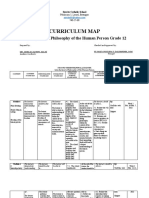
- Curriculum Map in Introduction To The World ReligionDocument7 pagesCurriculum Map in Introduction To The World ReligionRaizza Vanizza SiguenzaNo ratings yet
- MSA WorksheetDocument33 pagesMSA WorksheetSandrawarman BalasundramNo ratings yet
- Qualitative Study On Stress Among Nurses Working at Private Sector, in Suburban KolkataDocument9 pagesQualitative Study On Stress Among Nurses Working at Private Sector, in Suburban KolkataSandra RNo ratings yet
- Micro SplatDocument17 pagesMicro SplatCarlosAndresGarnicaSalazarNo ratings yet
- Aec3414 Philosophy FinalDocument5 pagesAec3414 Philosophy Finalapi-532996380No ratings yet
- List of ROs Under VODocument74 pagesList of ROs Under VOvivek mishraNo ratings yet
- 1000-211-V8-0000-01003 Concrete Works (Trial Mix)Document38 pages1000-211-V8-0000-01003 Concrete Works (Trial Mix)hodigojiggfjlgkdgiohghfdiohghjfNo ratings yet
- 04-68350A Manual CCN DM01-DI01 PDFDocument47 pages04-68350A Manual CCN DM01-DI01 PDFtaha50% (2)
- Conditions For Effective Innovation On The MacroDocument3 pagesConditions For Effective Innovation On The MacroWinesha U. Smith100% (2)
- Pallet Truck wp3000 Spec1 GBDocument6 pagesPallet Truck wp3000 Spec1 GBEjaz EjazNo ratings yet
- Qualities of A Good PresenterDocument2 pagesQualities of A Good PresenterMuhammad Umair KhanNo ratings yet
- Introduction To Discourse Analysis PDFDocument20 pagesIntroduction To Discourse Analysis PDFShobade Christianah Temitope100% (1)
- Inside The Social Network's (Datacenter) NetworkDocument49 pagesInside The Social Network's (Datacenter) NetworkVamsi Krishna PatchamatlaNo ratings yet
- A Simple Guide To Energy Budgets: Number 167 WWW - Curriculum-Press - Co.ukDocument4 pagesA Simple Guide To Energy Budgets: Number 167 WWW - Curriculum-Press - Co.ukKamaria ThomasNo ratings yet
- Long Quiz For Week 12345Document26 pagesLong Quiz For Week 12345Jerwyn Marie CayasNo ratings yet