You might also like
- Transforming Society: A Comprehensive Introduction to Understanding Trauma, Adversity, & Becoming a Trauma-Informed OrganisationFrom EverandTransforming Society: A Comprehensive Introduction to Understanding Trauma, Adversity, & Becoming a Trauma-Informed OrganisationNo ratings yet
- Trauma-Informed Care Resources For Leaders and ManagersDocument15 pagesTrauma-Informed Care Resources For Leaders and ManagersModi100% (1)
- Trauma-Informed Healthcare Approaches: A Guide for Primary CareFrom EverandTrauma-Informed Healthcare Approaches: A Guide for Primary CareMegan R. GerberNo ratings yet
- Best Practice & Research Clinical Anaesthesiology: Tanja Manser, PHD, Associate Professor SNSFDocument11 pagesBest Practice & Research Clinical Anaesthesiology: Tanja Manser, PHD, Associate Professor SNSFCristina Maria BostanNo ratings yet
- Point of Contact 0217 pp55 60Document6 pagesPoint of Contact 0217 pp55 60Rafi ramdhanNo ratings yet
- Trauma-Informed Abortion CareDocument5 pagesTrauma-Informed Abortion CareJohn BitsasNo ratings yet
- DRM Fact Sheet Safe HospitalsDocument3 pagesDRM Fact Sheet Safe HospitalsAnonymous dVcPCxF4eJNo ratings yet
- A-Trauma-Informed-Approach-to-Work 2024Document26 pagesA-Trauma-Informed-Approach-to-Work 2024hcintiland sbyNo ratings yet
- Fitzgerald Et Al 2017Document7 pagesFitzgerald Et Al 2017Aishi BaidyaNo ratings yet
- Addressing Burnout in Mental Health Nursing: Strategies, Challenges, and Future DirectionsDocument8 pagesAddressing Burnout in Mental Health Nursing: Strategies, Challenges, and Future DirectionseditorbijnrNo ratings yet
- The Goal of Disaster NursingDocument13 pagesThe Goal of Disaster NursingPrince Mark BadilloNo ratings yet
- Work Effectively in Trauma Informed CareDocument20 pagesWork Effectively in Trauma Informed CareCharlie HaddadNo ratings yet
- Trauma Informed Care in Medicine: Current Knowledge and Future Research DirectionsDocument11 pagesTrauma Informed Care in Medicine: Current Knowledge and Future Research DirectionsJohn BitsasNo ratings yet
- SAMHSA TraumaDocument29 pagesSAMHSA TraumaAna Paula V. CardosoNo ratings yet
- Nurses Role During A DisasterDocument4 pagesNurses Role During A DisasterNaomi RebongNo ratings yet
- Managing Traumatic Stress in The Workplace: EditorialDocument3 pagesManaging Traumatic Stress in The Workplace: EditorialSharifah suuNo ratings yet
- Barriers and Enablers For The Implementation of TRDocument21 pagesBarriers and Enablers For The Implementation of TRashlyn granthamNo ratings yet
- Developing A Trauma-Informed Child Welfare SystemDocument9 pagesDeveloping A Trauma-Informed Child Welfare SystemKeii blackhoodNo ratings yet
- Trauma Informed CareDocument8 pagesTrauma Informed CareJohn BitsasNo ratings yet
- Disaster PrepardnessDocument11 pagesDisaster Prepardnesssamantha harrynananNo ratings yet
- MentalIllnessPrevention 7-7-14 FORMATDocument4 pagesMentalIllnessPrevention 7-7-14 FORMATPrernaNo ratings yet
- Patient Safety: What About The Patient?: Consumers' ViewDocument5 pagesPatient Safety: What About The Patient?: Consumers' Viewujangketul62No ratings yet
- Trauma-Informed Social Work Practice: Jill LevensonDocument9 pagesTrauma-Informed Social Work Practice: Jill LevensonIvy WangNo ratings yet
- Safeguarding Incident ArticleDocument8 pagesSafeguarding Incident ArticleNimra JamilNo ratings yet
- NCM 113 Mod1Document6 pagesNCM 113 Mod1Samantha BolanteNo ratings yet
- (N20S) - Advocacy, Empowerment and SafeguardingDocument9 pages(N20S) - Advocacy, Empowerment and SafeguardingNimra JamilNo ratings yet
- 14 Supporting Prevention and Chronic Condition Self-ManagementDocument8 pages14 Supporting Prevention and Chronic Condition Self-Managementilham apriadiNo ratings yet
- Roles of Health Care Providers in Sto. Niño Health Center: Fire Disaster PreparednessDocument24 pagesRoles of Health Care Providers in Sto. Niño Health Center: Fire Disaster PreparednessOoLvs XibNo ratings yet
- Assignment 3, Anaisha Rachel Paul, RSCH-6032Document7 pagesAssignment 3, Anaisha Rachel Paul, RSCH-6032winchester218paulNo ratings yet
- CHN Module 1Document34 pagesCHN Module 1Don Maur ValeteNo ratings yet
- Community Health Nursing 1 NCM 104Document4 pagesCommunity Health Nursing 1 NCM 104Sheila May Teope Santos100% (1)
- An Institutional Model For Health Care WDocument18 pagesAn Institutional Model For Health Care WlokNo ratings yet
- Abstract The History and Principles of Trauma-Informed Practice in Social WorkDocument20 pagesAbstract The History and Principles of Trauma-Informed Practice in Social WorkHany A Aziz100% (1)
- Jama 2009 1384Document10 pagesJama 2009 1384Katherine ChicasNo ratings yet
- Disaster Mental Health PDFDocument85 pagesDisaster Mental Health PDFNicole Rachelyn MartinNo ratings yet
- Emergency Health Education and Communication: A Primer For Health EducatorsDocument4 pagesEmergency Health Education and Communication: A Primer For Health EducatorsJJoliat100% (1)
- Disaster Nursing - Icn Position and Recommendation - Rotone, Lycah v. - BSN 4yb-4Document3 pagesDisaster Nursing - Icn Position and Recommendation - Rotone, Lycah v. - BSN 4yb-4Lycah RotoneNo ratings yet
- Crisis Intervention ServicesDocument3 pagesCrisis Intervention ServicespysarchukludmylaNo ratings yet
- ICN Framework of Disaster Nursing CompetenciesDocument27 pagesICN Framework of Disaster Nursing CompetenciesChannelG100% (1)
- Morrison, 2010Document11 pagesMorrison, 2010Jbl2328No ratings yet
- Critical Incident Management ArticleDocument11 pagesCritical Incident Management ArticleNimra JamilNo ratings yet
- Crisis Intervention SummaryDocument7 pagesCrisis Intervention Summarydennis8113100% (2)
- Guide To Harm Reduction ManualDocument39 pagesGuide To Harm Reduction ManualRaquelNo ratings yet
- Running Head: Mental Health and Nursing PracticesDocument7 pagesRunning Head: Mental Health and Nursing PracticesRamizNo ratings yet
- De-Escalation in Health Care. Quick Safety. The Joint Commission, Division of Healthcare Improvement Issue 47 - January 2019Document4 pagesDe-Escalation in Health Care. Quick Safety. The Joint Commission, Division of Healthcare Improvement Issue 47 - January 2019Urgencias HorwitzNo ratings yet
- The Critical Role of Clinical Social Work in Case ManagementDocument2 pagesThe Critical Role of Clinical Social Work in Case Managementacma2010No ratings yet
- Crisis InterventionsDocument6 pagesCrisis InterventionsNilsa RoblesNo ratings yet
- Betty Neuman Framework Breast CancerDocument10 pagesBetty Neuman Framework Breast CancerConnie SianiparNo ratings yet
- Problem-Based ResearchDocument8 pagesProblem-Based Researchapi-480618512No ratings yet
- Disaster Plan - EditedDocument5 pagesDisaster Plan - EditedPoetic YatchyNo ratings yet
- R PaperDocument15 pagesR Paper78fhscpyt5No ratings yet
- Thesis - Prevention of Nosocomial Infections As Percieved by Staff NursesDocument31 pagesThesis - Prevention of Nosocomial Infections As Percieved by Staff NursesShine Lyn92% (12)
- Fpsyg 14 1145100Document12 pagesFpsyg 14 1145100Abigail MJNo ratings yet
- Briere ITCT-A Final PDFDocument119 pagesBriere ITCT-A Final PDFDave HenehanNo ratings yet
- Figure 1. Disaster Management Continuum: Prevention/MitigationDocument4 pagesFigure 1. Disaster Management Continuum: Prevention/MitigationSovia fitriaNo ratings yet
- Session 4 - Talking With Other Health Professionals - EnglishDocument1 pageSession 4 - Talking With Other Health Professionals - EnglishMaria GarabajiuNo ratings yet
- Post-Impact-RecoveryDocument15 pagesPost-Impact-Recoveryaisa baladjiNo ratings yet
- Mieliu TherapyDocument7 pagesMieliu TherapyRENJULALNo ratings yet
- What Are The "Features of Community Health Nursing"? Provide Definitions and ExamplesDocument2 pagesWhat Are The "Features of Community Health Nursing"? Provide Definitions and ExamplesEmeli Pis-ing Pang-esNo ratings yet
- Right Care 3. Drivers of Poor Medical CareDocument13 pagesRight Care 3. Drivers of Poor Medical CareJuan Jose Eraso OsorioNo ratings yet
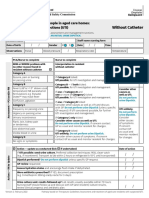
- Form Ams Clinical Pathway Fillable Form Without CatheterDocument1 pageForm Ams Clinical Pathway Fillable Form Without CatheterTeenu JobyNo ratings yet
- Trauma 2020Document25 pagesTrauma 2020K MNo ratings yet
- Elearning BLS Tutorial Version 9 - Dec 2016 - ACN Approved Feb 2016 PDFDocument29 pagesElearning BLS Tutorial Version 9 - Dec 2016 - ACN Approved Feb 2016 PDFgilangNo ratings yet
- NSW Acute Coronary Stenosis (STEMI/NSTEMI) ProtocolDocument16 pagesNSW Acute Coronary Stenosis (STEMI/NSTEMI) ProtocolFaraz MahboobNo ratings yet
- Hackmann 2011 Imagery Rescripting in PTSDDocument9 pagesHackmann 2011 Imagery Rescripting in PTSDAna FerreiraNo ratings yet
- The Mindfulness and Acceptance Workbook For Anxiety - A Guide To Breaking Free From Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy (PDFDrive)Document231 pagesThe Mindfulness and Acceptance Workbook For Anxiety - A Guide To Breaking Free From Anxiety, Phobias, and Worry Using Acceptance and Commitment Therapy (PDFDrive)Adriana fernandesNo ratings yet
- PTSD Lesson PlanDocument8 pagesPTSD Lesson Plansp2056251No ratings yet
- Mental Health Apps and SitesDocument5 pagesMental Health Apps and Sites10News WTSPNo ratings yet
- Breathing Retraining in PTSD A Practical ExerciseDocument16 pagesBreathing Retraining in PTSD A Practical ExerciseRyan DouglasNo ratings yet
- Cusack Et Al. (2016)Document54 pagesCusack Et Al. (2016)jehonol883No ratings yet
- PTSDDocument41 pagesPTSDnersrensi89gmailcomNo ratings yet
- Glickman Et Al., 2017Document13 pagesGlickman Et Al., 2017tania0308No ratings yet
- Using the PTSD Checklist for DSM-5 (PCL-5Document5 pagesUsing the PTSD Checklist for DSM-5 (PCL-5Lorena Teodora Cazacu100% (1)
- Perrotta Psychological Trauma DefinitionDocument7 pagesPerrotta Psychological Trauma DefinitionHvovi BhagwagarNo ratings yet
- CBT17 - Exposure and Response Prevention - Fall 2020Document211 pagesCBT17 - Exposure and Response Prevention - Fall 2020Natalia Ramirez100% (1)
- Treating The Trauma of Rape CBT For PTSDDocument6 pagesTreating The Trauma of Rape CBT For PTSDJulianaNo ratings yet
- Chapter 5: Stress and Physical and Mental HealthDocument9 pagesChapter 5: Stress and Physical and Mental HealthJuliet Anne Buangin Alo100% (1)
- Prolonged Exposure Therapy - Past, Present, and FutureDocument5 pagesProlonged Exposure Therapy - Past, Present, and FutureKelly GCNo ratings yet
- Prolonged Exposure Sessions With 20-MinuteDocument11 pagesProlonged Exposure Sessions With 20-MinutejlbermudezcNo ratings yet
- Treatment of Acute Stress DisorderDocument11 pagesTreatment of Acute Stress DisorderKusnanto Penasehat Kpb RyusakiNo ratings yet
- Evidence-Based Psychotherapy Interventions To Improve Psychosocial Functioning in Veterans With PTSDDocument10 pagesEvidence-Based Psychotherapy Interventions To Improve Psychosocial Functioning in Veterans With PTSDM SalNo ratings yet
- Beyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDDocument9 pagesBeyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDmakolla007No ratings yet
- Childhood Trauma and Psychosis Link Updated ReviewDocument15 pagesChildhood Trauma and Psychosis Link Updated ReviewDaniel Cossío MiravallesNo ratings yet
- Managing Psychological ProblemsDocument2 pagesManaging Psychological ProblemsAdrian LagascaNo ratings yet
- Trauma-Focused Treatment For Comorbid Post-Traumatic Stress and Substance Use DisorderDocument16 pagesTrauma-Focused Treatment For Comorbid Post-Traumatic Stress and Substance Use DisorderalejandraNo ratings yet
- Anxiety Therapy Types, Techniques, and WorksheetsDocument29 pagesAnxiety Therapy Types, Techniques, and WorksheetsGilang Faisal AndrianNo ratings yet
- Post-Traumatic Stress Disorder (PTSD) - Social Work - Oxford BibliographiesDocument6 pagesPost-Traumatic Stress Disorder (PTSD) - Social Work - Oxford BibliographiesmentamentaNo ratings yet
- The PTSD Behavioral Activation Workbook Activities To Help You Rebuild Your Life From Post-Traumatic Stress DisorderDocument213 pagesThe PTSD Behavioral Activation Workbook Activities To Help You Rebuild Your Life From Post-Traumatic Stress DisorderMaría Alejandra Pérez100% (3)
- Reclaiming Your Life From A Traumatic Experience: Workbook - Rothbaum, Edna B. Foa, HembreeDocument105 pagesReclaiming Your Life From A Traumatic Experience: Workbook - Rothbaum, Edna B. Foa, Hembreedoppler_100% (8)
- Cognitive Processing Therapy For Sexual Assault Victims.Document9 pagesCognitive Processing Therapy For Sexual Assault Victims.CripolizerNo ratings yet
- Prolonged Exposure Therapy For PTSD: Emotional Processing of Traumatic Experiences, Therapist Guide - Edna B. FoaDocument151 pagesProlonged Exposure Therapy For PTSD: Emotional Processing of Traumatic Experiences, Therapist Guide - Edna B. Foadoppler_100% (10)
- Schema Therapy For Dissociative Identity Disorder DID Further ExplanationDocument4 pagesSchema Therapy For Dissociative Identity Disorder DID Further ExplanationCarolina ValenciaNo ratings yet
- Treating PTSD in the Middle EastDocument4 pagesTreating PTSD in the Middle Eastsyeda salmaNo ratings yet
- Complex PTSDDocument29 pagesComplex PTSDLia VágvölgyiNo ratings yet
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerFrom EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerRating: 4.5 out of 5 stars4.5/5 (16)
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)
- Triggers: How We Can Stop Reacting and Start HealingFrom EverandTriggers: How We Can Stop Reacting and Start HealingRating: 5 out of 5 stars5/5 (58)
- Embrace Your Weird: Face Your Fears and Unleash CreativityFrom EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityRating: 4.5 out of 5 stars4.5/5 (124)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- The Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.From EverandThe Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.Rating: 5 out of 5 stars5/5 (14)