You might also like
- Oral Board Review For Oral and Maxillofacial Surgery, Robert - RetiDocument550 pagesOral Board Review For Oral and Maxillofacial Surgery, Robert - RetiMd Shoton100% (4)
- Drugs Used For Blood Coagulation Disorders - KatzungDocument3 pagesDrugs Used For Blood Coagulation Disorders - Katzungsarguss14100% (6)
- Drug-Lab Test Interaction - Full PDFDocument9 pagesDrug-Lab Test Interaction - Full PDFmanikNo ratings yet
- MLS ASCPi Exam Content Guidlines 2019Document12 pagesMLS ASCPi Exam Content Guidlines 2019Islam100% (2)
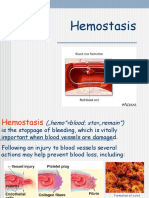
- HomeostasisDocument8 pagesHomeostasisLely SharmaNo ratings yet
- Coagulants and Anti CoagulantsDocument22 pagesCoagulants and Anti Coagulantsdhainey100% (2)
- Kastur IDocument38 pagesKastur IKasturi MohantyNo ratings yet
- Blood Biochemistry 2 (2021)Document29 pagesBlood Biochemistry 2 (2021)anis izzatiNo ratings yet
- Hemostasis: Rahajuningsih D. Setiabudy Department of Clinical Pathology Faculty of Medicine University of IndonesiaDocument37 pagesHemostasis: Rahajuningsih D. Setiabudy Department of Clinical Pathology Faculty of Medicine University of IndonesiastellatrsNo ratings yet
- Proses Hemostasis KULDocument46 pagesProses Hemostasis KULSuryana AdityaNo ratings yet
- Antithormbotics 2020Document34 pagesAntithormbotics 2020Kawther HussainNo ratings yet
- Coagulation in PregnancyDocument14 pagesCoagulation in PregnancyYorim Sora PasilaNo ratings yet
- Clinical Pathway of HemostasisDocument42 pagesClinical Pathway of HemostasisDhiaul Izzah RamadhaniNo ratings yet
- Hemostatic Physiology: Mansyur Arif Dept. of Clinical Pathology Faculty of Medicine, Hasanuddin University, MakassarDocument67 pagesHemostatic Physiology: Mansyur Arif Dept. of Clinical Pathology Faculty of Medicine, Hasanuddin University, Makassarnurliah armandNo ratings yet
- 3-17-08 Whitehill PDFDocument47 pages3-17-08 Whitehill PDFSindile MchunuNo ratings yet
- Bleeding and HemostasisDocument24 pagesBleeding and HemostasisMohamed Saeed BachooNo ratings yet
- Warfarin's mechanism of action and indicationsDocument4 pagesWarfarin's mechanism of action and indicationsAmir mohammad moori MohammadiNo ratings yet
- Hemostasis and Coagulation: Miklós MolnárDocument67 pagesHemostasis and Coagulation: Miklós MolnárHamzaNo ratings yet
- Blood Faed Haemostasis 3 Coagulation Tests Intro To Bleeding Disorders Full PDFDocument46 pagesBlood Faed Haemostasis 3 Coagulation Tests Intro To Bleeding Disorders Full PDFAsh KumarNo ratings yet
- Blood Thinners: Hussein Hallak, PH.DDocument68 pagesBlood Thinners: Hussein Hallak, PH.DIbrahim BarhamNo ratings yet
- Mekanisme Hemostasis & Koagulasi (Prof. Dr. Mansyur Arif, PH.D, SP - PK (K) )Document55 pagesMekanisme Hemostasis & Koagulasi (Prof. Dr. Mansyur Arif, PH.D, SP - PK (K) )ikram hanafiNo ratings yet
- Anticoagulant: Mechanism and ReverseDocument22 pagesAnticoagulant: Mechanism and ReverseNovi Riyadhah Ma'sumNo ratings yet
- Hemostasis and Thrombosis in ESRDDocument36 pagesHemostasis and Thrombosis in ESRDRam Dayal VishwakarmaNo ratings yet
- Tripathy - Summary of Drugs Affecting Blood and Blood FormationDocument33 pagesTripathy - Summary of Drugs Affecting Blood and Blood FormationSumi FaNo ratings yet
- Lecture 19 - AnticoagulantsDocument43 pagesLecture 19 - Anticoagulantsapi-3703352100% (1)
- HEMORRHAGIC DIATHESES: ASPECTS OF CLINICAL AND LABORATORY DIAGNOSIS AND TREATMENT PRINCIPLESDocument90 pagesHEMORRHAGIC DIATHESES: ASPECTS OF CLINICAL AND LABORATORY DIAGNOSIS AND TREATMENT PRINCIPLESNatalia MinzatuNo ratings yet
- 028 - Cardiovascular Pharmacology) Heparin - Mechanism of Action, Indications, ADRâ ™S, ContraindicationsDocument5 pages028 - Cardiovascular Pharmacology) Heparin - Mechanism of Action, Indications, ADRâ ™S, ContraindicationsOliver Jacobe100% (1)
- CoagulationDocument44 pagesCoagulationJoan FernandezNo ratings yet
- The Effects of Pituitary and Thyroid Disorders On Haemostasis, Potential Clinical ImplicationsDocument12 pagesThe Effects of Pituitary and Thyroid Disorders On Haemostasis, Potential Clinical ImplicationsTamara Silva FabresNo ratings yet
- Blood Clotting CascadeDocument10 pagesBlood Clotting CascadeshravaniNo ratings yet
- Blood Clotting Cascade OverviewDocument44 pagesBlood Clotting Cascade OverviewMAWEJJE OSTEENNo ratings yet
- Understanding Laboratory Tests for Hemostasis FunctionDocument46 pagesUnderstanding Laboratory Tests for Hemostasis FunctionGranitaNo ratings yet
- Blood Clotting CascadeDocument10 pagesBlood Clotting CascadeBiniyam AsratNo ratings yet
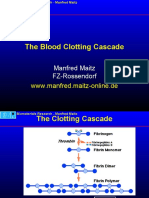
- The Blood Clotting Cascade: WWW - Manfred.maitz-Online - deDocument10 pagesThe Blood Clotting Cascade: WWW - Manfred.maitz-Online - desam16231No ratings yet
- Blood Clotting CascadeDocument10 pagesBlood Clotting CascadeLorato MmolawaNo ratings yet
- Blood Coagulation: Extrinsic and Intrinsic PathwayDocument13 pagesBlood Coagulation: Extrinsic and Intrinsic PathwayChaitanya KumarNo ratings yet
- Manfred Maitz's Research on the Blood Clotting CascadeDocument10 pagesManfred Maitz's Research on the Blood Clotting CascadeFitriyana WinarnoNo ratings yet
- OASIS 5 Prof Harmani Mercure 5 Feb 06Document55 pagesOASIS 5 Prof Harmani Mercure 5 Feb 06M Azmi HNo ratings yet
- Pharmacology Monitoring Medication LevelsDocument8 pagesPharmacology Monitoring Medication LevelsThierd Cañete III100% (1)
- Blood Coagulation SystemDocument46 pagesBlood Coagulation SystemFedrik Monte Kristo LimbongNo ratings yet
- Alteraciones de la hemostasia en el recién nacidoDocument59 pagesAlteraciones de la hemostasia en el recién nacidoUlises VillanuevaNo ratings yet
- Obat Sistem HematologiDocument21 pagesObat Sistem HematologiSuryana AdityaNo ratings yet
- Hemostasis Dan Koagulasi: DR - Fedelia Raya, M.Kes, SPPK Bagian Patologi Klinik Fk-UhoDocument18 pagesHemostasis Dan Koagulasi: DR - Fedelia Raya, M.Kes, SPPK Bagian Patologi Klinik Fk-UhoToraoNo ratings yet
- Disseminated Intravascular CoagulationDocument37 pagesDisseminated Intravascular Coagulationisrofah100% (1)
- ToxicologyDocument7 pagesToxicologysaadalotaibi31No ratings yet
- Chapter 4. Physiology of HemostasisDocument2 pagesChapter 4. Physiology of HemostasisDumapis RichardNo ratings yet
- Anticoagulant Drug Suvo (Fhami Mam-Pharmacology Lab)Document4 pagesAnticoagulant Drug Suvo (Fhami Mam-Pharmacology Lab)Ashaduzzaman suvoNo ratings yet
- Coag 2Document13 pagesCoag 2Tekkie TamNo ratings yet
- AntiarrhythmiaDocument29 pagesAntiarrhythmiaDRx Raju ChandranNo ratings yet
- NON Malig HaemDocument49 pagesNON Malig HaemNisini ImanyaNo ratings yet
- L8 Anti Coagulant DrugsDocument10 pagesL8 Anti Coagulant DrugsamanabduwahabNo ratings yet
- 21 - Anticoagulative DrugsDocument62 pages21 - Anticoagulative Drugsmashe1No ratings yet
- Anti CoagulantsDocument25 pagesAnti Coagulantsshoaib106muhammadNo ratings yet
- April 28 FibrinolysisDocument7 pagesApril 28 FibrinolysisCzarina Mae IlaganNo ratings yet
- Plasma Fractionation and Viral Inactivation/removal ProceduresDocument52 pagesPlasma Fractionation and Viral Inactivation/removal ProceduresMuhammad Ahmed MirzaNo ratings yet
- Lecture HemostasisDocument28 pagesLecture HemostasisЛариса ТкачеваNo ratings yet
- Aspek Laboratorium Kelainan HemostasisDocument48 pagesAspek Laboratorium Kelainan HemostasisriskypiradeNo ratings yet
- Fibrinolytic and Anticoag NotesDocument2 pagesFibrinolytic and Anticoag Notesrizz baternaNo ratings yet
- Bleeding Disorders by Dr. Sharad JohriDocument41 pagesBleeding Disorders by Dr. Sharad JohriShashwat JohriNo ratings yet
- HemostasisDocument36 pagesHemostasisPutri Rara BalernaPratiwiNo ratings yet
- Technothrombin TGA Triggers ML-00-00293REV01Document8 pagesTechnothrombin TGA Triggers ML-00-00293REV01myafiaNo ratings yet
- Coagulation Disorders-First Aid Book: SS DX TXDocument6 pagesCoagulation Disorders-First Aid Book: SS DX TXMAINo ratings yet
- PhysiologicDocument50 pagesPhysiologicRochelle Joyce AradoNo ratings yet
- Prevention & Treatment Prevention & Treatment: Thromboembolism ThromboembolismDocument64 pagesPrevention & Treatment Prevention & Treatment: Thromboembolism ThromboembolismrihuiNo ratings yet
- Nursing Care of a Child with HemophiliaDocument53 pagesNursing Care of a Child with HemophiliaDay Meds100% (1)
- Huether: Understanding Pathophysiology, 6th EditionDocument4 pagesHuether: Understanding Pathophysiology, 6th EditionTecsh DeckgirlNo ratings yet
- Bleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderDocument5 pagesBleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderAyisha EdwinNo ratings yet
- ThrombophiliaDocument37 pagesThrombophiliaapi-272740672No ratings yet
- Abram Study NotesDocument6 pagesAbram Study Notesteeman2No ratings yet
- Analyte Stability & Freeze-Thaw Information-1Document8 pagesAnalyte Stability & Freeze-Thaw Information-1Yusuf Indra SentosaNo ratings yet
- Genetice Disorders: Genetic Disorder Is A Disease or Disorder Caused by Damage or Change and Mutation On Individual's DNADocument46 pagesGenetice Disorders: Genetic Disorder Is A Disease or Disorder Caused by Damage or Change and Mutation On Individual's DNAAna Subol AñonuevoNo ratings yet
- Chapter 1 Overview of IsDocument35 pagesChapter 1 Overview of IsNathalie PortugalNo ratings yet
- April 28 FibrinolysisDocument7 pagesApril 28 FibrinolysisCzarina Mae IlaganNo ratings yet
- Covid19 HypercoagulabilityDocument22 pagesCovid19 Hypercoagulability陳瑞豐No ratings yet
- Order of DrawDocument8 pagesOrder of DrawVincent ReyesNo ratings yet
- Learning Outcome 1 Learning Outcome 2: (Osborn) Chapter 63 Learning Outcomes (Number and Title)Document19 pagesLearning Outcome 1 Learning Outcome 2: (Osborn) Chapter 63 Learning Outcomes (Number and Title)KittiesNo ratings yet
- Human Physiology BMLTDocument1 pageHuman Physiology BMLTGaurav SinghNo ratings yet
- Proteins, Platelets, and Coagulation at Biomaterial InterfacesDocument54 pagesProteins, Platelets, and Coagulation at Biomaterial InterfacesLUCERONo ratings yet
- Section VI: Flash Cards by Seetal K. Dhaliwal H. SDocument25 pagesSection VI: Flash Cards by Seetal K. Dhaliwal H. SmohamedadnanNo ratings yet
- Polytrauma Jacques Duranteau PDFDocument48 pagesPolytrauma Jacques Duranteau PDFMarcelo MercadoNo ratings yet
- Thrombolytic Therapy For Ischemic StrokeDocument7 pagesThrombolytic Therapy For Ischemic StrokechandradwtrNo ratings yet
- Pathology - Chapter 14Document14 pagesPathology - Chapter 14Cory GrayNo ratings yet
- NP1 NotesDocument59 pagesNP1 NotesBrianMarBeltranNo ratings yet
- Pengantar HemostasisDocument12 pagesPengantar HemostasisPretty AngeliaNo ratings yet
- Hematopoietic SystemDocument39 pagesHematopoietic SystemapplesncoreNo ratings yet
- Anticoagulants DrugsDocument6 pagesAnticoagulants DrugsHusam Al-OdatNo ratings yet
- HaematologyDocument11 pagesHaematologyIkram AzmanNo ratings yet
- Hema Rotation Quiz 2Document5 pagesHema Rotation Quiz 2Maxine AraralNo ratings yet
- Ceveron Alpha Brochure ML-00-00057REV03Document4 pagesCeveron Alpha Brochure ML-00-00057REV03Smithesh TpNo ratings yet