You might also like
- Social Case Study ReportDocument2 pagesSocial Case Study ReportKaren Laurin92% (12)
- Universal Health Care Implementers Project - GuidelinesDocument3 pagesUniversal Health Care Implementers Project - GuidelinesErnest Jerome Malamion0% (3)
- Scrub and Circulating Practitioner Simulation Script - Salimbagat, UsmanDocument12 pagesScrub and Circulating Practitioner Simulation Script - Salimbagat, UsmanChristine Pialan SalimbagatNo ratings yet
- Test Bank Advanced Health Assessment Clinical Diagnosis in Primary Care 6th Edition DainsDocument4 pagesTest Bank Advanced Health Assessment Clinical Diagnosis in Primary Care 6th Edition DainsCarlton Caughey100% (37)
- CDC 116484 DS1Document14 pagesCDC 116484 DS1Adnan WasimNo ratings yet
- Mihu 2015Document7 pagesMihu 2015Nuryasni NuryasniNo ratings yet
- WatermarkDocument7 pagesWatermarkAna AdamNo ratings yet
- 1642 Full PDFDocument5 pages1642 Full PDFAriana FlemingNo ratings yet
- Fracture of The Clavicle in The Newborn Following Normal Labor and DeliveryDocument6 pagesFracture of The Clavicle in The Newborn Following Normal Labor and DeliveryAlberto OrtizNo ratings yet
- Al Riyami-2020-Respiratory Distress Syndrome IDocument6 pagesAl Riyami-2020-Respiratory Distress Syndrome IHidayatt NurulNo ratings yet
- A 23-Year, Single-Center, Retrospective Analysis of 36 Cases of AcuteDocument4 pagesA 23-Year, Single-Center, Retrospective Analysis of 36 Cases of AcuteAleGrNo ratings yet
- Paper Cervical LenghtDocument30 pagesPaper Cervical LenghtDanTe D' WinchesterNo ratings yet
- Oral Plenary I: Study DesignDocument2 pagesOral Plenary I: Study DesignLestari LifaNo ratings yet
- Fetomaternal Outcome and Raised Bilirubin Level in PregnancyDocument4 pagesFetomaternal Outcome and Raised Bilirubin Level in PregnancyPrima Hari PratamaNo ratings yet
- Jean-Charles Pasquier, Olivier Claris, Muriel Rabilloud, René Ecochard, Jean-Charles Picaud, Stéphanie Moret, Danielle Buch, Georges MellierDocument8 pagesJean-Charles Pasquier, Olivier Claris, Muriel Rabilloud, René Ecochard, Jean-Charles Picaud, Stéphanie Moret, Danielle Buch, Georges Mellierclara giovaniNo ratings yet
- Asociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Document8 pagesAsociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Andrés Gaviria CNo ratings yet
- Liu 2020Document6 pagesLiu 2020Vanessa CarinoNo ratings yet
- Association of High Sensitivity C Reactive Protein Serum LevelsDocument5 pagesAssociation of High Sensitivity C Reactive Protein Serum LevelsJesslynBernadetteNo ratings yet
- Articulos Sepsis Neonatal TempranaDocument29 pagesArticulos Sepsis Neonatal Tempranaverock88No ratings yet
- Preterm Premature Rupture of Membranes in The Presence of Cerclage: Is The Risk For Intra-Uterine Infection and Adverse Neonatal Outcome Increased?Document6 pagesPreterm Premature Rupture of Membranes in The Presence of Cerclage: Is The Risk For Intra-Uterine Infection and Adverse Neonatal Outcome Increased?stephaniedianNo ratings yet
- Journal Gyn KETDocument8 pagesJournal Gyn KETImaylani S. SitanggangNo ratings yet
- PIIS2210778916303701Document2 pagesPIIS2210778916303701Fatimah AssagafNo ratings yet
- Screening For Fetal Growth Restriction Using Ultrasound and The Sflt1/Plgf Ratio in Nulliparous Women: A Prospective Cohort StudyDocument13 pagesScreening For Fetal Growth Restriction Using Ultrasound and The Sflt1/Plgf Ratio in Nulliparous Women: A Prospective Cohort StudynicolasdlcaNo ratings yet
- Expectant Versus Aggressive Management in Severe Preeclampsia Remote From TermDocument6 pagesExpectant Versus Aggressive Management in Severe Preeclampsia Remote From Termmiss.JEJENo ratings yet
- The American Journal of Surgery: J. Quinn Gentles, Gabriela Meglei, Leo Chen, Cameron J. Hague, Adrienne L. MelckDocument5 pagesThe American Journal of Surgery: J. Quinn Gentles, Gabriela Meglei, Leo Chen, Cameron J. Hague, Adrienne L. Melcksuyudi kimikoNo ratings yet
- Jurnal Obgyn AstiDocument5 pagesJurnal Obgyn AstiadelialuthfiNo ratings yet
- Deng 2012Document4 pagesDeng 2012Rachmad RasidinNo ratings yet
- Neonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporeDocument7 pagesNeonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporePremier PublishersNo ratings yet
- Natural History of Fetal Position During Pregnancy.11Document6 pagesNatural History of Fetal Position During Pregnancy.11PutriNo ratings yet
- PIIS0002937820311923Document3 pagesPIIS0002937820311923FebbyNo ratings yet
- Evaluation of Serum Lipids in Preeclampsia: A Comparative StudyDocument4 pagesEvaluation of Serum Lipids in Preeclampsia: A Comparative StudyGladys SusantyNo ratings yet
- Elective Delivery Versus Expectant Management For Pre-Eclampsia: A Meta-Analysis of RctsDocument16 pagesElective Delivery Versus Expectant Management For Pre-Eclampsia: A Meta-Analysis of RctsErliana Damayanti100% (1)
- Bakker 2012Document10 pagesBakker 2012ieoNo ratings yet
- BMJ f6398Document13 pagesBMJ f6398Luis Gerardo Pérez CastroNo ratings yet
- Maternal and Obstetric Outcome of Women With Epilepsy 2009 SeizureDocument4 pagesMaternal and Obstetric Outcome of Women With Epilepsy 2009 Seizurebilal hadiNo ratings yet
- Pre-Eclampsia, Eclampsia and Adverse Maternal and Perinatal Outcomes: A Secondary Analysis of The World Health Organization Multicountry Survey On Maternal and Newborn HealthDocument11 pagesPre-Eclampsia, Eclampsia and Adverse Maternal and Perinatal Outcomes: A Secondary Analysis of The World Health Organization Multicountry Survey On Maternal and Newborn HealthMariana CruzNo ratings yet
- Ectopic Pregnancy Risk Factors, Clinical Presentation and ManagementDocument6 pagesEctopic Pregnancy Risk Factors, Clinical Presentation and ManagementRizka AdiNo ratings yet
- Post Partum Maternal Morbidities and TheDocument102 pagesPost Partum Maternal Morbidities and TheBagusHibridaNo ratings yet
- Insidence of Fever in Labor and Risk of Neonatal SepsisDocument5 pagesInsidence of Fever in Labor and Risk of Neonatal SepsisSNFauziaNo ratings yet
- The NeoUpdates - DecDocument7 pagesThe NeoUpdates - DecDr Satish MishraNo ratings yet
- Pregnancy With Epilepsy - A Retrospective Analysis: Gynetology & ObstetricsDocument6 pagesPregnancy With Epilepsy - A Retrospective Analysis: Gynetology & ObstetricsDwi Rofiqoh FauzahNo ratings yet
- Safety of Acupuncture During Pregnancy: A Retrospective Cohort Study in KoreaDocument8 pagesSafety of Acupuncture During Pregnancy: A Retrospective Cohort Study in Koreaindra coolNo ratings yet
- Tugas Kelompok Kegawatdaruratan (Pre-Eklamsi)Document6 pagesTugas Kelompok Kegawatdaruratan (Pre-Eklamsi)FeniNo ratings yet
- ANS Before 24 WeeksDocument11 pagesANS Before 24 WeeksmadhuNo ratings yet
- Research ArticleDocument6 pagesResearch Articlesufiah istthyNo ratings yet
- 4891 GlobalWarmingImpactsDocument14 pages4891 GlobalWarmingImpactsEdilenaNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarNo ratings yet
- Vol9 Issue1 06Document4 pagesVol9 Issue1 06annisaNo ratings yet
- Merced 2019Document14 pagesMerced 2019Vanessa CarinoNo ratings yet
- US en EndometritisDocument7 pagesUS en EndometritisRubí FuerteNo ratings yet
- Article NeonatesDocument7 pagesArticle NeonatesFaisal YousafNo ratings yet
- Singleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalDocument6 pagesSingleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalSarah SilaenNo ratings yet
- Pregnancy Induced SLE, 2017Document7 pagesPregnancy Induced SLE, 2017Maria GarabajiuNo ratings yet
- MJCU Volume 86 Issue December Pages 4259-4265Document7 pagesMJCU Volume 86 Issue December Pages 4259-4265SamarNo ratings yet
- Journal Ectopic Pregnancy-A Rising TrendDocument5 pagesJournal Ectopic Pregnancy-A Rising TrendEricNo ratings yet
- DownloadDocument6 pagesDownloadKai GgNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundHartanto LieNo ratings yet
- Antenatal Corticosteroids: An Assessment of Anticipated Benefits and Potential RisksDocument13 pagesAntenatal Corticosteroids: An Assessment of Anticipated Benefits and Potential RiskssaryindrianyNo ratings yet
- Leitich, 2003 Antibiotico No Tratamento de VB Meta AnaliseDocument7 pagesLeitich, 2003 Antibiotico No Tratamento de VB Meta AnaliseEdgar SimmonsNo ratings yet
- Bacterial Vaginosis Jurnal ReadingDocument27 pagesBacterial Vaginosis Jurnal ReadingWahyu Permata LisaNo ratings yet
- Pregnancy HypertensionDocument9 pagesPregnancy Hypertensionabi tehNo ratings yet
- Khair-Un-Nisa FormattedDocument4 pagesKhair-Un-Nisa FormattedMominah MayamNo ratings yet
- Cervical Stitch (Cerclage) For Preventing Pregnancy Loss: Individual Patient Data Meta-AnalysisDocument17 pagesCervical Stitch (Cerclage) For Preventing Pregnancy Loss: Individual Patient Data Meta-AnalysisNi Wayan Ana PsNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- NP 1 Nov 2014 NleDocument5 pagesNP 1 Nov 2014 NleSitts YhyNo ratings yet
- Indonesia Health Profile 2017Document474 pagesIndonesia Health Profile 2017Muhammad Aji MaulanaNo ratings yet
- Oral Hygiene Practices and Oral Health Knowledge Among Students in Split, CroatiaDocument13 pagesOral Hygiene Practices and Oral Health Knowledge Among Students in Split, CroatiaAamirNo ratings yet
- History of OncologyDocument2 pagesHistory of OncologyMilagros GarcíaNo ratings yet
- Treatment Outcome and Factors Affecting Time To Recovery in Children With Severe Acute Malnutrition Treated at Outpatient Therapeutic Care ProgramDocument11 pagesTreatment Outcome and Factors Affecting Time To Recovery in Children With Severe Acute Malnutrition Treated at Outpatient Therapeutic Care ProgramMelkamuMeridNo ratings yet
- Hygiene & SanitationDocument12 pagesHygiene & SanitationEd GopsNo ratings yet
- Bioweapon AttackDocument3 pagesBioweapon Attackta84288No ratings yet
- Covid 19: Touch & Dial Directory KolkataDocument22 pagesCovid 19: Touch & Dial Directory KolkataALOKE GANGULYNo ratings yet
- Table 1-ADA Evidence-Grading System For Clinical Practice RecommendationsDocument110 pagesTable 1-ADA Evidence-Grading System For Clinical Practice RecommendationsCarlos EverardoNo ratings yet
- Preparation For ParenthoodDocument8 pagesPreparation For ParenthoodKoushik ChakrabortyNo ratings yet
- Hyperacusis: Major Research Questions: Background Epidemiology and Natural HistoryDocument6 pagesHyperacusis: Major Research Questions: Background Epidemiology and Natural HistoryFuninganaNo ratings yet
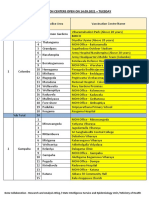
- Vaccination Centers On 14.09.2021Document8 pagesVaccination Centers On 14.09.2021Chanu On CTNo ratings yet
- 906.9203 Rev01 1014SONICflex Brochure LR-1Document20 pages906.9203 Rev01 1014SONICflex Brochure LR-1jonathanmarceNo ratings yet
- Gestational Diabetes Mellitus: Dr. R V S N Sarma., M.D., M.SC., (Canada)Document45 pagesGestational Diabetes Mellitus: Dr. R V S N Sarma., M.D., M.SC., (Canada)Yohannis AsefaNo ratings yet
- STEM-19, Group 5-Topic No. 3Document3 pagesSTEM-19, Group 5-Topic No. 3Erwin Ranel ConstantinoNo ratings yet
- Ehlers-Danlos Panel: ExpertDocument17 pagesEhlers-Danlos Panel: ExpertMalika ButtNo ratings yet
- Effectiveness of Nursing Care On Women Who Have Undergone Abdominal Hysterectomy at Post-Operative Work in Government Head Quarters Hospital, Kancheepuram, District, TamilnaduDocument2 pagesEffectiveness of Nursing Care On Women Who Have Undergone Abdominal Hysterectomy at Post-Operative Work in Government Head Quarters Hospital, Kancheepuram, District, TamilnaduInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Historical Background of Murtala Muhammad Specialist Hospital KanoDocument10 pagesHistorical Background of Murtala Muhammad Specialist Hospital KanoLeenCo TechNo ratings yet
- Long-Term Surgery Graves Disease 20 YearsDocument3 pagesLong-Term Surgery Graves Disease 20 YearsTambunta TariganNo ratings yet
- Prosthodontic Management of Severely ResorbedDocument2 pagesProsthodontic Management of Severely ResorbedAamir BugtiNo ratings yet
- 1463-Article Text-6814-1-10-20231102Document7 pages1463-Article Text-6814-1-10-20231102n2763288No ratings yet
- Bogash 1963Document5 pagesBogash 1963wahyu santikaNo ratings yet
- EINC Newborn Care GuidelinesDocument41 pagesEINC Newborn Care GuidelinesJayrelle D. SafranNo ratings yet
- P & G Purifier of Water - ReviewDocument2 pagesP & G Purifier of Water - ReviewjC HernandezNo ratings yet
- Manage Delirium in Critically Ill Patients Through Prevention, Early Diagnosis and Treatment PDFDocument6 pagesManage Delirium in Critically Ill Patients Through Prevention, Early Diagnosis and Treatment PDFPablo RamirezNo ratings yet
- Oral Pathology: Dr. Tasnim Hamdan Graduated From University of ValenciaDocument160 pagesOral Pathology: Dr. Tasnim Hamdan Graduated From University of ValenciaMariam Abd ElhadiNo ratings yet