You might also like
- Completion of the Partogram in PregnancyDocument9 pagesCompletion of the Partogram in Pregnancyfei cuaNo ratings yet
- GMEC SCN Fetal Monitoring in Labour CTG Guideline FINAL V2.1 September 2020Document33 pagesGMEC SCN Fetal Monitoring in Labour CTG Guideline FINAL V2.1 September 2020Anel BecirspahicNo ratings yet
- Assessment & Procedure For Performing A Vaginal Examination 3.0Document10 pagesAssessment & Procedure For Performing A Vaginal Examination 3.0jomarie gamiaoNo ratings yet
- Fetal Heart Rate Monitoring in Pregnancy and Labour 6.0Document42 pagesFetal Heart Rate Monitoring in Pregnancy and Labour 6.0Wong Lee CheeNo ratings yet
- Kenya Health Facility Assessment ToolDocument9 pagesKenya Health Facility Assessment ToolCelestine WanyonyiNo ratings yet
- Perineal Tear RepairDocument16 pagesPerineal Tear RepairGhaidaasadeqNo ratings yet
- Management of Labour 5.1Document27 pagesManagement of Labour 5.1Lalram Zaua MaramaNo ratings yet
- Trust Guideline For The Management of Stoma Output in Neonates and Infants v1Document23 pagesTrust Guideline For The Management of Stoma Output in Neonates and Infants v1Vian100% (1)
- Agenda Item 10 - Appx 2 - Risk Management Strategy Maternity V 6 2017Document28 pagesAgenda Item 10 - Appx 2 - Risk Management Strategy Maternity V 6 2017saeed hasan saeedNo ratings yet
- Wom1 (09) A - Issue No 5 - Initial Management of Women Experiencing Pain and or Bleeding in Early Pregnancy GuidelineDocument22 pagesWom1 (09) A - Issue No 5 - Initial Management of Women Experiencing Pain and or Bleeding in Early Pregnancy GuidelineMia FernandezNo ratings yet
- Fetal Monitoring in Pregnancy 5.0Document31 pagesFetal Monitoring in Pregnancy 5.0Kovacs TiborNo ratings yet
- Managing Ruptured UterusDocument14 pagesManaging Ruptured Uteruspreethi preethaNo ratings yet
- BREECH BIRTH GUIDELINESDocument13 pagesBREECH BIRTH GUIDELINESBramantyo Aji WicaksonoNo ratings yet
- Occupational Therapy in Neonatal Services and Early Intervention PDFDocument152 pagesOccupational Therapy in Neonatal Services and Early Intervention PDFLauren100% (1)
- Retained Placenta 5.0Document10 pagesRetained Placenta 5.0andi hamatajNo ratings yet
- Trombopenie Polycythemie expertReviewsHemat2014Document11 pagesTrombopenie Polycythemie expertReviewsHemat2014salamredNo ratings yet
- Routine Postnatal Care 4.0Document25 pagesRoutine Postnatal Care 4.0Razelle Hilary Viaña CastroNo ratings yet
- Vaginal Birth After Caesarean Section (VBAC) 5.0Document21 pagesVaginal Birth After Caesarean Section (VBAC) 5.0Savira ChoiNo ratings yet
- hb010 PPH Guideline Hse Home Birth Service 2018Document15 pageshb010 PPH Guideline Hse Home Birth Service 2018Tergantung WaktuNo ratings yet
- Maternity Services Escalation Policy 5.1Document29 pagesMaternity Services Escalation Policy 5.1Bader NammurNo ratings yet
- Safer Surgery UHL PolicyDocument27 pagesSafer Surgery UHL PolicyAsmaa Awad AtiyaNo ratings yet
- Maternity Record Keeping 4.0Document24 pagesMaternity Record Keeping 4.0ItaNo ratings yet
- Management of Meconium Stained Liquor 6.0Document12 pagesManagement of Meconium Stained Liquor 6.0andi hamatajNo ratings yet
- Neon Proc 004 v1Document11 pagesNeon Proc 004 v1SusieNo ratings yet
- Environmental Auditing Guide: European Business Center, Office BC - 25 Dubai Investments Park, PO Box: 166 Dubai-UAEDocument16 pagesEnvironmental Auditing Guide: European Business Center, Office BC - 25 Dubai Investments Park, PO Box: 166 Dubai-UAEMohamad Fazwan Bin Mohd NasirNo ratings yet
- Standard Operating Procedure Manual For Obstetrics and Midwifery ServicesDocument64 pagesStandard Operating Procedure Manual For Obstetrics and Midwifery ServicesTmanoj Praveen75% (4)
- Ghop 2013Document65 pagesGhop 2013petal80No ratings yet
- Procedure For Vaginal Examination 2.1 PDFDocument8 pagesProcedure For Vaginal Examination 2.1 PDFAlfonso AnggriawanNo ratings yet
- Defining Competent Maternal and Newborn Health ProfessionalsDocument42 pagesDefining Competent Maternal and Newborn Health ProfessionalsArti NegiNo ratings yet
- Pharmaceutical Work Breakdown Structure (WBS) Example: Appendix HDocument4 pagesPharmaceutical Work Breakdown Structure (WBS) Example: Appendix HAaronNo ratings yet
- Deterioration in Pregnant or Recently Delivered Women MeowsDocument17 pagesDeterioration in Pregnant or Recently Delivered Women MeowsYudi WiraNo ratings yet
- Dental Clinic ManagementDocument16 pagesDental Clinic Managementsheikh jaber shantoNo ratings yet
- Document Control: Fetal Wellbeing and Monitoring GuidelineDocument17 pagesDocument Control: Fetal Wellbeing and Monitoring GuidelineنورهانعزالدينNo ratings yet
- Induction of LaborDocument124 pagesInduction of LaborFarah DinaNo ratings yet
- Model of Care Diabetic FootDocument22 pagesModel of Care Diabetic FootHendra HefaNo ratings yet
- Midwifery Consultancy Report Provides Valuable InsightsDocument88 pagesMidwifery Consultancy Report Provides Valuable InsightsTalita MaulidaNo ratings yet
- EMAAR MGF D LIMITED HSE MANAGEMENT SYSTEMDocument11 pagesEMAAR MGF D LIMITED HSE MANAGEMENT SYSTEMParmod RanaNo ratings yet
- VTE Risk Assessment and Thromboprophylaxis GuidelineDocument Title: VENOUS THROMBOEMBOLISM (VTE) RISK ASSESSMENT AND THROMBOPROPHYLAXIS IN MATERNITYDocument22 pagesVTE Risk Assessment and Thromboprophylaxis GuidelineDocument Title: VENOUS THROMBOEMBOLISM (VTE) RISK ASSESSMENT AND THROMBOPROPHYLAXIS IN MATERNITYAnonymous 9dVZCnTXSNo ratings yet
- Recruitment and Selection: Reference No. W16.1Document23 pagesRecruitment and Selection: Reference No. W16.1Javed shekhNo ratings yet
- HR quarterly report highlights key issuesDocument11 pagesHR quarterly report highlights key issuesZaffir Zainal AbidinNo ratings yet
- Control and Management of Methicillin Resistant Staphylococcus Aureus (MRSA) / Michelle Bergin ... (Et Al.)Document36 pagesControl and Management of Methicillin Resistant Staphylococcus Aureus (MRSA) / Michelle Bergin ... (Et Al.)alshanNo ratings yet
- Paediatric abdominal pain pathwayDocument10 pagesPaediatric abdominal pain pathwayDwi PuspitaNo ratings yet
- WP 01 Guidance Safe WorkDocument20 pagesWP 01 Guidance Safe WorkCarlos GuevaraNo ratings yet
- WHO Labour Care Guide: User'S ManualDocument42 pagesWHO Labour Care Guide: User'S ManualWidia RamadaniNo ratings yet
- Examination of The Newborn InfantDocument15 pagesExamination of The Newborn InfantWilda AwliaNo ratings yet
- Techniques for Manual Patient HandlingDocument41 pagesTechniques for Manual Patient HandlingJasonJejametNo ratings yet
- Roles and Responsibilities of Medical and Midwifery Staff 4.4 PDFDocument22 pagesRoles and Responsibilities of Medical and Midwifery Staff 4.4 PDFSaleena ResheedNo ratings yet
- Ministry of Health Malaysia releases updated credentialing guidelinesDocument142 pagesMinistry of Health Malaysia releases updated credentialing guidelinesFirdaus Al HafizNo ratings yet
- A Guideline For The Management of Caesarean Section: Document SummaryDocument24 pagesA Guideline For The Management of Caesarean Section: Document SummaryRano HatNo ratings yet
- HSE Incident Management Procedure SummaryDocument30 pagesHSE Incident Management Procedure SummaryPippo Topolino50% (2)
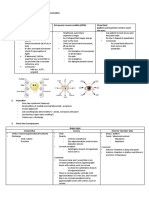
- Transport of CellsDocument20 pagesTransport of CellsshneetsNo ratings yet
- WIN Project Manual for Family-Centered Maternity Care TrainingDocument120 pagesWIN Project Manual for Family-Centered Maternity Care TrainingIsraNo ratings yet
- PR-GM 09 Identification and Control Ofnon Conformance ProcedureDocument5 pagesPR-GM 09 Identification and Control Ofnon Conformance ProcedureFULGENCE RUHARARANo ratings yet
- Pgs Guidelines en IFOAMDocument47 pagesPgs Guidelines en IFOAMRania Touma WannaNo ratings yet
- Emergency Department SOP V4.1Document17 pagesEmergency Department SOP V4.1Faisol KabirNo ratings yet
- Antenatal Care1Document454 pagesAntenatal Care1Abanoub Philopater RushdyNo ratings yet
- Internal Investigations: A Basic Guide Anyone Can UseFrom EverandInternal Investigations: A Basic Guide Anyone Can UseRating: 3 out of 5 stars3/5 (1)
- L1 Vbac PDFDocument16 pagesL1 Vbac PDFMuhammad HaziqNo ratings yet
- Benign and Malignant Tumor of UterusDocument138 pagesBenign and Malignant Tumor of UterusMuhammad HaziqNo ratings yet
- Fundamentals of OpthalmologyDocument4 pagesFundamentals of OpthalmologyMuhammad HaziqNo ratings yet
- Ocular Exam GuideDocument2 pagesOcular Exam GuideMuhammad HaziqNo ratings yet
- (Practical) OphthalmosDocument32 pages(Practical) OphthalmosHoriana BusuiocNo ratings yet
- CWU AttirahDocument13 pagesCWU AttirahMuhammad HaziqNo ratings yet
- Ocular ExaminationDocument2 pagesOcular ExaminationMuhammad HaziqNo ratings yet
- Case Write Up OphthalmologyDocument11 pagesCase Write Up OphthalmologyMuhammad HaziqNo ratings yet
- Cwu Orthoy4Document10 pagesCwu Orthoy4Muhammad HaziqNo ratings yet
- Case Write Up Ortho JaneDocument15 pagesCase Write Up Ortho JaneMuhammad HaziqNo ratings yet
- Cwu OrthopaedicDocument13 pagesCwu OrthopaedicMuhammad HaziqNo ratings yet
- Urinary Tract Infection in ChildrenDocument45 pagesUrinary Tract Infection in ChildrenMuhammad HaziqNo ratings yet
- Cwu OrhtoDocument15 pagesCwu OrhtoMuhammad HaziqNo ratings yet
- Bronchial Asthma Ina Childhood Case Based Learning October 2021Document2 pagesBronchial Asthma Ina Childhood Case Based Learning October 2021Muhammad HaziqNo ratings yet
- (CSL8) Pleural Tap & BiopsyDocument6 pages(CSL8) Pleural Tap & BiopsyMuhammad HaziqNo ratings yet
- BronchiectasisDocument24 pagesBronchiectasisMuhammad HaziqNo ratings yet
- Child TCLDocument12 pagesChild TCLlaliejhessNo ratings yet
- Vasa PraeviaDocument3 pagesVasa PraeviaAngelica CabututanNo ratings yet
- Fish Cant See Water The Need To Humanize BirthDocument13 pagesFish Cant See Water The Need To Humanize BirthludierludyNo ratings yet
- Daftar Pustaka Hipertensi Dalam KehamilanDocument2 pagesDaftar Pustaka Hipertensi Dalam KehamilanIndah Juni YantiNo ratings yet
- สูติบัตรDocument1 pageสูติบัตรchusak1234No ratings yet
- How To Optimize Nutrition in Preterm Infants With IUGR: Rinawati RohsiswatmoDocument38 pagesHow To Optimize Nutrition in Preterm Infants With IUGR: Rinawati Rohsiswatmodian kurniasariNo ratings yet
- Ob Osce.04 CTG ReadingDocument6 pagesOb Osce.04 CTG ReadingDasha VeeNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesJelica AlvarezNo ratings yet
- General ObjectivesDocument13 pagesGeneral ObjectiveskevinNo ratings yet
- DR ScrubsDocument1 pageDR ScrubsninzestrellaNo ratings yet
- Prolapse of The Umbilical CordDocument13 pagesProlapse of The Umbilical CordJm OpolintoNo ratings yet
- Abortus Rsud UngaranDocument11 pagesAbortus Rsud Ungaranmardiana siregarNo ratings yet
- Involution and LochiaDocument2 pagesInvolution and Lochiaapi-316491996100% (1)
- Prenatal Factors Influencing Growth and Development of FetusDocument15 pagesPrenatal Factors Influencing Growth and Development of FetusSrd Rch100% (1)
- Antepartum, Intrapartum and Postpartm Fevers.M2 2009pptDocument15 pagesAntepartum, Intrapartum and Postpartm Fevers.M2 2009pptIdiAmadouNo ratings yet
- SYNOPSISDocument25 pagesSYNOPSISpriyankaNo ratings yet
- Prolonged PregnancyDocument45 pagesProlonged PregnancyReshmi S ChellappanNo ratings yet
- Workshop In-Alarm: Scientific Program Pre - CongressDocument3 pagesWorkshop In-Alarm: Scientific Program Pre - Congressdaniel_alexander_susenoNo ratings yet
- How To Have An Awesome Birthe BookDocument278 pagesHow To Have An Awesome Birthe BookgovacityNo ratings yet
- Evidence-Based Ways to Reduce Maternal MortalityDocument44 pagesEvidence-Based Ways to Reduce Maternal MortalityJalajarani Aridass100% (1)
- The Iona Test Reduces The Need For Invasive Procedures:: 100,000 PregnanciesDocument2 pagesThe Iona Test Reduces The Need For Invasive Procedures:: 100,000 PregnanciesionelaioneNo ratings yet
- Assessment Diagnosis Rationale Planning Interventio N Rationale EvaluationDocument2 pagesAssessment Diagnosis Rationale Planning Interventio N Rationale Evaluationbambem aevanNo ratings yet
- Cesearean Section FinalDocument62 pagesCesearean Section FinalsanthiyasandyNo ratings yet
- Labor Duration Guidelines SummaryDocument1 pageLabor Duration Guidelines Summaryjust for download matterNo ratings yet
- Multiple-Pregnancy - 2Document9 pagesMultiple-Pregnancy - 2Queenie SilvaNo ratings yet
- SynopsisDocument10 pagesSynopsisAhmedMalikNo ratings yet
- Meredith Grey's Patient ProfileDocument1 pageMeredith Grey's Patient ProfileQueenzee AsuncionNo ratings yet
- Blighted OvumDocument33 pagesBlighted Ovumamirz_4100% (1)
- Intrauterine Fetal Death (IUD)Document10 pagesIntrauterine Fetal Death (IUD)Sivaram Shanmugha VilasNo ratings yet
- BREECH BIRTH GUIDELINESDocument13 pagesBREECH BIRTH GUIDELINESBramantyo Aji WicaksonoNo ratings yet