You might also like
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Plate and Screw TraumaDocument46 pagesPlate and Screw Traumaianfajar8No ratings yet
- Operating Room PersonnelDocument44 pagesOperating Room Personnelamir hamzahNo ratings yet
- Surgery IIExam 1 REVIEWDocument6 pagesSurgery IIExam 1 REVIEWEddie MillsNo ratings yet
- Plate and Screw TraumaDocument45 pagesPlate and Screw TraumaRichard 151289No ratings yet
- History of OsteosynthesisDocument9 pagesHistory of OsteosynthesisPankaj VatsaNo ratings yet
- Prinicple of External FixatorDocument29 pagesPrinicple of External FixatorAnkit KarkiNo ratings yet
- Basic Principles and Techniques of Internal Fixation of FracturesDocument56 pagesBasic Principles and Techniques of Internal Fixation of FracturesRudi haris munandarNo ratings yet
- Type and Biomaterial ImplantDocument36 pagesType and Biomaterial ImplantluthfisnetNo ratings yet
- AOAF Presentation LCPDocument45 pagesAOAF Presentation LCPRajiv YadavNo ratings yet
- Know Your Tools Series: 'A Mind That Can Comprehend The Principle Will Device Its Own Methods.'' Nicolas AndryDocument91 pagesKnow Your Tools Series: 'A Mind That Can Comprehend The Principle Will Device Its Own Methods.'' Nicolas Andrymuhammad ammar naqviNo ratings yet
- External FixatorsDocument49 pagesExternal FixatorsdvenumohanNo ratings yet
- IMPLANTSDocument24 pagesIMPLANTSHarsh PawarNo ratings yet
- Principle of NailingDocument62 pagesPrinciple of Nailingsharvindan subramaniamNo ratings yet
- Intramedullar Nail 3Document39 pagesIntramedullar Nail 3Dr NIVEDITHA CNo ratings yet
- Pricippriles of Intramedullary NailingDocument57 pagesPricippriles of Intramedullary NailingAbdallah OmerNo ratings yet
- Orthopaedics Instruments: Kirschner WireDocument17 pagesOrthopaedics Instruments: Kirschner WireBi PinNo ratings yet
- G11 Ex Fix Principles JTG Rev 2 4 10Document70 pagesG11 Ex Fix Principles JTG Rev 2 4 10Aprilia Eka PutriNo ratings yet
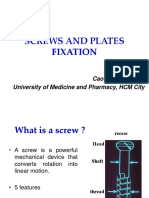
- Screws and Plates Fixation: Cao Ba Huong, MD University of Medicine and Pharmacy, HCM CityDocument38 pagesScrews and Plates Fixation: Cao Ba Huong, MD University of Medicine and Pharmacy, HCM CityWasim R. IssaNo ratings yet
- Trochanteric #Document20 pagesTrochanteric #Prakash AyyaduraiNo ratings yet
- 03-06 Internal FixationDocument69 pages03-06 Internal Fixation69016No ratings yet
- Implant SystemsDocument103 pagesImplant SystemsBharathi GudapatiNo ratings yet
- OverdentureDocument97 pagesOverdentureAmit Bhargav100% (1)
- The Use of Plates in Fracture FixationDocument23 pagesThe Use of Plates in Fracture FixationhaminatrafNo ratings yet
- Implants in OrthopaedicsDocument20 pagesImplants in OrthopaedicsDr. F. Abdul KhaderNo ratings yet
- Internal FixationDocument22 pagesInternal Fixationlotd6002No ratings yet
- Principle of Screw and Plate Fixation & Mechanical Behavior of Implant MaterialsDocument40 pagesPrinciple of Screw and Plate Fixation & Mechanical Behavior of Implant MaterialsagusNo ratings yet
- 2.3 Use of Plates in Fracture FixationDocument22 pages2.3 Use of Plates in Fracture FixationAlex DiconiNo ratings yet
- Fracture FixationDocument21 pagesFracture FixationMISS. COMNo ratings yet
- AO Plating Basics (Brief)Document6 pagesAO Plating Basics (Brief)Jake sanchezNo ratings yet
- Finishing Stage Part 2Document132 pagesFinishing Stage Part 2sahar emadNo ratings yet
- Plates and Screws: An Overview: Presented by DR Oteki MisianiDocument45 pagesPlates and Screws: An Overview: Presented by DR Oteki MisianiIan OrwaNo ratings yet
- Ilizarov Fixator: DR Pratik AgarwalDocument86 pagesIlizarov Fixator: DR Pratik AgarwaltesfahuntekletilahunNo ratings yet
- Applied Biomechanics of Hip ArthroplastyDocument28 pagesApplied Biomechanics of Hip ArthroplastyAgung TristyantoNo ratings yet
- Plates: Iwan B Anwar. Dr. SpotDocument59 pagesPlates: Iwan B Anwar. Dr. SpotTiffani ApriliaNo ratings yet
- FixinCatalog PDFDocument44 pagesFixinCatalog PDFWedoeditor Fast100% (1)
- Biomechanics of Fractures and FixationDocument70 pagesBiomechanics of Fractures and FixationnishantsinghbmeNo ratings yet
- FixinDocument44 pagesFixinJaime EscobarNo ratings yet
- ProsthesisDocument42 pagesProsthesissmrutiptNo ratings yet
- Open Reduction Internal Fixation RifDocument16 pagesOpen Reduction Internal Fixation RifNurul Hidayah100% (2)
- Principles of External FixationDocument36 pagesPrinciples of External Fixationcromwellopoku42No ratings yet
- Biomechanics of Pin and Post Retained Restorations-MadhurimaDocument190 pagesBiomechanics of Pin and Post Retained Restorations-Madhurimarasagna reddy100% (1)
- Codo MedartisDocument36 pagesCodo MedartisavillouNo ratings yet
- Large Fragment Locking Compression Plate (LCP) : Technique GuideDocument23 pagesLarge Fragment Locking Compression Plate (LCP) : Technique GuideLouis MiuNo ratings yet
- Implant-Supported Fixed Dental Prosthesis With A MicrolockingDocument31 pagesImplant-Supported Fixed Dental Prosthesis With A MicrolockingbalwantNo ratings yet
- Plates and ScrewsDocument96 pagesPlates and ScrewsFathy AlhallagNo ratings yet
- Lecture 3Document65 pagesLecture 3bme.21.282No ratings yet
- General A7 Principles of External FixationDocument75 pagesGeneral A7 Principles of External FixationNabil AhmedNo ratings yet
- Anatomi Sistem MuskuloskeletalDocument48 pagesAnatomi Sistem MuskuloskeletalSujana100% (1)
- Bolted ConnectionDocument56 pagesBolted ConnectionScracher Sahil ChauhanNo ratings yet
- Bolted Connections PDFDocument56 pagesBolted Connections PDFÃvēđÆñ ŤhåķųřNo ratings yet
- Bridge Plating PDFDocument4 pagesBridge Plating PDFKae 王珊婷 Wang100% (1)
- DE Module 3Document40 pagesDE Module 3AVERAGENo ratings yet
- Fracture ManagementDocument50 pagesFracture ManagementCharLes OdalNo ratings yet
- Rite Up PDFDocument66 pagesRite Up PDFDayal SharanNo ratings yet
- 15 170521052253 محولDocument32 pages15 170521052253 محول22368717No ratings yet
- Inramedullarynailingpptfinal 160902185707Document65 pagesInramedullarynailingpptfinal 160902185707Pankaj VatsaNo ratings yet
- G11-Principles of External FixationDocument111 pagesG11-Principles of External Fixationhello from the other side100% (1)
- AO Plates & Their ApplicationDocument74 pagesAO Plates & Their ApplicationAbu ZidaneNo ratings yet
- Malleolar Fractures 17Document41 pagesMalleolar Fractures 17ABUBAKER ZANBOUZINo ratings yet
- Intro HADocument38 pagesIntro HAMuhammad Abbas WaliNo ratings yet
- Weight ManagementDocument50 pagesWeight Managementzia ullahNo ratings yet
- Cncept of SexulaityDocument25 pagesCncept of SexulaityMuhammad Abbas WaliNo ratings yet
- Cncept of SexulaityDocument25 pagesCncept of SexulaityMuhammad Abbas WaliNo ratings yet
- Lecture 3 Cell - Structure - FunctionDocument94 pagesLecture 3 Cell - Structure - FunctionMuhammad Abbas WaliNo ratings yet
- Lecture 9 CVSDocument118 pagesLecture 9 CVSMuhammad Abbas WaliNo ratings yet
- Loss, Death, and Grieving - PPTX 222222-1Document37 pagesLoss, Death, and Grieving - PPTX 222222-1Muhammad Abbas Wali100% (1)
- Ovulation - ReproDocument14 pagesOvulation - ReproMuhammad Abbas WaliNo ratings yet
- BURNDocument45 pagesBURNMuhammad Abbas WaliNo ratings yet
- Red Winemaking in Cool Climates: Belinda Kemp Karine PedneaultDocument10 pagesRed Winemaking in Cool Climates: Belinda Kemp Karine Pedneaultgjm126No ratings yet
- "Hiv and Aids Awareness of Junior and Senior High School Students" Part I: Profile of RespondentsDocument1 page"Hiv and Aids Awareness of Junior and Senior High School Students" Part I: Profile of RespondentsDahl xxNo ratings yet
- Mental Health & TravelDocument18 pagesMental Health & TravelReyza HasnyNo ratings yet
- 4 - Mixing Equipments Used in Flocculation and CoagulationDocument27 pages4 - Mixing Equipments Used in Flocculation and Coagulationhadeer osmanNo ratings yet
- Process of Reinstatement Value Fire PoliciesDocument1 pageProcess of Reinstatement Value Fire PoliciesvinaysekharNo ratings yet
- Agriculture and FisheryDocument5 pagesAgriculture and FisheryJolliven JamiloNo ratings yet
- Unit 18: Calculating Food Costs, Selling Prices and Making A ProfitDocument4 pagesUnit 18: Calculating Food Costs, Selling Prices and Making A Profitkarupukamal100% (2)
- VedasUktimAlA Sanskrit Hindi EnglishDocument47 pagesVedasUktimAlA Sanskrit Hindi EnglishAnantha Krishna K SNo ratings yet
- Module 6 - Addictions Prayer ServiceDocument6 pagesModule 6 - Addictions Prayer Serviceapi-450520432No ratings yet
- Dirty Dozen List of Endocrine DisruptorsDocument4 pagesDirty Dozen List of Endocrine DisruptorsMariuszNo ratings yet
- Inversor Abb 3 8kwDocument2 pagesInversor Abb 3 8kwapi-290643326No ratings yet
- 7B Form GRA Original - Part499 PDFDocument1 page7B Form GRA Original - Part499 PDFRicardo SinghNo ratings yet
- Sasol Polymers PP HNR100Document3 pagesSasol Polymers PP HNR100Albert FortunatoNo ratings yet
- MS 1979 2015Document44 pagesMS 1979 2015SHARIFFAH KHAIRUNNISA BINTI SYED MUHAMMAD NASIR A19EE0151No ratings yet
- Entrepreneurship Paper 2Document3 pagesEntrepreneurship Paper 2kisebe yusufNo ratings yet
- Reaction Paper On Water PollutionDocument1 pageReaction Paper On Water PollutionAztah KivycNo ratings yet
- PP Aaa PP1 141Document30 pagesPP Aaa PP1 141Rabah AmidiNo ratings yet
- Melancholic PersonalityDocument5 pagesMelancholic PersonalityChris100% (1)
- 13 Methods To Increase Your Conditioning - Strength by SkylerDocument5 pages13 Methods To Increase Your Conditioning - Strength by SkylerMarko Štambuk100% (1)
- Babok Framework Overview: BA Planning & MonitoringDocument1 pageBabok Framework Overview: BA Planning & MonitoringJuan100% (1)
- How To Defend The Faith Without Raising Your VoiceDocument139 pagesHow To Defend The Faith Without Raising Your VoiceCleber De Souza Cunha100% (2)
- The Exceeding Sinfulness of Sin - Guy CaskeyDocument402 pagesThe Exceeding Sinfulness of Sin - Guy Caskeyclaroblanco100% (1)
- Sewage and Effluent Water Treatment Plant Services in PuneDocument11 pagesSewage and Effluent Water Treatment Plant Services in PunedipakNo ratings yet
- Anglo American - Belt Conveyor Design CriteriaDocument19 pagesAnglo American - Belt Conveyor Design CriteriaIgor San Martín Peñaloza0% (1)
- The Allied Valve Spares Manufacturer Company Maharashtra IndiaDocument10 pagesThe Allied Valve Spares Manufacturer Company Maharashtra IndiaThe Allied Valve Spares Manufacturer CompanyNo ratings yet
- MCQ Cell InjuryDocument19 pagesMCQ Cell InjuryMoaz EbrahimNo ratings yet
- Air MassesDocument22 pagesAir MassesPrince MpofuNo ratings yet
- Diplomate Course and Conferment RequirementsDocument1 pageDiplomate Course and Conferment Requirementsabigail lausNo ratings yet
- TextDocument3 pagesTextKristineNo ratings yet