You might also like
- 1 ❤ Smart Sheet for History Taking in Internal Medicine خلفية سماويةDocument12 pages1 ❤ Smart Sheet for History Taking in Internal Medicine خلفية سماويةOsama A100% (1)
- CCTV Consent FormDocument2 pagesCCTV Consent FormGam SaiiNo ratings yet
- 3 ❤ Smart Sheet for History Taking in Pediatrics خلفية صفراءDocument14 pages3 ❤ Smart Sheet for History Taking in Pediatrics خلفية صفراءsalah almozahemNo ratings yet
- Clerkship Resources Additional NotesDocument4 pagesClerkship Resources Additional NotesAnnaNo ratings yet
- Form Sbar Rsud SananaDocument5 pagesForm Sbar Rsud SananaDesman SyahNo ratings yet
- High Risk Consent Form: Doctor-In-Charge / Principal Surgeon / Principal InterventionistDocument5 pagesHigh Risk Consent Form: Doctor-In-Charge / Principal Surgeon / Principal InterventionistDrPraveen SharmaNo ratings yet
- Pharmacy Guidelines For Dispensing of MedicinesDocument9 pagesPharmacy Guidelines For Dispensing of MedicinesAngelica Lee Acebuche PalmeroNo ratings yet
- MCPS in Family Medicine: Individual Module: Rs 3000Document1 pageMCPS in Family Medicine: Individual Module: Rs 3000NASIR MEHMOOD KHANNo ratings yet
- 2020 Mcqs Case Selection and TX PlanDocument18 pages2020 Mcqs Case Selection and TX Planareej alblowiNo ratings yet
- Cancer EpidemiologyDocument18 pagesCancer EpidemiologyMariaLisseth MoralesNo ratings yet
- Consent Waiver of Medical / Surgery: ST NDDocument2 pagesConsent Waiver of Medical / Surgery: ST NDrekam medis selaras100% (1)
- Surat Rujukan Bahasa InggrisDocument1 pageSurat Rujukan Bahasa InggrisJondry Suitela100% (2)
- Form Resume MedisDocument2 pagesForm Resume MedisDesi AndrianovitaNo ratings yet
- 4-Drugs in Obs & GyneDocument52 pages4-Drugs in Obs & Gyneapi-37033520% (2)
- Quality Improvement ProjectDocument7 pagesQuality Improvement Projectapi-272534722100% (1)
- A Descriptive Study To Assess The Knowledge and Attitude On Birth Preparedness Among Primigravida Mothers Attending Gynae OPD at Civil Hospital Sangrur, PunjabDocument27 pagesA Descriptive Study To Assess The Knowledge and Attitude On Birth Preparedness Among Primigravida Mothers Attending Gynae OPD at Civil Hospital Sangrur, PunjabEditor IJTSRDNo ratings yet
- RTG Hozzájárulási Nyilatkozat AngolDocument2 pagesRTG Hozzájárulási Nyilatkozat AngolMui Nguyen NgocNo ratings yet
- 3.1.1 EP b.3 FORMAT INFORMED CONSENTDocument3 pages3.1.1 EP b.3 FORMAT INFORMED CONSENTRifda NurfadilahNo ratings yet
- Wellness Check Consent Form-3Document1 pageWellness Check Consent Form-3Matthew TivNo ratings yet
- 3.medical FormDocument5 pages3.medical Formamistudio30No ratings yet
- Form of Informed and Voluntary Consent To Participate in ResearchDocument1 pageForm of Informed and Voluntary Consent To Participate in ResearchrianadhiviraNo ratings yet
- I.M.E. Life Insurance Company LTD.: Physician'S Statement For Critical IllnessDocument2 pagesI.M.E. Life Insurance Company LTD.: Physician'S Statement For Critical IllnessMystic MilanNo ratings yet
- Format PengkajianDocument5 pagesFormat Pengkajianhestika dondaNo ratings yet
- Obstetric & Gynecology Departement Medical School / General Hospital FK UKIDocument7 pagesObstetric & Gynecology Departement Medical School / General Hospital FK UKIImanuel CristiantoNo ratings yet
- New Cashless FormDocument4 pagesNew Cashless FormPrhnsht mindraNo ratings yet
- Form General Consent UmumDocument2 pagesForm General Consent Umumcut hervizaNo ratings yet
- Generic Consent FormDocument4 pagesGeneric Consent Formfoobar24No ratings yet
- ملزمة دورة المهارات معهد اديسون مضغوطةDocument76 pagesملزمة دورة المهارات معهد اديسون مضغوطةruba al hammadiNo ratings yet
- Informed Consent Form For Sterilization OperationDocument8 pagesInformed Consent Form For Sterilization Operationjobs shahiNo ratings yet
- Form Rekom SIP IDI JakselDocument6 pagesForm Rekom SIP IDI JakselMimi SunaryantiNo ratings yet
- BIU Clinic FormsDocument4 pagesBIU Clinic FormsMarvellous AbrahamNo ratings yet
- BNA Senior Games Registration Forms 2023Document3 pagesBNA Senior Games Registration Forms 2023Serena RouseNo ratings yet
- Puskesmas Tanjung Beringin: Pemerintah Kabupaten Pesisir SelatanDocument1 pagePuskesmas Tanjung Beringin: Pemerintah Kabupaten Pesisir SelatanHanna GustinNo ratings yet
- Blood Donation Application FormDocument2 pagesBlood Donation Application FormFadjar MulyaNo ratings yet
- 7.4.4.2 Lembar Informed Consent TerisiDocument1 page7.4.4.2 Lembar Informed Consent Terisititis dwinaNo ratings yet
- Form Claim Section A - Med ExDocument4 pagesForm Claim Section A - Med Exerwin hpNo ratings yet
- Resume Evaluasi Praktek Keperawatan Dasar Profesi Tanggal: ................................Document6 pagesResume Evaluasi Praktek Keperawatan Dasar Profesi Tanggal: ................................Mira KumalaNo ratings yet
- AdmissionForm GIMDocument2 pagesAdmissionForm GIMSanjay SahooNo ratings yet
- Claim FormDocument3 pagesClaim Forma.a.wiratamaNo ratings yet
- Show PDFDocument2 pagesShow PDFSandip MandalNo ratings yet
- Anesthesia ConsentDocument4 pagesAnesthesia ConsentvinodshsaNo ratings yet
- Uptd Puskesmas Bandar Agung: Rujukan EksternalDocument1 pageUptd Puskesmas Bandar Agung: Rujukan Eksternalirsyad robaniNo ratings yet
- Form KDMDocument49 pagesForm KDMFirdaus MaulanaNo ratings yet
- Informed ConsentDocument3 pagesInformed ConsentFitria anandaNo ratings yet
- GP Referral Form 2023Document1 pageGP Referral Form 2023Rahul VishwanathNo ratings yet
- 2018 +Generali+Claim+form EN+ (Legal+rev) +-+171017Document2 pages2018 +Generali+Claim+form EN+ (Legal+rev) +-+171017Femi EvalnesNo ratings yet
- History SheetDocument4 pagesHistory Sheetmonirul islam shohanNo ratings yet
- RM 3 Ugd Assesment Medis UgdDocument3 pagesRM 3 Ugd Assesment Medis UgdHajrah SaidNo ratings yet
- Contoh Format INC FisiologisDocument11 pagesContoh Format INC FisiologisSyauqi NgkNo ratings yet
- Contoh Format INC Fisiologis Dan PatologisDocument12 pagesContoh Format INC Fisiologis Dan PatologisSyauqi NgkNo ratings yet
- Tue Application FormDocument4 pagesTue Application FormHengky AntonNo ratings yet
- Joint Admissions and Matriculation BoardgrtgtDocument1 pageJoint Admissions and Matriculation BoardgrtgtElujekwute BenjaminNo ratings yet
- Mekonnen Gizachew PDFDocument60 pagesMekonnen Gizachew PDFkelid IbrahimNo ratings yet
- Keterangan Sebab Kematian: Rs. Surya Asih PringsewuDocument1 pageKeterangan Sebab Kematian: Rs. Surya Asih PringsewuAtika Eka RachmayatiNo ratings yet
- Application Form PT WBA CrewDocument2 pagesApplication Form PT WBA CrewRiki DeltaboxNo ratings yet
- Medical CertificateDocument4 pagesMedical Certificateมุทิตา แสนบุญศรีNo ratings yet
- Format Asuhan Keperawatan Medikal BedahDocument9 pagesFormat Asuhan Keperawatan Medikal Bedahkhairunisa AnnurNo ratings yet
- Lamp 1 Format KMB For UDocument9 pagesLamp 1 Format KMB For UAgusTinusNo ratings yet
- DentistsstatementDocument1 pageDentistsstatementEmmanuelle PetitNo ratings yet
- Fresh Start Doctor Referral Form 2022 PDFDocument1 pageFresh Start Doctor Referral Form 2022 PDFZoee WestworthNo ratings yet
- Form PIODocument1 pageForm PIOabdul latifNo ratings yet
- Doctor AffidavitsDocument1 pageDoctor AffidavitsabdiNo ratings yet
- Doctor AffidavitsDocument1 pageDoctor Affidavits[pmlNo ratings yet
- Ina Chapter 3Document1 pageIna Chapter 3Riany Jade SabrinaNo ratings yet
- How To Have SexDocument1 pageHow To Have SexNìkhíl HonêyNo ratings yet
- Form Pendaftaran - 020051Document3 pagesForm Pendaftaran - 020051Dimass PrassetioNo ratings yet
- Not Just for Stoners: Everything You've Always Wanted to Know About Cannabis But Were Afraid to AskFrom EverandNot Just for Stoners: Everything You've Always Wanted to Know About Cannabis But Were Afraid to AskRating: 5 out of 5 stars5/5 (2)
- Describe The Activity Based On The Following: Walking Around For 5 Minutes Brisk Walking For 4 Minutes 3-Minute Jump JacksDocument4 pagesDescribe The Activity Based On The Following: Walking Around For 5 Minutes Brisk Walking For 4 Minutes 3-Minute Jump JacksJeremiah Se-engNo ratings yet
- Seroepidemiology of Clamaydia TDocument8 pagesSeroepidemiology of Clamaydia TMulatuNo ratings yet
- Uterine RuptureDocument14 pagesUterine RuptureHazelkaye AbadNo ratings yet
- Who 2019 Ncov Ipcppe Use 2020.2 EngDocument7 pagesWho 2019 Ncov Ipcppe Use 2020.2 EngAnty AuliaNo ratings yet
- Covid 19 Risk Assessment PresentationDocument23 pagesCovid 19 Risk Assessment PresentationAljur OntawarNo ratings yet
- A Case Report On Kartagener's SyndromeDocument3 pagesA Case Report On Kartagener's SyndromeBaru Chandrasekhar RaoNo ratings yet
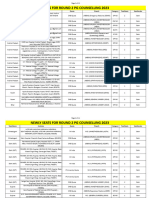
- Newly Seats For Round 2 PG Counselling 2023Document11 pagesNewly Seats For Round 2 PG Counselling 2023Manoj KumarNo ratings yet
- Lung Disease and Copd Seminar PresentationDocument14 pagesLung Disease and Copd Seminar Presentationapi-402325622No ratings yet
- 2.5 Herbal Medicine As Alternative MedicineDocument3 pages2.5 Herbal Medicine As Alternative MedicineIsla SpencerNo ratings yet
- Service Annotated BibliographyDocument6 pagesService Annotated Bibliographyapi-355966257No ratings yet
- Prevalence of Down SyndromeDocument4 pagesPrevalence of Down SyndromeAbhinav MishraNo ratings yet
- Virology DatabaseDocument56 pagesVirology DatabaseAhraNo ratings yet
- Recist Criteria - Respon Solid Tumor Pada TerapiDocument18 pagesRecist Criteria - Respon Solid Tumor Pada TerapiBhayu Dharma SuryanaNo ratings yet
- Professional Interview Assignment - Group 20Document11 pagesProfessional Interview Assignment - Group 20api-356121202No ratings yet
- FARMASAINS Vol. Xx. No. XX, Bulan TahunDocument9 pagesFARMASAINS Vol. Xx. No. XX, Bulan TahunShonia FatwaNo ratings yet
- QDT 2012 Quintessence of DentalDocument238 pagesQDT 2012 Quintessence of DentalRazvan UngureanuNo ratings yet
- Hiv Hub Clinics Doh2023 0284Document14 pagesHiv Hub Clinics Doh2023 0284Juvelle CambiaNo ratings yet
- 06 22 2018 Cne Prep Course CertificateDocument1 page06 22 2018 Cne Prep Course Certificateapi-372924050No ratings yet
- Bangladesh 2012-13 MICS Final ReportDocument272 pagesBangladesh 2012-13 MICS Final ReportMD. ROBIUL ISLAM TALUKDERNo ratings yet
- Quality Improvement ProjectDocument6 pagesQuality Improvement Projectapi-629209689No ratings yet
- n478 Cover Letter 1Document1 pagen478 Cover Letter 1api-509458762No ratings yet
- Protocolo Estudio RadicalsDocument66 pagesProtocolo Estudio RadicalsandresNo ratings yet