You might also like
- Coronary Vasomotion AbnormalitiesFrom EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaNo ratings yet
- Leong2015 Hub Total Waktu Iskemik LVMD Dan AritmiaDocument8 pagesLeong2015 Hub Total Waktu Iskemik LVMD Dan AritmiaauliaNo ratings yet
- tmp9120 TMPDocument6 pagestmp9120 TMPFrontiersNo ratings yet
- An Important Cause of Wide Complex Tachycardia: Case PresentationDocument2 pagesAn Important Cause of Wide Complex Tachycardia: Case PresentationLuis Fernando Morales JuradoNo ratings yet
- T-Wave AlternansDocument11 pagesT-Wave AlternansМихаил НеболеевNo ratings yet
- Spot Diagnosis Using Pulse Wave Doppler Interrogation of The Abdominal AortaDocument2 pagesSpot Diagnosis Using Pulse Wave Doppler Interrogation of The Abdominal AortaHand SanitizerNo ratings yet
- Pacing Clinical Electrophis - 2022 - MartiniDocument10 pagesPacing Clinical Electrophis - 2022 - MartiniRobertoNo ratings yet
- 5.RCA or LCX in Inferior MIDocument7 pages5.RCA or LCX in Inferior MIAshraf ChowdhuryNo ratings yet
- Single Coronary Artery Anomaly Case ReportDocument5 pagesSingle Coronary Artery Anomaly Case ReportJhonike NawipaNo ratings yet
- Ecg ThalasemiaDocument16 pagesEcg ThalasemiaFian AldyNo ratings yet
- Articol BrsDocument21 pagesArticol BrsIulia NistorNo ratings yet
- The Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseDocument9 pagesThe Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseshodhgangaNo ratings yet
- Cardiac Arrhythmia RisksDocument17 pagesCardiac Arrhythmia RisksAnel ConquetNo ratings yet
- How Dangerous Is Hyperkalemia?Document11 pagesHow Dangerous Is Hyperkalemia?Erika SalazarNo ratings yet
- Thesis FinaaaaaallllllDocument201 pagesThesis FinaaaaaallllllMunir AlshameeryNo ratings yet
- Perioperative Cardiac Arrhythmias: A. Thompson and J. R. BalserDocument9 pagesPerioperative Cardiac Arrhythmias: A. Thompson and J. R. BalsererzaraptorNo ratings yet
- Cardiac Sodium Channelopathies: Ion Channels, Receptors and TransportersDocument15 pagesCardiac Sodium Channelopathies: Ion Channels, Receptors and TransportersRicardo QuinteiroNo ratings yet
- HHS Public Access: The Electrophysiology of Hypo-And HyperkalemiaDocument21 pagesHHS Public Access: The Electrophysiology of Hypo-And HyperkalemiaDickyNo ratings yet
- 1 s2.0 S0735109710025726 MainDocument12 pages1 s2.0 S0735109710025726 MainretnoNo ratings yet
- ECG Frequency Changes inDocument13 pagesECG Frequency Changes inArief KamilNo ratings yet
- Mujer Con Torsades de PointesDocument2 pagesMujer Con Torsades de PointesAníbal José Arroyo RodríguezNo ratings yet
- Diffuse ST Segment Depression and ST Segment Elevation in Lead aVR and V1 by Left Circumflex Artery OcclusionDocument3 pagesDiffuse ST Segment Depression and ST Segment Elevation in Lead aVR and V1 by Left Circumflex Artery OcclusionComisión Académica FCM - UNAHNo ratings yet
- DISCUDocument23 pagesDISCUpvsvrNo ratings yet
- Coronary Artery Calcification On CT Scanning PDFDocument7 pagesCoronary Artery Calcification On CT Scanning PDFfikriadityaNo ratings yet
- Spondilita Ankilozanta Cardio PulmonarDocument6 pagesSpondilita Ankilozanta Cardio PulmonarGiulia LungulescuNo ratings yet
- Calcium Overload-Induced Arrhythmia Is Suppressed by Farnesol in Rat HeartDocument13 pagesCalcium Overload-Induced Arrhythmia Is Suppressed by Farnesol in Rat HeartAdriana GuimarãesNo ratings yet
- T2 MRI and Myocardial Iron in Thalassemia (Pennell)Document6 pagesT2 MRI and Myocardial Iron in Thalassemia (Pennell)sachin s hiremathNo ratings yet
- Aortic Coarctation Cardiology Clinics 2020Document15 pagesAortic Coarctation Cardiology Clinics 2020Angela OrozcoNo ratings yet
- Abstracts / Atherosclerosis 252 (2016) E1 Ee196 E185Document2 pagesAbstracts / Atherosclerosis 252 (2016) E1 Ee196 E185MaulNo ratings yet
- Arritmias Ventriculares en Corazones NormalesDocument14 pagesArritmias Ventriculares en Corazones Normalessanalejo0290No ratings yet
- medip,+IJCMPH-10303+RDocument5 pagesmedip,+IJCMPH-10303+RaisyahhelmadevithalibNo ratings yet
- Agustus Monitoring HemodinamikDocument61 pagesAgustus Monitoring HemodinamikFikriYTNo ratings yet
- Vasospastic AnginaDocument10 pagesVasospastic AnginaSyadza FirdausiahNo ratings yet
- Heijman Et Al-2013-Acta Physiologica (Oxford, England)Document4 pagesHeijman Et Al-2013-Acta Physiologica (Oxford, England)an7li721No ratings yet
- Intra Cath ArrythemiasDocument17 pagesIntra Cath Arrythemiasmuath taaniNo ratings yet
- 247 FullDocument6 pages247 FullBryan FarrelNo ratings yet
- Characteristics of Left Ventricular Diastolic Dysfunction in The Community: An Echocardiographic SurveyDocument7 pagesCharacteristics of Left Ventricular Diastolic Dysfunction in The Community: An Echocardiographic SurveyPaul AsturbiarisNo ratings yet
- Percutaneous Coronary Intervention in A Patient With Severe Systemic Vasculitis and Myocardial InfarctionDocument4 pagesPercutaneous Coronary Intervention in A Patient With Severe Systemic Vasculitis and Myocardial Infarctionvam buddhaNo ratings yet
- Challenges and Opportunities in Improving Left VentricularDocument22 pagesChallenges and Opportunities in Improving Left VentricularGaal PinNo ratings yet
- J Ultrasmedbio 2018 02 013Document10 pagesJ Ultrasmedbio 2018 02 013Parlan SingodimejoNo ratings yet
- Adverse Diastolic Remodeling After Reperfused ST-elevation Myocardial Infarction: An Important Prognostic IndicatorDocument11 pagesAdverse Diastolic Remodeling After Reperfused ST-elevation Myocardial Infarction: An Important Prognostic IndicatorCatia MoraesNo ratings yet
- ECG Manifestations of Multiple Electrolyte Imbalance: Peaked T Wave To P Wave ("Tee Pee Sign")Document5 pagesECG Manifestations of Multiple Electrolyte Imbalance: Peaked T Wave To P Wave ("Tee Pee Sign")Mohammad AlzawiNo ratings yet
- AR Yang Komplikasi Menjadi Gagal Jantung PDFDocument5 pagesAR Yang Komplikasi Menjadi Gagal Jantung PDFFitriani AlawiyahNo ratings yet
- Li (2021) - Human RyR2 (Ryanodine Receptor 2) Loss-of-Function MutationsDocument12 pagesLi (2021) - Human RyR2 (Ryanodine Receptor 2) Loss-of-Function MutationsbalounovaNo ratings yet
- 58-63 DallAra JIC 2020 Feb WMDocument6 pages58-63 DallAra JIC 2020 Feb WMJose Manuel Ornelas-AguirreNo ratings yet
- Sudden Death and Ion Channel Disease: Pathophysiology and Implications For ManagementDocument10 pagesSudden Death and Ion Channel Disease: Pathophysiology and Implications For ManagementAndi Tiara S. AdamNo ratings yet
- Placa Femoral y CVDDocument10 pagesPlaca Femoral y CVDvascoNo ratings yet
- Hiperkalemia 1 PDFDocument5 pagesHiperkalemia 1 PDFablfilaNo ratings yet
- Acute Stroke AssessmentDocument7 pagesAcute Stroke AssessmentHanh NguyenNo ratings yet
- Relationship Between Electrocardiographic Characteristics of Left Bundle Branch Block and Echocardiographic FindingsDocument7 pagesRelationship Between Electrocardiographic Characteristics of Left Bundle Branch Block and Echocardiographic FindingsVlada SiricNo ratings yet
- Atwater 2020Document6 pagesAtwater 2020Vlada SiricNo ratings yet
- Perioperative ArrthymiasDocument9 pagesPerioperative ArrthymiasDrshoaib KhanNo ratings yet
- 2018 - Manifestaciones Electrocardiograficas de La Hiperkalemia SeveraDocument4 pages2018 - Manifestaciones Electrocardiograficas de La Hiperkalemia SeveraNANDY LUZ FERIA DIAZNo ratings yet
- Qader Othman 2019 J. Phys. Conf. Ser. 1294 062110Document11 pagesQader Othman 2019 J. Phys. Conf. Ser. 1294 062110GoranNo ratings yet
- Acute Kidney Injury in COVID-19: Emerging Evidence of A Distinct PathophysiologyDocument4 pagesAcute Kidney Injury in COVID-19: Emerging Evidence of A Distinct PathophysiologyxtineNo ratings yet
- Relation of Iron Status To Prognosis After Acute Coronary SyndromeDocument9 pagesRelation of Iron Status To Prognosis After Acute Coronary SyndromeselvianaNo ratings yet
- Long QT SyndromeDocument9 pagesLong QT SyndromeRoberto SalazarNo ratings yet
- Let's TwistDocument2 pagesLet's TwistMladenKocicaNo ratings yet
- Cardiac Electricians 2011Document8 pagesCardiac Electricians 2011Odessa FileNo ratings yet
- Pathologic Implications of Restored Positive T Waves and Persistent Negative T Waves After Q Wave Myocardial InfarctionDocument5 pagesPathologic Implications of Restored Positive T Waves and Persistent Negative T Waves After Q Wave Myocardial InfarctionABDULLAH ALHASANNo ratings yet
- Eurheartj/ehab 138Document11 pagesEurheartj/ehab 138ABDULLAH ALHASANNo ratings yet
- Simultaneous Occurrence of AF+AVLDocument11 pagesSimultaneous Occurrence of AF+AVLABDULLAH ALHASANNo ratings yet
- Nihms 396567Document13 pagesNihms 396567ABDULLAH ALHASANNo ratings yet
- Ddxnet: A Deep Learning Model For Automatic Interpretation of Electronic Health Records, Electrocardiograms and ElectroencephalogramsDocument11 pagesDdxnet: A Deep Learning Model For Automatic Interpretation of Electronic Health Records, Electrocardiograms and ElectroencephalogramsABDULLAH ALHASANNo ratings yet
- NIH Public AccessDocument14 pagesNIH Public AccessABDULLAH ALHASANNo ratings yet
- Jamaneurology Dolui 2022 Oi 220004 1649435699.28458Document10 pagesJamaneurology Dolui 2022 Oi 220004 1649435699.28458ABDULLAH ALHASANNo ratings yet
- An Interesting Case of "Trigeminal Tachycardia"Document3 pagesAn Interesting Case of "Trigeminal Tachycardia"ABDULLAH ALHASANNo ratings yet
- Updated Peer-Reviewed Medical Papers Submitted To Various MedicalDocument80 pagesUpdated Peer-Reviewed Medical Papers Submitted To Various MedicalJim Hoft100% (8)
- FundaDocument5 pagesFundaGreggy Francisco LaraNo ratings yet
- Change Theory Project: University of Texas at Arlington Leadership and Management N4455 By: Jordan GossageDocument16 pagesChange Theory Project: University of Texas at Arlington Leadership and Management N4455 By: Jordan GossageInna NaraievskaNo ratings yet
- Biostatistics Unit 5Document2 pagesBiostatistics Unit 5Joseph NjovuNo ratings yet
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- Sonosite Micromaxx Portable Color DopplerDocument4 pagesSonosite Micromaxx Portable Color DopplerSERVICIO TECNICONo ratings yet
- Use of Steroid OintmentsDocument6 pagesUse of Steroid OintmentsPal KuriaNo ratings yet
- NCM 109 (ECG and Cardiac Monitoring)Document7 pagesNCM 109 (ECG and Cardiac Monitoring)Kyla BungayNo ratings yet
- Vascular Technology 1000 Multiple Choice QuestionsDocument196 pagesVascular Technology 1000 Multiple Choice Questionssaimum9092% (13)
- Drug Study HemostanDocument2 pagesDrug Study HemostanMaria Leonie Dela CruzNo ratings yet
- Week 10 Lab Exercise - Cvs & Bood Vessels AnsDocument4 pagesWeek 10 Lab Exercise - Cvs & Bood Vessels AnsG4 AMOYO ANGELICA NICOLENo ratings yet
- Massive Transfusion - An Update For The Anesthesiologist 2017Document9 pagesMassive Transfusion - An Update For The Anesthesiologist 2017JOSENo ratings yet
- Incomplete Right Bundle Branch Block: Challenges in Electrocardiogram DiagnosisDocument7 pagesIncomplete Right Bundle Branch Block: Challenges in Electrocardiogram Diagnosisheni arisNo ratings yet
- 5 Min - Myocardial Strain AnalysisDocument26 pages5 Min - Myocardial Strain AnalysisAsim Kumar Biswas100% (1)
- Atrial Septal Defect: Presented By:-Dr Kunwar Sidharth SaurabhDocument60 pagesAtrial Septal Defect: Presented By:-Dr Kunwar Sidharth SaurabhKunwar Sidharth SaurabhNo ratings yet
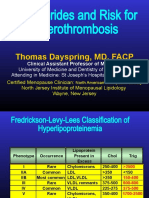
- Triglycerides and Risk For Atherothrombosis: Thomas Dayspring, MD, FACPDocument92 pagesTriglycerides and Risk For Atherothrombosis: Thomas Dayspring, MD, FACPيونس حسينNo ratings yet
- Lesson Plan MIDocument14 pagesLesson Plan MIAnand Bhawna100% (1)
- Role of The Physiotherapist in Cardiac Rehabilitation Document Version 4Document32 pagesRole of The Physiotherapist in Cardiac Rehabilitation Document Version 4Irene Chrysovalanto Themistocleous67% (3)
- 23 Mock CodesDocument56 pages23 Mock Codesmaguisssa100% (4)
- Pharmacology OF Anti-Hypertensive: Siti SyarifahDocument38 pagesPharmacology OF Anti-Hypertensive: Siti SyarifahAnnurul Badry IINo ratings yet
- Comparison of The Effects of Nebivolol and Bisoprolol On Systematic Vascular Resistance in Patients With Essential HypertensionDocument15 pagesComparison of The Effects of Nebivolol and Bisoprolol On Systematic Vascular Resistance in Patients With Essential HypertensionSherif KamalNo ratings yet
- Mechanical Thrombectomy For Acute Ischemic StrokeDocument19 pagesMechanical Thrombectomy For Acute Ischemic StrokeCarlos Alfredo Vargas QuinteroNo ratings yet
- Tachycardia AlgorithmDocument1 pageTachycardia AlgorithmGideon BahuleNo ratings yet
- POCUS in ChildrenDocument13 pagesPOCUS in ChildrenISELENE MARIANo ratings yet
- Myocardial Infarction (MI)Document23 pagesMyocardial Infarction (MI)Abedin Mehmedovic88% (60)
- Thrombosis Research: Full Length ArticleDocument6 pagesThrombosis Research: Full Length ArticleCarol GomezNo ratings yet
- A Study To Assess The Effectiveness of Amla Juice With Honey To Reduce The Blood Pressure Level Among Hypertension Patients in Selected Urban AreaDocument8 pagesA Study To Assess The Effectiveness of Amla Juice With Honey To Reduce The Blood Pressure Level Among Hypertension Patients in Selected Urban AreaResearch ParkNo ratings yet
- Approach To PalpitationsDocument2 pagesApproach To PalpitationsNicole Xyza JunsayNo ratings yet
- Assessment of Chest PainDocument59 pagesAssessment of Chest PainMaria GarabajiuNo ratings yet
- Drug Name Mode of Action Indications Contraindications Side Effects/ Advserse Effects (Specify) Nursing InterventionsDocument4 pagesDrug Name Mode of Action Indications Contraindications Side Effects/ Advserse Effects (Specify) Nursing InterventionsKaterina Petrova100% (1)