You might also like
- Circulatory System: A Tutorial Study GuideFrom EverandCirculatory System: A Tutorial Study GuideRating: 5 out of 5 stars5/5 (3)
- The Jejunoileum: Anatomy The Abdomen Small and Large IntestineDocument7 pagesThe Jejunoileum: Anatomy The Abdomen Small and Large IntestineWaeel AbdullatifNo ratings yet
- Esophageal SurgeryDocument11 pagesEsophageal Surgerydr_kumananNo ratings yet
- Colon Benign Conditions - Surgery NotesDocument85 pagesColon Benign Conditions - Surgery NotesNagulan ChanemougameNo ratings yet
- Anatomy of Esophagus and StomachDocument65 pagesAnatomy of Esophagus and Stomachmackiecc100% (2)
- IntestinesDocument56 pagesIntestinesShimmering MoonNo ratings yet
- Clinical Anatomy of The Esophagus and StomachDocument82 pagesClinical Anatomy of The Esophagus and StomachmackieccNo ratings yet
- 3.digestive SystemDocument103 pages3.digestive Systemokoti.omutanyi22No ratings yet
- My StomachDocument24 pagesMy StomachPriya GKNo ratings yet
- Small Intestine AnatomyDocument4 pagesSmall Intestine AnatomyMaria Natalie IrwandaNo ratings yet
- Factors Affecting Clinical Outcomes Among Patients With Esophageal Varices BleedingDocument16 pagesFactors Affecting Clinical Outcomes Among Patients With Esophageal Varices BleedingMohamed ZezoNo ratings yet
- SURGERY - 1.5 Colon, Rectum, and Anus (Lecture)Document8 pagesSURGERY - 1.5 Colon, Rectum, and Anus (Lecture)Bianca Jane Maaliw100% (1)
- Unit 4 ReviewDocument53 pagesUnit 4 ReviewRoberta BansahNo ratings yet
- Post-Graduate Medical: JournalDocument5 pagesPost-Graduate Medical: JournallynaayusofNo ratings yet
- Anatomy and Physiology of RectumDocument5 pagesAnatomy and Physiology of RectumDoreen Claire M. WallangNo ratings yet
- 3.1 Anterior Abdominal Wall (Bea)Document5 pages3.1 Anterior Abdominal Wall (Bea)Norjetalexis CabreraNo ratings yet
- 18 IntestinesDocument28 pages18 Intestinesafzal sulemaniNo ratings yet
- The Boundaries of The Anterior Abdominal WallDocument63 pagesThe Boundaries of The Anterior Abdominal WallbeeNo ratings yet
- The Boundaries of The Anterior Abdominal Wall AreDocument62 pagesThe Boundaries of The Anterior Abdominal Wall ArebeeNo ratings yet
- ANAPHYG2Document8 pagesANAPHYG2Sam PenadosNo ratings yet
- OesophagusDocument3 pagesOesophagusХина КападиаNo ratings yet
- Bab IDocument9 pagesBab II Wayan Rendi AwendikaNo ratings yet
- The Abdominal AortaDocument9 pagesThe Abdominal AortaJuan Jose LeonNo ratings yet
- Digestive System: Digestive Glands. Alimentary CanalDocument27 pagesDigestive System: Digestive Glands. Alimentary CanalAnkit NariyaNo ratings yet
- Anatomy of The Rectum and Anal Canal: The Rectum Is The Part of The Colon Between The Sigmoid ColonDocument25 pagesAnatomy of The Rectum and Anal Canal: The Rectum Is The Part of The Colon Between The Sigmoid ColonJoy GhoseNo ratings yet
- 3 RD ENGDocument25 pages3 RD ENGVkcegcaNo ratings yet
- 14 StomachDocument24 pages14 Stomachafzal sulemaniNo ratings yet
- Structures of The ForegutDocument13 pagesStructures of The ForegutJatan KothariNo ratings yet
- Esophagus: Pipe or Gullet, Is An Organ in Vertebrates Through Which Food PassesDocument12 pagesEsophagus: Pipe or Gullet, Is An Organ in Vertebrates Through Which Food PassesCrow LordNo ratings yet
- Anatomy of Digestive SystemDocument20 pagesAnatomy of Digestive Systemolive jollyNo ratings yet
- Abdominal CavityDocument85 pagesAbdominal CavityMac HaNo ratings yet
- The AbdomenDocument2 pagesThe Abdomenrubie ann tillorNo ratings yet
- The Digestive System 3Document4 pagesThe Digestive System 3geniusgurl91No ratings yet
- Lecture 4Document14 pagesLecture 4X RamboNo ratings yet
- Anatomy of The KidneyDocument2 pagesAnatomy of The KidneychinecheremnfNo ratings yet
- Anatomy Abdominal Wall ThorekDocument26 pagesAnatomy Abdominal Wall ThorekAlna Shelah IbañezNo ratings yet
- Lecture 2 - Anatomy of The Ureters, Bladder and UrethraDocument7 pagesLecture 2 - Anatomy of The Ureters, Bladder and UrethraNatalie LiNo ratings yet
- RectumDocument43 pagesRectummidhunramesh007100% (4)
- Marking Scheme For Ant 414 (Functional Anatomy of Abdomen, Pelvis and Perineum) For 2017/2018 SessionDocument5 pagesMarking Scheme For Ant 414 (Functional Anatomy of Abdomen, Pelvis and Perineum) For 2017/2018 SessionmomoduNo ratings yet
- Anorectal Anatomy & Surgical ManagementDocument164 pagesAnorectal Anatomy & Surgical Managementsgod34No ratings yet
- UNIT 9 (Digestive System)Document8 pagesUNIT 9 (Digestive System)Workinesh Kaynabo KambaloNo ratings yet
- Abdominal Visceral OrgansDocument5 pagesAbdominal Visceral OrgansYudi Kelsi KaharapNo ratings yet
- Ac 2Document104 pagesAc 2saide limNo ratings yet
- Chapter I-V-1-Anatomy-Dr-Mark-MakaryDocument17 pagesChapter I-V-1-Anatomy-Dr-Mark-MakaryMark MakaryNo ratings yet
- Anatomy and Physiology of Colon of Case StudyDocument4 pagesAnatomy and Physiology of Colon of Case StudySimran JosanNo ratings yet
- Anatomi Fisiologi Dada AbdomenDocument16 pagesAnatomi Fisiologi Dada AbdomenemiliatamaraNo ratings yet
- Anatomy of UreterDocument19 pagesAnatomy of Ureterfabunmiopeyemiv23No ratings yet
- 323 Lecture 11Document45 pages323 Lecture 11Philip GituriNo ratings yet
- Lecture 5 Serous Sacs, Features and FunctionsDocument7 pagesLecture 5 Serous Sacs, Features and Functionssomebody_maNo ratings yet
- Stomach and Duodenum 10-27Document32 pagesStomach and Duodenum 10-27Ditas ChuNo ratings yet
- ССС 2019Document83 pagesССС 2019bekafop813No ratings yet
- Anatomy SpleenDocument32 pagesAnatomy SpleenBijo K BennyNo ratings yet
- Tugas Mandiri FloDocument24 pagesTugas Mandiri FloDom TorettoNo ratings yet
- 5.2 AbdomenDocument4 pages5.2 Abdomensaxman011No ratings yet
- Anatomy of OesophagusDocument25 pagesAnatomy of OesophagusRabi SyedNo ratings yet
- Anatomy of StomachDocument4 pagesAnatomy of StomachIntan Putri Maisarah100% (1)
- iNTERNAL oRGANSDocument92 pagesiNTERNAL oRGANSönemsiz biriNo ratings yet
- Anatomy of The Abdomen: Dr. Ahmad Kamil Shahwan Ph.D. General SurgeryDocument87 pagesAnatomy of The Abdomen: Dr. Ahmad Kamil Shahwan Ph.D. General SurgeryDaniel SitungkirNo ratings yet
- Journal of Entomology and Zoology Volume Eleven, Number Two, June 1919From EverandJournal of Entomology and Zoology Volume Eleven, Number Two, June 1919No ratings yet
- Qualtative ResearchDocument53 pagesQualtative ResearchIbtehal HasanNo ratings yet
- PBL Problem 1 Unit IV Week 1Document4 pagesPBL Problem 1 Unit IV Week 1Ibtehal HasanNo ratings yet
- Summar Resaerch ArticlesDocument1 pageSummar Resaerch ArticlesIbtehal HasanNo ratings yet
- Oral ExaminationDocument5 pagesOral ExaminationIbtehal HasanNo ratings yet
- Summar Resaerch ArticlesDocument1 pageSummar Resaerch ArticlesIbtehal HasanNo ratings yet
- Lecture Scanners FT v4Document75 pagesLecture Scanners FT v4Ibtehal HasanNo ratings yet
- Effect of Orofacial Myofunctional Exercise Using An Oral Rehabilitation Tool On Labial Closure Strength, Tongue Elevation Strength and Skin ElasticityDocument4 pagesEffect of Orofacial Myofunctional Exercise Using An Oral Rehabilitation Tool On Labial Closure Strength, Tongue Elevation Strength and Skin ElasticityUniversity Malaya's Dental Sciences ResearchNo ratings yet
- PAPER (ENG) - Swallowing Disturbance Questionnaire For Detecting DysphagiaDocument5 pagesPAPER (ENG) - Swallowing Disturbance Questionnaire For Detecting DysphagiaAldo Hip NaranjoNo ratings yet
- GastrointestinalDocument39 pagesGastrointestinalالمسوول الاعلاميNo ratings yet
- Rehabilitation of Glossectomy Cases With Tongue Prosthesis: A Literature ReviewDocument4 pagesRehabilitation of Glossectomy Cases With Tongue Prosthesis: A Literature ReviewmujtabaNo ratings yet
- Wei Mai (Parte 2) - Yin Wei MaiDocument15 pagesWei Mai (Parte 2) - Yin Wei MaiAlexandre HenriquesNo ratings yet
- Progressive Balbar Palsy: Dr. Mohamed Ali 3 Year MD IM ResidentDocument15 pagesProgressive Balbar Palsy: Dr. Mohamed Ali 3 Year MD IM ResidentMohamed AliNo ratings yet
- 11 PharynxDocument8 pages11 PharynxNur Ain Faezah RoslanNo ratings yet
- 4.3 Swallowing - Center - Concepts - and - ProceduresDocument7 pages4.3 Swallowing - Center - Concepts - and - Proceduresluribe662No ratings yet
- Dysphagia From A Neurogeriatric Point of ViewDocument6 pagesDysphagia From A Neurogeriatric Point of ViewVanessaCarrilloNo ratings yet
- Chapter 7 - The Digestive SystemDocument65 pagesChapter 7 - The Digestive SystemLama AlqarniNo ratings yet
- Canine and Feline Mega EsophagusDocument10 pagesCanine and Feline Mega Esophagustaner_soysurenNo ratings yet
- Dysphagia Management of Pediatric Patients With Cerebral PalsyDocument17 pagesDysphagia Management of Pediatric Patients With Cerebral PalsyDaniela AdarosNo ratings yet
- NCP GoiterDocument2 pagesNCP GoiterShaira De La CruzNo ratings yet
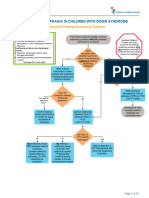
- Aspiration and Dysphagia in Children With Down SyndromeDocument23 pagesAspiration and Dysphagia in Children With Down SyndromeJessa MaeNo ratings yet
- Digestive SystemDocument60 pagesDigestive SystemdrynwhylNo ratings yet
- Videofluoroscopic Swallowing StudiesDocument25 pagesVideofluoroscopic Swallowing StudiesPriisciilla Vicencio100% (1)
- Git PhysioDocument102 pagesGit PhysioPahw BaluisNo ratings yet
- Table of Head and Neck MusclesDocument5 pagesTable of Head and Neck Musclesororoangel0% (1)
- 2007 CASLPA Position Paper On Dysphagia in AdultsDocument8 pages2007 CASLPA Position Paper On Dysphagia in AdultsEva Sala RenauNo ratings yet
- LX Suspension and UES Myotomy Kos 2008Document7 pagesLX Suspension and UES Myotomy Kos 2008DEVNo ratings yet
- Pemicu 1 Blok GIT: Theffany 405120198 Fakultas Kedokteran Universitas TarumanagaraDocument99 pagesPemicu 1 Blok GIT: Theffany 405120198 Fakultas Kedokteran Universitas TarumanagaraTheffany KasiranNo ratings yet
- GIT NotesDocument23 pagesGIT NotesGrey SyNo ratings yet
- Anatomy & Physiology of PharynxDocument22 pagesAnatomy & Physiology of PharynxArvind SangaviNo ratings yet
- Swallowing Analyses of Neonates and Infants in Breastfeeding and Bottle-Feeding: Impact On Video Uoroscopy Swallow StudiesDocument11 pagesSwallowing Analyses of Neonates and Infants in Breastfeeding and Bottle-Feeding: Impact On Video Uoroscopy Swallow Studiesantonio gabriel egea castilloNo ratings yet
- Abnormal Swallow Infantile and AdultDocument2 pagesAbnormal Swallow Infantile and Adultfinix33No ratings yet
- Bingo Cards 2x2Document5 pagesBingo Cards 2x2Marta Pérez MadridNo ratings yet
- NCP On SahDocument21 pagesNCP On SahDr-Sanjay SinghaniaNo ratings yet
- Speech and Language Therapy Exercises - vn2 A5Document8 pagesSpeech and Language Therapy Exercises - vn2 A5Mian Imran IqbalNo ratings yet
- Dysphagia Diagnosis 1and Treatment (Olle Ekberg) (Z-Lib - Org) (1) - 83-284Document202 pagesDysphagia Diagnosis 1and Treatment (Olle Ekberg) (Z-Lib - Org) (1) - 83-284Macarena Paz ÁlvarezNo ratings yet
- DysphagiaDocument8 pagesDysphagiaDini MarsyaNo ratings yet