You might also like
- Technical Guidelines on Rapid Risk Assessment for Animal Health ThreatsFrom EverandTechnical Guidelines on Rapid Risk Assessment for Animal Health ThreatsNo ratings yet
- Falls Risk Assessment ToolDocument3 pagesFalls Risk Assessment ToolBabyna Mozez Iiaa ReztieNo ratings yet
- Disease Control Priorities, Third Edition (Volume 3): CancerFrom EverandDisease Control Priorities, Third Edition (Volume 3): CancerNo ratings yet
- Fall Risk Assessment FormDocument3 pagesFall Risk Assessment FormMichael Silva100% (1)
- The Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsFrom EverandThe Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsNo ratings yet
- Capacity Development Needs Assessment QuestionnaireDocument12 pagesCapacity Development Needs Assessment QuestionnaireAndres OrtizNo ratings yet
- Acute Coronary Syndrome - Antithrombotic Therapy and Secondary PreventionFrom EverandAcute Coronary Syndrome - Antithrombotic Therapy and Secondary PreventionNo ratings yet
- Inpatient Treatment Order - Level 2 - : (MRMHA-D)Document2 pagesInpatient Treatment Order - Level 2 - : (MRMHA-D)prabhaNo ratings yet
- Veterinary Public Health & Epidemiology Veterinary Public Health - Epidemiology-Zoonosis-One HealthDocument433 pagesVeterinary Public Health & Epidemiology Veterinary Public Health - Epidemiology-Zoonosis-One HealthdracvmedicineNo ratings yet
- Treatment Protocols 2016Document209 pagesTreatment Protocols 2016NanaNo ratings yet
- Admissions Medical ApplicationDocument2 pagesAdmissions Medical ApplicationkesnaNo ratings yet
- Admissions Medical ApplicationDocument2 pagesAdmissions Medical ApplicationDajueNo ratings yet
- International Parkinson and Movement Disorder Society - Non-Motor Rating ScaleDocument12 pagesInternational Parkinson and Movement Disorder Society - Non-Motor Rating ScaleNeurologia homicNo ratings yet
- Practical Guide to School Crisis PlanningDocument132 pagesPractical Guide to School Crisis PlanningAnemoessaNo ratings yet
- PDAC - DSaRM 11022018 FDABackgrounderDocument33 pagesPDAC - DSaRM 11022018 FDABackgrounderBianca AlinaNo ratings yet
- Public Health Assessment Guidance Manual UpdateDocument357 pagesPublic Health Assessment Guidance Manual UpdateAbhishek SahuNo ratings yet
- Nejmoa1208394 AppendixDocument81 pagesNejmoa1208394 Appendixadee04No ratings yet
- Pfizer-Biontech COVID-19 Vaccine Briefing DocumentDocument92 pagesPfizer-Biontech COVID-19 Vaccine Briefing DocumentDavid CaplanNo ratings yet
- Encyclopedia BD Income-Associated BDDocument15 pagesEncyclopedia BD Income-Associated BDPeter MuennigNo ratings yet
- Hira 2014 08 20 PDFDocument24 pagesHira 2014 08 20 PDFSADHEDNo ratings yet
- Medication Error Report FormDocument2 pagesMedication Error Report FormAhmad TaramsyNo ratings yet
- Adverse Reaction Reporting FormDocument1 pageAdverse Reaction Reporting FormAshutosh SharmaNo ratings yet
- Attach 5 Falls Risk Assessment FormDocument4 pagesAttach 5 Falls Risk Assessment FormEko Wahyu AgustinNo ratings yet
- Hankin Ozon GeneratorDocument26 pagesHankin Ozon GeneratormilenkovicnNo ratings yet
- Health and Health Related Indicators 2013 EFYDocument61 pagesHealth and Health Related Indicators 2013 EFYRedietNo ratings yet
- Corticosteroids For The Prevention and Treatment of Postextubation Stridor in Neonates, Children and AdultsDocument34 pagesCorticosteroids For The Prevention and Treatment of Postextubation Stridor in Neonates, Children and AdultscarlospinopedNo ratings yet
- Standardised Categories and Indicators For Better Cmam Reporting Final Apr 2015Document44 pagesStandardised Categories and Indicators For Better Cmam Reporting Final Apr 2015Md. Rafiqul IslamNo ratings yet
- HAZOP RISK CHARACTERIZATION and TemplateDocument3 pagesHAZOP RISK CHARACTERIZATION and Templatekphk1979100% (1)
- Emergency Medical Services Pre Hospital Treatment Protocols Version 2019 2 Effective 100119Document231 pagesEmergency Medical Services Pre Hospital Treatment Protocols Version 2019 2 Effective 100119Kyle ChenNo ratings yet
- PTSD On MilitaryDocument19 pagesPTSD On Militaryayu yuliantiNo ratings yet
- Emergency Department Trends From The Drug Abuse Warning Network, Final Estimates 1994-2001Document142 pagesEmergency Department Trends From The Drug Abuse Warning Network, Final Estimates 1994-2001losangelesNo ratings yet
- Procedure for Hazard Risk Assessment and Control DeterminationDocument5 pagesProcedure for Hazard Risk Assessment and Control DeterminationSamsu SamsNo ratings yet
- Working Group Report On Sea LiceDocument117 pagesWorking Group Report On Sea LiceJon Arne GrøttumNo ratings yet
- A. Spinks Et Al - Scopolamine (Hyoscine) For Preventing and Treating Motion Sickness (Review)Document31 pagesA. Spinks Et Al - Scopolamine (Hyoscine) For Preventing and Treating Motion Sickness (Review)LonkesNo ratings yet
- BRM Psy V11P1Document10 pagesBRM Psy V11P1simbawulaNo ratings yet
- Induced Termination of Pregnancy (ITOP) Reporting System GuideDocument36 pagesInduced Termination of Pregnancy (ITOP) Reporting System GuideYiddy Kester Vilchez ArellanosNo ratings yet
- Statistical Analysis On Risk Factors of Prevalence of Malaria in Z/ Dugda Woreda, Oromia, East ArsiDocument31 pagesStatistical Analysis On Risk Factors of Prevalence of Malaria in Z/ Dugda Woreda, Oromia, East Arsitewodrosmolalign19No ratings yet
- 6 Tratamiento Del RiesgoDocument15 pages6 Tratamiento Del RiesgoIVAN OVIEDONo ratings yet
- CD 013130Document18 pagesCD 013130Deedee RenovaldiNo ratings yet
- Screening and Case Finding Instruments For Depression (Review)Document34 pagesScreening and Case Finding Instruments For Depression (Review)Felipe Andrés Ponce CorreaNo ratings yet
- Perfilestoxicologicos PDFDocument666 pagesPerfilestoxicologicos PDFHector GonzalezNo ratings yet
- CDP FullReport Mar06Document222 pagesCDP FullReport Mar06Amit Abhishek TopnoNo ratings yet
- Risk Management Plan TemplateDocument17 pagesRisk Management Plan Templaterafael.binder86% (7)
- NR - EUA 27034.132 Review Memo Pfizer-BioNTech COVID-19 Vaccine - REVISED24May - Final - 0Document43 pagesNR - EUA 27034.132 Review Memo Pfizer-BioNTech COVID-19 Vaccine - REVISED24May - Final - 0Linda JohnsonNo ratings yet
- Lab Risk AssessmentDocument8 pagesLab Risk Assessmentaqilah haronNo ratings yet
- Noh2016 PDFDocument149 pagesNoh2016 PDFSef MartinezNo ratings yet
- What Are The Psychological Effects of Disaster Work On An Emergency Manager?Document13 pagesWhat Are The Psychological Effects of Disaster Work On An Emergency Manager?api-525064413No ratings yet
- Follow-Up BlankDocument2 pagesFollow-Up BlankAflkjael JamaelNo ratings yet
- Case PresentationDocument2 pagesCase Presentationalalrashidi1No ratings yet
- 808 - 204447 Vortioxetine Unireview Prea - 0Document95 pages808 - 204447 Vortioxetine Unireview Prea - 0Dr Meenakshi ParwaniNo ratings yet
- Risk Assessment My GardenDocument2 pagesRisk Assessment My GardenMatthew BaguleyNo ratings yet
- Interventions For Dissociated Vertical Deviation (Review) : CochraneDocument37 pagesInterventions For Dissociated Vertical Deviation (Review) : CochraneMacarena AlvarezNo ratings yet
- Risk Assessment LRCDocument3 pagesRisk Assessment LRCChloe PeacockNo ratings yet
- Form Laporan Insiden InternalDocument7 pagesForm Laporan Insiden InternalYuliana LopeNo ratings yet
- VAD Vesikari Scoring ManualDocument51 pagesVAD Vesikari Scoring Manualmuhamad mukhtarNo ratings yet
- Draft Rapport ARC-D MIHR Mali 14 04 2023 en-USDocument45 pagesDraft Rapport ARC-D MIHR Mali 14 04 2023 en-USOumar TOGOLANo ratings yet
- Chest Stabbing DiagnosisDocument11 pagesChest Stabbing DiagnosisMustafa100% (1)
- 1 Medical Board Format ESE 091216Document6 pages1 Medical Board Format ESE 091216ryy38480No ratings yet
- RiskTreatmentPlanTemplate ISO27001Document15 pagesRiskTreatmentPlanTemplate ISO27001Yulian SaniNo ratings yet
- Guideline AAP DMDDocument2 pagesGuideline AAP DMDarifNo ratings yet
- Plain Film and HRCT Diagnosis of Interstitial Lung Disease: Sujal R. Desai, Helmut Prosch, and Jeffrey R. GalvinDocument9 pagesPlain Film and HRCT Diagnosis of Interstitial Lung Disease: Sujal R. Desai, Helmut Prosch, and Jeffrey R. GalvinVictor ChiabaiNo ratings yet
- TOG Human Parvo B19Document6 pagesTOG Human Parvo B19MarNo ratings yet
- Etats-Unis//Rapport Septembre 2019/criminal Victimization, 2018Document37 pagesEtats-Unis//Rapport Septembre 2019/criminal Victimization, 2018Sebastien de Lyon100% (1)
- Clinical Pharmacy Therapeu - 2016 - Gunter - Non Steroidal Anti Inflammatory Drug Induced Cardiovascular Adverse Events ADocument12 pagesClinical Pharmacy Therapeu - 2016 - Gunter - Non Steroidal Anti Inflammatory Drug Induced Cardiovascular Adverse Events AYuan TamaraNo ratings yet
- Optima Secure Plan HDFC ERGODocument6 pagesOptima Secure Plan HDFC ERGOStar JasmineNo ratings yet
- Right Lower Quadrant PainDocument19 pagesRight Lower Quadrant PainSohaib Mohammad KhanNo ratings yet
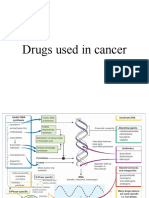
- Drugs Used in CancerDocument46 pagesDrugs Used in CancerRENTI NOVITANo ratings yet
- Ru 58 42150Document12 pagesRu 58 42150Efen YtNo ratings yet
- ASSSSDocument21 pagesASSSSACERET, IVAN LAURENTINE G.No ratings yet
- Botox For SyringomaDocument3 pagesBotox For SyringomaAdi WijayantoNo ratings yet
- JGeriatrMentHealth2130-4603396 124713Document8 pagesJGeriatrMentHealth2130-4603396 124713Bruno Déo de OliveiraNo ratings yet
- NCM 109 Reviewer 2Document13 pagesNCM 109 Reviewer 2Jerick PapoloniasNo ratings yet
- Newborn Screening StudentDocument39 pagesNewborn Screening StudentKeanu Win CatipayNo ratings yet
- Comprehensive Geriatric Assessment - MPGIDocument16 pagesComprehensive Geriatric Assessment - MPGIEric James ManuelNo ratings yet
- Practice Exam in Nursing Set ADocument38 pagesPractice Exam in Nursing Set AGo IdeasNo ratings yet
- Enterocutaneous FistulaDocument37 pagesEnterocutaneous FistulaAdityadewi SulistyoNo ratings yet
- Ear Pain in Children Up To DateDocument25 pagesEar Pain in Children Up To DateNicole Marie NicolasNo ratings yet
- Diabetes (Revision)Document10 pagesDiabetes (Revision)กฤติน วนิจวรางกุลNo ratings yet
- Tot TCM in Pain Management.v1 2018Document41 pagesTot TCM in Pain Management.v1 2018AHNo ratings yet
- Assessment Questions - Fungal DiagnosticsDocument3 pagesAssessment Questions - Fungal Diagnosticsapi-647779956No ratings yet
- Annual Medical Report FormDocument8 pagesAnnual Medical Report Formromulo anascoNo ratings yet
- Q3 Health 8 Module 3 PDFDocument13 pagesQ3 Health 8 Module 3 PDFkateNo ratings yet
- Pre Term Labor Case Scenario GRP ADocument5 pagesPre Term Labor Case Scenario GRP AJR Rolf NeuqeletNo ratings yet
- 2018:19 Crime StatsDocument220 pages2018:19 Crime StatsBusinessTech64% (14)
- High Risk PregnancyDocument2 pagesHigh Risk PregnancyDianeNo ratings yet
- DR McDaniel PSYC 3023 Abnormal Psych FA 21 Chapter 8 Dissociative POSTDocument27 pagesDR McDaniel PSYC 3023 Abnormal Psych FA 21 Chapter 8 Dissociative POSTHeather JenkinsNo ratings yet
- Research ArticleDocument17 pagesResearch ArticleAdil JDNo ratings yet
- Venipuncture ComplicationsDocument21 pagesVenipuncture ComplicationsKeren Nathaniel Alvarado100% (1)
- Acute appendicitis symptoms and diagnosisDocument51 pagesAcute appendicitis symptoms and diagnosisALok Kumar100% (1)