Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Dental Fluorosis: Management from the Least to the
Most Invasive Treatment, Based on a Series of
Clinical Cases
Mejri.O1, Hammouda.L2, Kalghoum.I1, Gurgel-Georgelin.M3,4, Canceill.T3,4, Hadyaoui.D1, Diemer.F3,4
1Department of Fixed Prosthodontics, Research Laboratory of Occlusodontic and Ceramic Prostheses LR16ES15,
Faculty of Dental Medicine, University of Monastir, Tunisia;
2
Dental Faculty of Monastir, Research Laboratory LR12ES11, University of Monastir, Tunisia;
3
UFR d’Odontologie et CHU de Toulouse
4
INSERM U1048; Institut des Maladies Métaboliques et Cardiovasculaires (I2MC), équipe INCOMM, Toulouse
Abstract :- Dental fluorosis is a dental pathology caused South-West (Gafsa, Sidi Bouzid, Mednine...) constitutes a
by excessive ingestion of fluoride during the first years of very rich zone in fluoride with a content higher than 6 ppm.
life. Excess of fluoride will thus disrupt the normal (45)
formation of enamel crystals during amelogenesis and
lead to the formation of an often unsightly porous Excessive intake of fluoride for several months or
enamel. The degree of severity of fluorosis can be years during the period of tooth formation (between birth
established precisely using different classifications and and 8 years, the age at which enamel formation is complete)
depends on the ingested dose, the frequency of ingestion, can cause a pathology called "fluorosis". The latter is one of
the age of the subject and individual variability. The the syndromes of chronic fluoride intoxication with bone
reason for consultation of patients with fluorosis is and/or dental lesions. (3)
mainly aesthetic. The choice of treatment was based on
the stage of fluorosis. There are currently very Excessive concentrations of fluoride can disturb the
conservative therapies such as whitening or micro- functioning of the cells responsible for the formation of
abrasion, which can effectively treat mild or even enamel (ameloblasts), which prevents the proper maturation
moderate fluorosis. Treatment with bonded ceramic of the enamel. It is clinically manifested by a dyschromia,
veneers or full-coverage prostheses is only indicated for symmetry of lesions and sometimes porosities (4)
cases of moderate and severe fluorosis because of their
aesthetic interest and their mechanical and biological Ludmila Manuila, Pierre Lewalle (2004, the medical
properties. It will therefore be appropriate for the dictionary): "Dental fluorosis, due to the consumption of
partitionner to make a precise diagnosis and to choose water that is too rich in fluoride, is manifested by white and
the best suited therapy to his patient. brown spots on the enamel, which are irreversible". (5/6)
Our papier will present and discuss 3 clinical cases There are major classifications that will allow to
about the managment of dental fluorosis. establish with precision the degree of damage of the dental
surfaces : Dean's index and Thylstrup Fejerskov's index.
Keywords:- Fluorosis, Therapeutic Gradient, Whitening, (7/8)
Micro Abrasion, Ceramic Veneer, Crown. Dean's classification is the oldest classification (1942)
but is still in practice today. This classification is employed
I. INTRODUCTION by the WHO and applied clinically to define the clinical
aspects of fluorosis. The patient's score is based on the two
Fluoride is a natural mineral element that is essential. It most severely affected teeth. If two teeth have different
is used since the 1940s for its cario-protective action and is degrees of disease, the score of the less affected tooth is
recognized as the main factor responsible for the spectacular used.
decrease in the prevalence of dental caries observed in the
world. (1/2) It has six levels, which classify the occurrence of
fluorosis from "normal" to "severe" (9) :
The sources of fluoride are multiple. It can be through
systemic way, such as, the drinking water, the fluorinated *Score 0 : Normal : The enamel is translucent. The
milk, the salt... Or topical way, such as, the toothpaste, the dental surface is smooth and shiny. The shade is normal
fluorinated varnish, the mouthwash, and the fluorinated and uniform.
Gels. (3) Score 1: Fluorosis questionable, doubtful : The enamel
shows some small defects of translucency (occasional
In Tunisia, drinking water naturally contains in some small white spots).
regions, high or average doses of fluoride. The region of
IJISRT23AUG1121 www.ijisrt.com 2251
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
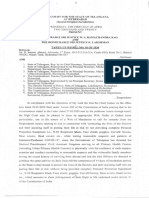
Score 2: Fluorosis very mild, very low : Small opaque into account his health and financial conditions. The
white areas are irregularly distributed on the enamel clinical examination was performed on clean and dry teeth
surface represent less than 25% of the surface of the with adequate lighting. It showed the absence of carious
tooth concerned. lesions and cracks. The brown spots are generalized, with
Score 3: Mild, low fluorosis: The white opaque areas of the form of horizontal lines bilateral and symmetrical to the
enamel are more extensive but do not represent more midline. The shape of the teeth remained unchanged. (figure
than 50% of the tooth surface 1.a). We established the diagnosis of moderate dental
Score 4: Fluorosis moderate : All enamel surfaces are fluorosis of Dean’s index 4.
affected but the shape of the teeth remains unchanged.
Brown stains may be present. After a discussion with the patient, a microabrasion
Score 5: Severe fluorosis: All enamel surfaces are treatment with Opalustre® (figure 1.b) was proposed.
affected. Hypoplasia is so marked that the shape of the Following his agreement, we started by applying a layer of
tooth may be altered. Brown stains are widespread. abrasive mixture (2mm) on the vestibular surfaces of the
Incisal edges and occlusal surfaces are abraded. teeth (figure 1.c). Circular movements were performed
with a rubber prophy cup (Opalustre®) for 5 to 10 seconds
The purpose of this article is to present the different followed with rinsing, for each cycle (figure 1.c-d).
techniques for the management of dental fluorosis through a
series of clinical cases. After 5 application cycles, an evaluation of the
situation was carried out. A decrease in the saturation of the
Clinical Cases : brownish color of the stains, and a harmonization of the hue
were noted. After that, we made the application of a fluoride
Clinical Case n°1 gel 2%, for 4 to 5 minutes with the polishing cup
A 27 year old man (M.H), non-smoker, from Tataouine (Opalustre®), to remineralize the surface of the tooth and
(South West of Tunisia), was referred to the prosthetic provide postoperative sensitivity (figure 1.e). Photographs
department in the dental clinic of Monastir , expressing were taken after a micro-abrasion session (Figure 1.f), and
dissatisfaction with the appearance of his smile. He wanted after 6 months of follow-up (figure 1.g).
to solve his aesthetic problem as soon as possible and to take
Fig 1 Treatment of a Moderate Fluorosis Index 4 of Dean by Micro-Abrasion
IJISRT23AUG1121 www.ijisrt.com 2252
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Clinical Case n°2 : The mock-up has been realized from a digital wax up
A 26-healthy patient (T.B), from Sidi-Bouzid (South- using the direct self-molding technique (figure 2.e). A
West of Tunisia), was consulted for an aesthetic problem in silicone key (mask) is loaded with an injectable self-
our department of fixed prosthesis in Monastir, suffering polymerizing acrylic resin (Protemp®), (figure 3.f). The
from generalized brown spots with a sensitivity to cold. The preparations were made according to the technique of butt
clinical examination shows the absence of carious lesions margin (figure 2.g-h). The choice of the shade of the
and restorations. All enamel surfaces were affected by ceramic veneers was made on the chair, respecting the
brown stains. During the smile, the patient discovers from patient’s requests.
the right first premolar to the left first premolar. The enamel
hypoplasia was so marked that the shape of the teeth was Then, a digital impression was made with an intra-oral
altered. Pits were marked by a hooking of the probe. The optical camera directly in the mouth (3 Shape) (figure 2.i).
simple passage by a probe N°17, on the vestibular faces, In the laboratory, the dental technician designs and
gene the patient. The incisal edges and occlusal surfaces are manufactures the lithium disilicate ceramic veneers (IPS
abraded.We established the diagnosis of dental fluorosis of e.max Press ®) using CAD/CAM (figure 2.j-k-l).
Dean’s index 5 (figure 2.a-b).
After removal of the ceramic veneers, the bonding was
For this patient, 2253tw as proposed to treat the done under rubber dam isolation (figure 2.m). The
fluorosis with a combined treatment. A preliminary micro- treatment of the enamel surface was ensured by an adhesive
abrasion with Opalustre® followed by ceramic veneers from system of the MR type. An orthophosphoric acid etching
the right first premolar to the left first premolar. with a concentration of 40% was used (figure 2.n),
respecting the double etching technique (30 seconds),
After the patient’s agreement, we started with the followed by a grooving with water for 30 seconds (figure
placement of the rubber dam isolation, then, the micro 2.o).
abrasion with opalustre® paste was performed (figure 2.c).
After 6 cycles of application, a decrease in the saturation of After bonding, photos were taken after the removal of
the brownish color of the stains was noted, as well as a the dam (figure 2.p-q). A clinical control, after 3 months
harmonization of the hue. (figure 2.d) follow-up, has been done (figure 2.r-s-t).
Fig 2 Treatment of Severe Fluorosis with a Combination of Microabrasion and
IPS E.Max® Ceramic Veneers by CAD/CAM.
IJISRT23AUG1121 www.ijisrt.com 2253
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Clinical case n°3 diagnosis of dental fluorosis of Dean’s index 2 (figure 3.a).
A 23-healthy patient (R.B), non smoker, from Gafsa An armchair treatment with 16% hydrogen peroxide was
(South-West of Tunisia), consulted us, in the service of proposed and accepted by the patient. After placement of the
fixed prosthesis of Monastir, to solve his aesthetic problem. liquid rubber isolation dam (Figure 3.b), to provide gingival
The clinical examination showed the absence of carious protection. The product was applied to the vestibular
lesions, abrasions and defective restorations. A surface of the teeth for 45 minutes: 15 minutes per cycle
transillumination examination was performed. It showed the (figure 3.c). Each cycle includes, product placement
absence of dental cracks. Fine horizontal white streaks were followed by light curing (figure 3.d), and water grooving at
distributed over the entire tooth surface. These opaque stains the end of the 15 min. A picture was taken at the end of the
were also presented on the cusps and incisal edges. The session (figure 3.f).
shape of the teeth remained intact. We established the
Fig 3 Treatment of a Dental Fluorosis Dean’s Index 2 by Hydrogen Peroxide on the Chairside Under Liquid Rubber Dam
Isolation.
II. DISCUSSION In Tunisia, the south-west region ( Gabes, Gafsa,
Kairouan, Mednine , Sidi Bouzid , Tataouine), has a danger
Several studies have established the causal relationship quotient (QD) >1. These regions are considered as risk areas
between the use of water containing fluoride and the for dental fluorosis, caused by high doses of fluoride in
prevention of dental caries. Fluoride in drinking water can water(6 ppm). Therefore, this pathology presents a very
be found naturally or after being added artificially to prevent frequent aesthetic diagnostic element in these regions. (45)
tooth decay. According to the World Health Organization
(WHO) in 1986, fluoride at a concentration of 1 ppm or 1 The earliest sign is the color change showing many
mg per liter of water has the greatest cariostatic effect thin horizontal white lines across the surface of the teeth. At
without causing aesthetic disadvantages. Water fluoridation higher levels of fluoride exposure, these become more
is adopted in many countries and remains the most effective defined and thicker. Cloudy areas and thick opaque bands
method of prevention and treatment of dental caries also appear on the affected teeth which may be associated
compared to other prevention methods (toothpaste, drug with pits, hypoplasic enamel or even missing enamel. In
supplementation, professional treatment). (3/44) fact, the opaque white appearance of the enamel is caused
by an increase in the porosity of the underlying structures.
The overexposure during the mineralization phase to Due to interactions with various food coloring agents,
high doses (greater than or equal to 0.1 mg per kg / Day) in whitish stains can turn yellow or brownish-black. This
the body can cause dental fluorosis. Excessive ingestion of disease generally affects the entire dentition, all sides of an
fluorides after the age of 8 will not cause dental affected tooth are equally affected at the time of eruption
fluorosis.(10) and homologous teeth are always affected with the same
degree of severity. (11)
IJISRT23AUG1121 www.ijisrt.com 2254
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
The principle of preservation of dental tissue has a application and rinsing cycles, it is most likely that the
direct impact on the life of a tooth when it is restored. The discoloration is too deep. After treatment, the tooth surface
therapeutic gradient, "is a practical concept that should should be carefully polished with a silicone polishing burr or
guide the practitioner's thinking when faced with an fine disk to achieve a smooth surface, and a 2% fluoride gel
aesthetic request." (Thirlet and Attal 2009). When several (sodium fluoride, tin fluoride, sodium bicarbonate) should
therapies can be considered, the solution most adapted to the be used for 4-5 minutes to remineralize the tooth enamel
clinical case must be chosen in the spirit of tissue surface and prevent post-operative sensitivity. (22/23)
preservation. (7) This gradient must be applied in the
management of email anomalies. Then erosion-infiltration is a minimally invasive and
painless technique. Its first indication was to stop and
For dental fluorosis, the gradient starts with whitening prevent non-cavity caries progression at the proximal or
and microabrasion, then infiltrated resin, and in the most vestibular level. It is linked to the Icon®DMG system, its
complex cases, more invasive therapies. (12/13) principle consists in infiltrating the porosities within the
enamel (following the dissolution of the mineral phase)
Dental whitening is the first step in the treatment of through the Icon and thus preventing the diffusion of
stains caused by fluorosis. This technique respects the cariogenic acids. (24/25). This technique includes, in a first
principles of tissue economy and is the least invasive step, a demineralization performed with a 15% hydrochloric
technique in the treatment of dental fluorosis. (14). acid solution and, in a second step, an infiltration of the very
Bleaching is the result of an oxidative chemical reaction that low viscosity hydrophobic photopolymerizable composite
allows the release of nascent oxygen. This lightening agent resin. The infiltration of the porosities in the lesion is done
must penetrate the hard tissue without altering it and act on by a resin with a refractive index (1.52) that is close to a
the pigments that are responsible for the coloring and healthy enamel (1.62), which improves the transmission of
ensures its degradation following a redox reaction. This light photons through the hypo-mineralized enamel and
leads to changes in the absorption characteristics of light, restores its translucent appearance. This infiltration leads to
which leads to a reduction in the color of these molecules. an increase in the mechanical strength of the demineralized
(15/16). Whitening techniques are indicated as first-line enamel as well as an improvement in the resistance to
treatment for simple fluorosis (up to stage 3 of Dean's demineralization of the healthy enamel.(26/27/28). Indeed,
classification). The results are variable depending on the applications with an aesthetic aim are indicated such as the
patient and the clinical situation. The final aesthetic result is treatment of vestibular dyschromia: white spots linked to
difficult to predict because there is a strong individual fluorosis, MIH or even spots corresponding to the after-
variability. This technique is contraindicated when there is a effects of a trauma. Icon® is contraindicated in cases of
very large pulp chamber, dental hypersensitivity, gingival deep lesions, exceeding the outer third of the enamel, in
recession, enamel cracks or significant enamel loss, allergy cavities as well as in cases of allergy or intolerance to one of
to the products used, and teeth with extensive restorations. the components of the material. (29)
(17/18). Chairside sessions improve the color of fluorotic
teeth, but the combined treatment with a mouthpiece worn Composite resin veneers is a technique that has many
on an out patient basis for 15 days offers better responses to advantages in the context of anterior restorations, including
fluorosis and stability over time. (19) being less expensive for the patient, more conservative in
terms of dental tissue and can be performed in a single
Micro-abrasion is a non-invasive, simple, fast and clinical session. (30). This solution can be chosen in the
inexpensive technique. It is mainly used for mild to short term in order to satisfy an aesthetic demand while
moderate fluorosis. It removes superficial stains from the waiting for a more perennial rehabilitation (have a limited
tooth enamel in a controlled manner (between 20 and 200 lifespan in time, and can stain over the years). It is a very
microns, depending on the concentration of the acid and the conservative additive approach based on a layering
time of use). Brown stains are more superficial than white technique with different layers of composites each replacing
stains, which yield to micro-abrasion in 75% of cases, a type of dental tissue, reproducing the optical qualities of
whereas for brown stains the success rate is close to 100%. enamel and dentin. The goal is to achieve a biomimetic
(20). The principle of micro-abrasion with Opalustre is effect that allows light to pass through the restoration in a
based on a double mechanical and chemical action. The similar manner to natural teeth. (31)
mechanical action is performed with a diamond cup and a
burr, and the chemical attack is obtained with a 6.6% In cases of treatment of enamel anomalies, the
hydrochloric acid-based micro-abrasive paste containing complex layering protocol can be simplified because usually
microparticles of silica carbide and pumice powder (21). the morphology of the tooth remains intact and only the
The operative protocol consists of applying a layer of dyschromic part has been removed by microblasting or
abrasive mixture (2mm) on the vestibular surfaces of the milling. In more severe cases, the incisal edge may be
teeth. After installing a waterproof surgical field. Install a affected by hypomineralization and will therefore need to be
rubber cup on a low-speed contra-angle handpiece restored. The complex layering technique will be required
(1000rpm) that will move alternately over each tooth for 5 with the help of study models, laboratory wax-ups and
to 10 seconds for each cycle. Between each step, rinse with silicone keys.
water, dry and reassess the tooth surface before each new
application. However, if no improvement is seen after 6 to 7
IJISRT23AUG1121 www.ijisrt.com 2255
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
When the non-invasive techniques found their limits approximately two weeks to reduce the risk of failure and
and could not meet the needs of the patients, the prosthetic veneer delamination. (42)
solutions found their indications . (32/33). Since the 1980's,
with the development and evolution of bonding materials The light transmission of the veneer can be, in some
and technologies, today's ceramic veneers have the cases, a good indication given these advantages, but in other
reliability and aesthetic qualities required to correct situations, it is a real problem, especially when the support
discoloration problems while allowing tissue sparing. is strongly dyschromic as in cases of severe fluorosis.
(34/35) Therefore, the use of full-coverage prostheses (ceramic-
ceramic or metal-ceramic prosthesis) is the solution of
Among the multitude of ceramics, only some can be choice. (43)
used for the creation of dental veneers. These ceramics are
characterized by good optical properties: their translucency The full-coverage crown restoration is only indicated
must correspond to the pre-restoration discoloration of the in cases of severe fluorosis with very deep dark
teeth. The more the tooth is having a color that we want to discoloration or significant enamel loss. It may also be
correct, more the ceramic will have to be opaque or in thick indicated in cases of vertical dimension loss associated with
layer in order to mask the dyschromia. These ceramics must fluorosis. It is a macro-invasive technique (as opposed to
also have a large vitreous phase that can be etched to veneer restoration which is micro-invasive) which will
increase their bonding ability. Currently, the most affect the structural integrity of the tooth. (12)
commonly ceramics used are: feldspathic ceramics, leucite-
reinforced feldspathic ceramics, lithium disilicate-based III. CONCLUSION
ceramics and infiltrated aluminous ceramics. (36/37)
Fluorosis represents a fairly frequent reason for
When the bonding protocol is mastered, veneers can consultation, the damage of which is often aesthetic and
not only restore the mechanical properties of natural teeth, more or less important depending on the degree of severity
but also increase their strength compared to a healthy un- of the fluorosis.
treated tooth. Bonding increases the strength of the ceramic
restoration by creating a unique body between the restora- A precise diagnosis will be made by the practitioner
tion and the tooth. (38/39). Fluorite enamel has an impact on following the clinical examination in order to choose the
the way ceramic veneers are assembled, we note the effec- most appropriate therapeutic solution according to the
tiveness of the adhesive systems on fluoride enamel , whose clinical case.
adhesive material penetrates 3.5 μm into the enamel when
using phosphoric acid (Mordant and Rinse (MR) adhésive Tissue preservation nowadays is an essential
systems), while the material penetrates only 1 μm in the case prerequisite for any modern dental treatment. The
of a self-etching system (SAM). (40) Therefore, the use of partitionner should therefore choose the most conservative
an MR type adhesive system is much more effective for treatment possible according to the clinical case while
enamel-resin bonding and more stable over time than the respecting the therapeutic gradient.
SAM system for fluorite teeth. (41)
REFERENCES
For the concentration of ortho-phosphoric acid, studies
were performed on fluorotic teeth to examine the effects of [1]. TWETMAN, Svante, AXELSSON, Susanna,
orthophosphoric acids in different concentrations of 35%, DAHLGREN, Helena, et al. Caries‐preventive effect
40% and 45% on bonding. Maximum bond strengths were of fluoride toothpaste: a systematic review. Acta
achieved when phosphoric acid of 40% concentration was Odontologica Scandinavica, 2003, vol. 61, no 6, p.
used. (41) 347-355.
[2]. OGANESSIAN, E., LENCOVA, E., et BROUKAL, Z.
Also, hypermineralized fluorotic enamel, where Is systemic fluoride supplementation for dental caries
hydroxyapatite is replaced by fluoroapatite, is more difficult prevention in children still justifiable. Prague Medical
to etch than healthy enamel. The double etching technique Report, 2007, vol. 108, no 4, p. 306-314.
must then be used. Hence, for moderate fluorosis, it is [3]. Agence Française de Sécurité Sanitaire des Produits de
recommended to double the enamel etching time (30 Santé. Utilisation du fluor dans la prévention de la
seconds) for best conditions with 37% phosphoric acid in carie dentaire avant l'âge de 18 ans. J Pediatr Puericult
order to obtain an effective bonding strength and to remove 2009;22:235-40.
the 50-80 mm thick outer layer of hypermineralization. (39) [4]. Fejerskov O, Kidd EA. Dental caries: the disease and
its clinical management. Iowa: Blackwell Munksgaard,
In certain situations such as moderate fluorosis, a 2008.
preliminary treatment by a hydrogen peroxide (H2O2) [5]. Belkhir MS, Triller M.Modifications ultrastructurales
whitening must be considered before the realization of the de la dent fluorotiques et conséquences cliniques.
ceramic veneers in order to attenuate the dental dyschromia Actual Odontostomatol 1987;158:224-37.
and to harmonize the basic color for a better aesthetic result. [6]. Levy SM. Une mise à jour sur les fluorures et la
It is recommended, after using hydrogen peroxide at 35% fluorose. J Assoc Dent Can 2014;69:286-91
concentration, to delay the bonding of the veneers for
IJISRT23AUG1121 www.ijisrt.com 2256
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[7]. Adelario AK, Vilas-Novas LF, Castilho LS, Vargas [24]. Attal JP, Atlan A, Denis M, Vennat E, Tirlet G.
AM, Ferreira EF, Abreu MH. Accuracy of the Nouveau concept pour le masquage des taches de
simplified Thylstrup & Fejerskov index in rural l’émail. L’infiltration en profondeur - Partie II.
communities with endemic fluorosis. Int J Environ Res Traitement d’une fluorose. Inf Dent 2014;2:1-6.
Public Health 2010;7(3):927-37. [25]. Attal JP, Denis M, Atlan A, Vennat E, Tirlet G.
[8]. Denbesten PK, Li W. Chronic fluoride toxicity: dental L’infiltration en profondeur: un nouveau concept pour
fluorosis. Monograph Oral Sci 2011;22:81-96. le masquage des tâches blanches de l’émail. Partie 1.
[9]. FEJERSKOV, O., MANJI, F., et BAELUM, V. The Inf Dent 2013;19:74-9
nature and mechanisms of dental fluorosis in man. [26]. Attal JP, Atlan A, Denis M, Vennat E, Tirlet G. Taches
Journal of dental research, 1990, vol. 69, no 2_suppl, blanches de l’émail: protocole de traitement par
p. 692-700. infiltration superficielle ou en profondeur (partie 2). Int
[10]. Bronckers AL, Lyaruu DM, Denbesten PK. The impact Orthod 2014;12(1):1-31.
of fluoride on ameloblasts and the mechanisms of [27]. Castro KS, Ferreira AC, Duarte RM, Sampaio FC,
enamel fluorosis. J Dent Res 2009;88:877-93. Meireles SS. Acceptability, efficacy and safety of two
[11]. Denbesten PK, Li W. Chronic fluoride toxicity: dental treatment protocols for dental fluorosis: a randomized
fluorosis. Monograph Oral Sci 2011;22:81-96. clinical trial. J Dent 2014;42:938-44.
[12]. Sherwood IA. Fluorosis varied treatment options. J [28]. Paris S, Schwendicke F, Keltsch J, Dorfer C, Meyer-
Conserv Dent 2010;13(1):47 53. Lueckel H.Masking of white spot lesions by resin
[13]. Chhabra N, Singbal KP. Viable approach to manage infiltration in vitro.
superficial enamel discoloration. Contemp Clin Dent J Dent 2013;41(5):28-34.
2010;1(4):284-7. [29]. Taher NM, Alkhamis HA, Dowaidi SM. The influence
[14]. Ardu S, Stavridakis M, Krejci I. A minimally invasive of resin infiltration system on enamel microhardness
treatment of severe dental fluorosis. Quintescence Int and surface roughness: an in vitro study. Saudi Dent J
2007;38(6):455 8. 2012;24(2):79-84.
[15]. Buchalla W, Attin T.External beaching therapy with [30]. Korkut B. Smile makeover with direct composite
activation by heat, light or laser-A systematic review. veneers: A two-year follow-up report. J Dent Res Dent
Dent Mater 2007; 23:586-96. Clin Dent Prospects 2018;12(2):146-51.
[16]. Fernández E, Bersezio C, Bottner J et al. Longevity, [31]. Magne P, Belser U, Liger F. Restaurations adhésives
esthetic perception, and psychosocial impact of teeth en céramique sur dents antérieures: approche
bleaching by low (6%) hydrogen peroxide biomimétique. Paris: Quintessence International, 2003.
concentration for in-office treatment: a randomized [32]. Akpata ES.Therapeutic management of dental
clinical trial. Oper Dent 2017;42:41-52. fluorosis: A critical review of literature. Saudi J Oral
[17]. Pignoly C. Eclaircissement des dents pulpées : Sci 2014;1(1):3-13
pourquoi la technique au fauteuil est elle toujours [33]. Dogui H , Dakhli R, Abdelmalek F, Nouira Z, Amor
d’actualité ? Les 10 points clés sur les dyschromies A, Cherif M. Aesthetic rehabilitation of severe dental
dentaires 2015:29-36 fluorosis with Porcelain Veneers: About a case report.
[18]. Pillon F, Pillot G. Le blanchiment des dents, un acte IOSR J Dent Med Sci 2019;18(11):57-63.
sous contrôle des professionnels de santé. Actual [34]. Kruetongsri K, Leevailoj C.Treatment of moderate
Pharm 2014;53:49-52. dental fluorosis using porcelain laminate veneers: A
[19]. Perdigão J, Lam VQ, Burseth BG, Real C. Masking of case report. Chulalongkorn Univ Dent J 2013;35(1):49
enamel fluorosis discolorations and tooth misalignment 64.
with a combination of at-home whitening, resin [35]. Verma A. Smile makeover in a patient with severe
infiltration, and direct composite restorations. Oper dental fluorosis using ceramic laminate veneers: a case
Dent 2017;42(4):347-56. report. Int J Sci Res 2019;18(10):1464-7.
[20]. Daskalaki Z, Alifakioti E, Arhakis A. Aesthetic [36]. Della Bona A, Borba M, Benetti P, Cecchetti D. Effect
treatment of dental fluorosis in a 9-year-old girl: Case of surface treatments on the bond strenght of a
report. Balk J Dent Med 2019;23(3):157-62 zirconia-reinforced ceramic to composite resin. Braz
[21]. Perete-de-Freitas CE, Silva PD, Faria-E-Silva AL. Oral Res 2007;21(1):10-5.
Impact of microabrasion on the effectiveness of tooth [37]. Etienne O. Les facettes en céramique. Paris : CdP ;
bleaching. Braz Dent J 2017;28(5):612-7. 2013.
[22]. Romero MF, Babb CS, Delash J, Brackett WW. [38]. Oudin Gendrel A. Les protocoles d’assemblage en
Minimally invasive esthetic improvement in a patient prothèse fixée. Inf Dent 2019;25.
with dental fluorosis by using microabrasion and [39]. Torres-Gallegos I, Zavala-Alonso V, Patiño-Marín N,
bleaching: A clinical report. J Prosthet Dent Martinez-Castañon GA, Anusavice K, Loyola-
2018;120(3):323-6. Rodríguez JP. Enamel roughness and depth profile
[23]. Sundfeld D, Pavani CC, Schott TC et al. Dental after phosphoric acid etching of healthy and fluorotic
bleaching on teeth submitted to enamel microabrasion enamel. Aust Dent J 2012;57(2):151-6.
30 years ago-a case report of patients' compliance [40]. Ermis RB, Van Landuyt K, Van Meerbeek B, Swift EJ
during bleaching treatment. Clin Oral Investig Jr.Bonding to fluorosed teeth. J Esthet Restor Dent
2019;23(1):321-6. 2009;21(4):213-4.
IJISRT23AUG1121 www.ijisrt.com 2257
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[41]. Gu M, Lv L, He X, Li W, Guo L. Effect of phosphoric
acid concentration used for etching on the microtensile
bond strength to fluorotic teeth. Medicine
2018;97(35):e12093.
[42]. Imani MM, Azizi F, Bahrami K, Golshah A, Safari-
Faramani R. In vitro bleaching effect of hydrogen
peroxide with different time of exposition and
concentration on shear bond strength of orthodontic
brackets to human enamel: A meta-analysis of in vitro
studies. Int Orthod 2020;18(1):22-31.
[43]. Meireles SS, Heckmann SS, Santos IS, Della Bona A,
Demarco FF. A double blind randomized clinical trial
of at home tooth, bleaching using two carbamide
peroxide concentrations: 6 month follow up. J Dent
2008;36:878-84.
[44]. Organisation Mondiale de la Santé.Le bon usage des
fluorures pour la santé de l’homme. Genève : OMS,
1986.
[45]. Maâtouk F. Fluoride & oral prevention [En Ligne].
Disponible à partir l'URL: http://maatouk.tripod.com/
IJISRT23AUG1121 www.ijisrt.com 2258
You might also like
- RCT Success and Pain ReliefDocument39 pagesRCT Success and Pain ReliefSoo YoongNo ratings yet
- The Body Never Lies PDFDocument5 pagesThe Body Never Lies PDFhmyzone55No ratings yet
- Comprehensive Management of Severe Dental Fluorosis With Adhesively Bonded All-Ceramic RestorationsDocument15 pagesComprehensive Management of Severe Dental Fluorosis With Adhesively Bonded All-Ceramic RestorationsNicole StoicaNo ratings yet
- (23350245 - Balkan Journal of Dental Medicine) Aesthetic Treatment of Dental Fluorosis in A 9-Year-Old Girl - Case Report PDFDocument6 pages(23350245 - Balkan Journal of Dental Medicine) Aesthetic Treatment of Dental Fluorosis in A 9-Year-Old Girl - Case Report PDFNadhyaNo ratings yet
- Desensitasi 2Document7 pagesDesensitasi 2fennilubisNo ratings yet
- Zotti 2020Document14 pagesZotti 2020Max PosseltNo ratings yet
- White SpotsDocument24 pagesWhite SpotsDonanguyenNo ratings yet
- Fs Guideline Online Final V 2Document6 pagesFs Guideline Online Final V 2DeasireeNo ratings yet
- Niño 2Document6 pagesNiño 2Kev aqpNo ratings yet
- Chronic Fluoride Toxicity: Dental Fluorosis: Pamela Denbesten Wu LiDocument16 pagesChronic Fluoride Toxicity: Dental Fluorosis: Pamela Denbesten Wu Lizen epicNo ratings yet
- 10 Muhammad Salman RashidDocument3 pages10 Muhammad Salman Rashidrahul sharmaNo ratings yet
- Enlightening Diagnosis and Differential DiagnosisDocument8 pagesEnlightening Diagnosis and Differential DiagnosisYusti Nur UtamiNo ratings yet
- Dis ColorDocument13 pagesDis ColortarekrabiNo ratings yet
- OunsiDocument7 pagesOunsiDanis Diba Sabatillah YaminNo ratings yet
- An Unusual Case of Gemination in Mandibular Second Premolar A Case ReportDocument4 pagesAn Unusual Case of Gemination in Mandibular Second Premolar A Case ReportDanish NasirNo ratings yet
- Eb 79Document5 pagesEb 79mohammad naufalNo ratings yet
- Endodontic and Orthodontic Case ReportDocument4 pagesEndodontic and Orthodontic Case ReportkakodkarNo ratings yet
- Internal Resorption Review: Causes, Diagnosis, TreatmentDocument4 pagesInternal Resorption Review: Causes, Diagnosis, TreatmentmaharaniNo ratings yet
- Effect of Fluoride-Releasing Resin Composite in White Spot Lesions Prevention: A Single-Centre, Split-Mouth, Randomized Controlled TrialDocument7 pagesEffect of Fluoride-Releasing Resin Composite in White Spot Lesions Prevention: A Single-Centre, Split-Mouth, Randomized Controlled TrialXIID 67No ratings yet
- Case Report: Management of A Severely Submerged Primary Molar: A Case ReportDocument4 pagesCase Report: Management of A Severely Submerged Primary Molar: A Case ReportCalvintNo ratings yet
- Extreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical ManagementDocument8 pagesExtreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical Managementcarmen espinozaNo ratings yet
- Lecture 5, Measuring Dental FluorosisDocument3 pagesLecture 5, Measuring Dental FluorosisJustDen09No ratings yet
- Unraveling The Enigma of Amelogenesis Imperfecta: A Detailed Case ReportDocument5 pagesUnraveling The Enigma of Amelogenesis Imperfecta: A Detailed Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Australian Dental Journal - 2009 - Abbott - Internal Bleaching of Teeth An Analysis of 255 TeethDocument8 pagesAustralian Dental Journal - 2009 - Abbott - Internal Bleaching of Teeth An Analysis of 255 Teethnafsiyah xyzNo ratings yet
- An Alternative Technique of Bleaching Vital ToothDocument3 pagesAn Alternative Technique of Bleaching Vital ToothMissyNo ratings yet
- 1 - Methods of Measuring Dental FluorosisDocument5 pages1 - Methods of Measuring Dental FluorosisJehad Ali Al-ammariNo ratings yet
- Weaknenamel Enamel HypoplasiaDocument4 pagesWeaknenamel Enamel HypoplasiaNeeraj SharmaNo ratings yet
- Tooth Discolour at Ion and StainingDocument8 pagesTooth Discolour at Ion and StainingNilesh S KadamNo ratings yet
- Combined minimally invasive treatment of white and brown fluorotic discolorations in a teenagerDocument8 pagesCombined minimally invasive treatment of white and brown fluorotic discolorations in a teenagerandres gabrielNo ratings yet
- Should the UK Add Fluoride to Drinking WaterDocument8 pagesShould the UK Add Fluoride to Drinking WaterClaire LeightonNo ratings yet
- GulusinDocument5 pagesGulusinEkta KhobragadeNo ratings yet
- Dentistry 10 00150Document10 pagesDentistry 10 00150Sam RasydNo ratings yet
- Papillon Lefevre SyndromeDocument4 pagesPapillon Lefevre SyndromemNo ratings yet
- د. خولة محمد Dental Fluorosis-1 (Muhadharaty)Document5 pagesد. خولة محمد Dental Fluorosis-1 (Muhadharaty)علي موسى مهديNo ratings yet
- InTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsDocument25 pagesInTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsNeagu EmaNo ratings yet
- Amelogenesis Imperfecta: Therapeutic Strategy From Primary To Permanent Dentition Across Case ReportsDocument8 pagesAmelogenesis Imperfecta: Therapeutic Strategy From Primary To Permanent Dentition Across Case ReportsbanyubiruNo ratings yet
- Turner's HypoplasiaDocument4 pagesTurner's HypoplasiaAzi Pertiwi HussainNo ratings yet
- While LesionDocument7 pagesWhile LesionFourthMolar.comNo ratings yet
- Management of Dental Fluorosis Based On Severity IndexDocument6 pagesManagement of Dental Fluorosis Based On Severity IndexIJAR JOURNALNo ratings yet
- Gingival Labial Recessions and The Post-Treatment Proclination of Mandibular IncisorsDocument7 pagesGingival Labial Recessions and The Post-Treatment Proclination of Mandibular Incisorsريام الموسويNo ratings yet
- Jurnal PedoDocument4 pagesJurnal PedoMantika AtiqahNo ratings yet
- Sidang Tesis TGL 30 Oktober 2014 Final FixedDocument11 pagesSidang Tesis TGL 30 Oktober 2014 Final Fixedfaizal prabowo KalimanNo ratings yet
- Dental Clinic PowerPoint TemplatesDocument14 pagesDental Clinic PowerPoint TemplatesnancyNo ratings yet
- Bishara2008 PDFDocument9 pagesBishara2008 PDFSai KrupaNo ratings yet
- Dental Erosion in Children: A Literature ReviewDocument7 pagesDental Erosion in Children: A Literature ReviewHala LalaNo ratings yet
- Pulp Therapy in Maxillary Fused Primary Central and Lateral Incisor: A Case ReportDocument6 pagesPulp Therapy in Maxillary Fused Primary Central and Lateral Incisor: A Case ReportAsriNo ratings yet
- Treatment of A Patient With Oligodontia A Case ReportDocument5 pagesTreatment of A Patient With Oligodontia A Case ReportWindaNo ratings yet
- Dental Wear - A Scanning Electron Microscope Study - 2014Document8 pagesDental Wear - A Scanning Electron Microscope Study - 2014Ana CondeNo ratings yet
- Classification of Tooth Discolouration Causes and MechanismsDocument14 pagesClassification of Tooth Discolouration Causes and MechanismsSARINAHNo ratings yet
- Managing cracked teeth with conservative treatmentDocument10 pagesManaging cracked teeth with conservative treatmentNaji Z. ArandiNo ratings yet
- Compound Odontoma Associated With Impacted Teeth: A Case ReportDocument4 pagesCompound Odontoma Associated With Impacted Teeth: A Case ReportayuandraniNo ratings yet
- 8-Treatment of Deep Caries, Vital Pulp Exposure, Pulpless TeethDocument8 pages8-Treatment of Deep Caries, Vital Pulp Exposure, Pulpless TeethAhmed AbdNo ratings yet
- The Nature and Mechanisms of Dental Fluorosis in Man: Et Al.Document9 pagesThe Nature and Mechanisms of Dental Fluorosis in Man: Et Al.mageshwariNo ratings yet
- Non Syndromic Generalised MacrodontiaDocument4 pagesNon Syndromic Generalised MacrodontiaArum Kartika DewiNo ratings yet
- 3435-Article Text-10228-1-10-20211027Document6 pages3435-Article Text-10228-1-10-20211027Irin Susan VargheseNo ratings yet
- A Minimally Invasive Treatment of Severe Dental FluorosisDocument4 pagesA Minimally Invasive Treatment of Severe Dental FluorosisMohammed AldaosariNo ratings yet
- Pedodontic Lect 17Document10 pagesPedodontic Lect 17Mustafa AmmarNo ratings yet
- Ojst20110300009 24394623Document6 pagesOjst20110300009 24394623Nandini KattaNo ratings yet
- April 2002: East African Medical Journal 221Document3 pagesApril 2002: East African Medical Journal 221Sreekanth KrishnamurthyNo ratings yet
- LUSSI, 2019. The Use of Fluoride For The Prevention of Dental Erosion and Erosive Tooth Wear in Children and Adolescents PDFDocument11 pagesLUSSI, 2019. The Use of Fluoride For The Prevention of Dental Erosion and Erosive Tooth Wear in Children and Adolescents PDFJohnatan MeirelesNo ratings yet
- Comparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightDocument4 pagesComparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Electro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyDocument7 pagesElectro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonDocument14 pagesTerracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions on Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions on Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Review: Pink Eye Outbreak in IndiaDocument3 pagesA Review: Pink Eye Outbreak in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETDocument6 pagesAuto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design, Development and Evaluation of Methi-Shikakai Herbal ShampooDocument8 pagesDesign, Development and Evaluation of Methi-Shikakai Herbal ShampooInternational Journal of Innovative Science and Research Technology100% (3)
- A Survey of the Plastic Waste used in Paving BlocksDocument4 pagesA Survey of the Plastic Waste used in Paving BlocksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentDocument7 pagesCyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hepatic Portovenous Gas in a Young MaleDocument2 pagesHepatic Portovenous Gas in a Young MaleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Explorning the Role of Machine Learning in Enhancing Cloud SecurityDocument5 pagesExplorning the Role of Machine Learning in Enhancing Cloud SecurityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Navigating Digitalization: AHP Insights for SMEs' Strategic TransformationDocument11 pagesNavigating Digitalization: AHP Insights for SMEs' Strategic TransformationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Perceived Impact of Active Pedagogy in Medical Students' Learning at the Faculty of Medicine and Pharmacy of CasablancaDocument5 pagesPerceived Impact of Active Pedagogy in Medical Students' Learning at the Faculty of Medicine and Pharmacy of CasablancaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Automatic Power Factor ControllerDocument4 pagesAutomatic Power Factor ControllerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mobile Distractions among Adolescents: Impact on Learning in the Aftermath of COVID-19 in IndiaDocument2 pagesMobile Distractions among Adolescents: Impact on Learning in the Aftermath of COVID-19 in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Review of Biomechanics in Footwear Design and Development: An Exploration of Key Concepts and InnovationsDocument5 pagesReview of Biomechanics in Footwear Design and Development: An Exploration of Key Concepts and InnovationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Studying the Situation and Proposing Some Basic Solutions to Improve Psychological Harmony Between Managerial Staff and Students of Medical Universities in Hanoi AreaDocument5 pagesStudying the Situation and Proposing Some Basic Solutions to Improve Psychological Harmony Between Managerial Staff and Students of Medical Universities in Hanoi AreaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effect of Time Variables as Predictors of Senior Secondary School Students' Mathematical Performance Department of Mathematics Education Freetown PolytechnicDocument7 pagesThe Effect of Time Variables as Predictors of Senior Secondary School Students' Mathematical Performance Department of Mathematics Education Freetown PolytechnicInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drug Dosage Control System Using Reinforcement LearningDocument8 pagesDrug Dosage Control System Using Reinforcement LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Securing Document Exchange with Blockchain Technology: A New Paradigm for Information SharingDocument4 pagesSecuring Document Exchange with Blockchain Technology: A New Paradigm for Information SharingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Enhancing the Strength of Concrete by Using Human Hairs as a FiberDocument3 pagesEnhancing the Strength of Concrete by Using Human Hairs as a FiberInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formation of New Technology in Automated Highway System in Peripheral HighwayDocument6 pagesFormation of New Technology in Automated Highway System in Peripheral HighwayInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Supply Chain 5.0: A Comprehensive Literature Review on Implications, Applications and ChallengesDocument11 pagesSupply Chain 5.0: A Comprehensive Literature Review on Implications, Applications and ChallengesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intelligent Engines: Revolutionizing Manufacturing and Supply Chains with AIDocument14 pagesIntelligent Engines: Revolutionizing Manufacturing and Supply Chains with AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Self-Disposing Contactless Motion-Activated Trash Bin Using Ultrasonic SensorsDocument7 pagesThe Making of Self-Disposing Contactless Motion-Activated Trash Bin Using Ultrasonic SensorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 5 6269504843056939800Document141 pages5 6269504843056939800SwapardeshiNo ratings yet
- Enrollment No B.A. LL.B./II Sem./ET/Apr-20/Eng-IIDocument14 pagesEnrollment No B.A. LL.B./II Sem./ET/Apr-20/Eng-IIShashwat SinghNo ratings yet
- Innovative Use of Virtual Reality in Autism Spectrum Disorder: A Case-StudyDocument12 pagesInnovative Use of Virtual Reality in Autism Spectrum Disorder: A Case-StudyomenpkuNo ratings yet
- Making Strides EbookDocument18 pagesMaking Strides EbooksamNo ratings yet
- Care Plan: Degree Programme in Nursing School of Health and Social StudieDocument14 pagesCare Plan: Degree Programme in Nursing School of Health and Social Studiepevala8648No ratings yet
- Hiv and Prevention of Mother-To-Child Transmission (PMTCT) : by Gebremaryam TDocument100 pagesHiv and Prevention of Mother-To-Child Transmission (PMTCT) : by Gebremaryam THambal AhamedNo ratings yet
- Writ CallDocument4 pagesWrit CallSandhya GurunathNo ratings yet
- FisabaroxefuragegobaDocument2 pagesFisabaroxefuragegobaOswaldo Jurado0% (1)
- Assignment On Element3 Safety CultureDocument3 pagesAssignment On Element3 Safety CultureSAFETY VOFPL100% (2)
- Nursing DiagnosisDocument16 pagesNursing DiagnosisShemie TutorNo ratings yet
- COVID-19 Information, LucknowDocument2 pagesCOVID-19 Information, LucknowVipul GautamNo ratings yet
- De-Escalation in Health Care. Quick Safety. The Joint Commission, Division of Healthcare Improvement Issue 47 - January 2019Document4 pagesDe-Escalation in Health Care. Quick Safety. The Joint Commission, Division of Healthcare Improvement Issue 47 - January 2019Urgencias HorwitzNo ratings yet
- CefabroxilDocument12 pagesCefabroxilRawdatul JannahNo ratings yet
- Retdem Part 2Document4 pagesRetdem Part 2gave maternityNo ratings yet
- Standardization and Upgrading of Barmm HospitalsDocument41 pagesStandardization and Upgrading of Barmm HospitalsApipah Datudacula-MacabangkitNo ratings yet
- MEDUMAT Transport 83428-ENDocument16 pagesMEDUMAT Transport 83428-ENShota MukhashavriaNo ratings yet
- Bonardi2017 - Cópia PDFDocument11 pagesBonardi2017 - Cópia PDFRENATO SUDATINo ratings yet
- FCCS Course Advert 22.09.2022 - FinalDocument2 pagesFCCS Course Advert 22.09.2022 - FinalShaneabbas JafferNo ratings yet
- MARGARITA BrandDocument32 pagesMARGARITA BrandCARDIAC8No ratings yet
- MCC 34 DomperidoneDocument40 pagesMCC 34 DomperidoneAnonymous PTSx0GANo ratings yet
- Effect of Emotional Intelligence On Work Stress I J IcbmDocument15 pagesEffect of Emotional Intelligence On Work Stress I J Icbmbhavya mishraNo ratings yet
- What Is Artificial Meat PDFDocument18 pagesWhat Is Artificial Meat PDFDivya DiyaNo ratings yet
- Kebutuhan Cairan NeonatusDocument3 pagesKebutuhan Cairan NeonatusGendis SudjaNo ratings yet
- Republic of The Philippines Province of Rizal Municipality of Rodriguez Barangay Geronimo Office of Sangguniang KabataanDocument3 pagesRepublic of The Philippines Province of Rizal Municipality of Rodriguez Barangay Geronimo Office of Sangguniang KabataanMark MagsilaNo ratings yet
- Automation of Drug Dispensing: Feedback From A Hospital PharmacyDocument5 pagesAutomation of Drug Dispensing: Feedback From A Hospital PharmacyIJAR JOURNALNo ratings yet
- 016 - Attachment For Full Scale Shear Pads - 01 Mar 11Document54 pages016 - Attachment For Full Scale Shear Pads - 01 Mar 11nadraNo ratings yet
- COSHH Clenzol (APC)Document3 pagesCOSHH Clenzol (APC)zaimNo ratings yet
- FITNESS ASSESSMENT AND SELF-EVALUATIONDocument2 pagesFITNESS ASSESSMENT AND SELF-EVALUATIONdiane100% (1)
- Miller 2010 Chapter 2Document22 pagesMiller 2010 Chapter 2elsaNo ratings yet