You might also like
- Spiritual Well Being in Patients With Rheumatoid.3 PDFDocument12 pagesSpiritual Well Being in Patients With Rheumatoid.3 PDFAriel Anaya GalvisNo ratings yet
- Review: James W. Daily, Mini Yang, and Sunmin ParkDocument13 pagesReview: James W. Daily, Mini Yang, and Sunmin Parkv_azygosNo ratings yet
- Reh ImmunlogyDocument18 pagesReh Immunlogygavallapalli ramyaNo ratings yet
- ArthritisDocument8 pagesArthritisnonyeprecious4959No ratings yet
- JRM 55 2572Document13 pagesJRM 55 2572Vnime MusicNo ratings yet
- Animal Models of Arthritis With Varied Etiopathology and Their Significance - B - SR Naik, SM Wala - BDocument11 pagesAnimal Models of Arthritis With Varied Etiopathology and Their Significance - B - SR Naik, SM Wala - BJohanmary GallardoNo ratings yet
- ArthritisDocument16 pagesArthritisVikas JhawatNo ratings yet
- 1 s2.0 S2772753X22000739 MainDocument15 pages1 s2.0 S2772753X22000739 MainRina HerowatiNo ratings yet
- Neuropatía ReumatoideDocument9 pagesNeuropatía ReumatoideJorge GámezNo ratings yet
- Self Management Program of Client With Artritis Literature ReviewDocument8 pagesSelf Management Program of Client With Artritis Literature Reviewika wahyuni puji lestariNo ratings yet
- AR para ManosDocument22 pagesAR para ManosAndres CasteloNo ratings yet
- Musculoskeletal 3 ModuleDocument14 pagesMusculoskeletal 3 Modulejibran khanNo ratings yet
- Neuropsychiatry in Clinical Practice: The Challenge of Diagnosing Behavioral Variant Frontotemporal DementiaDocument53 pagesNeuropsychiatry in Clinical Practice: The Challenge of Diagnosing Behavioral Variant Frontotemporal DementiaMark A. FosterNo ratings yet
- Nihms 1583867Document48 pagesNihms 1583867RONALDO ABDALLANo ratings yet
- Sensory Processing Disorders - Diagnostic and Therapeutic ControversiesDocument10 pagesSensory Processing Disorders - Diagnostic and Therapeutic ControversiesiimNo ratings yet
- A Review of The Relation Between Dissociation, Memory, Executive FunctionDocument25 pagesA Review of The Relation Between Dissociation, Memory, Executive FunctionHelena QuintNo ratings yet
- Rematological ExaminationDocument37 pagesRematological ExaminationAbdul BasitNo ratings yet
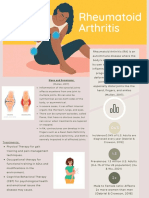
- Rheumatoid Arthritis: Signs and SymptomsDocument2 pagesRheumatoid Arthritis: Signs and SymptomsTatiana EdmistonNo ratings yet
- Response To Treatment in Osteoarthritis Clinical Trial: A Narrative ReviewDocument8 pagesResponse To Treatment in Osteoarthritis Clinical Trial: A Narrative ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluación - Historia ClínicaDocument9 pagesEvaluación - Historia ClínicamonseibanezbarraganNo ratings yet
- Functional Neurologic Disorders, Disorders To Be Managed by Neurologists, or Are Neurologists Wandering in A Dangerous Field With Inadequate Resources?Document16 pagesFunctional Neurologic Disorders, Disorders To Be Managed by Neurologists, or Are Neurologists Wandering in A Dangerous Field With Inadequate Resources?955g7sxb8pNo ratings yet
- Zingerone Sci - Pharmacotherapeutic Potential of Ginger and Its Compounds in Age-Related Neurological DisordersDocument15 pagesZingerone Sci - Pharmacotherapeutic Potential of Ginger and Its Compounds in Age-Related Neurological DisordersyunusNo ratings yet
- Small Amygdala - High AggressionDocument7 pagesSmall Amygdala - High AggressionfernandogfcnsNo ratings yet
- Icns 9 7-8 42Document6 pagesIcns 9 7-8 42caydin33No ratings yet
- Functional Neurological Disorder - New Subtypes and Shared MechanismsDocument14 pagesFunctional Neurological Disorder - New Subtypes and Shared MechanismsDalal HazelNo ratings yet
- Somatization in Patients With Dissociative DisordersDocument6 pagesSomatization in Patients With Dissociative DisordersfranciscoNo ratings yet
- Dolor y Aspectos PsicologicosDocument13 pagesDolor y Aspectos PsicologicosEVER HEYNAR ROSENTHAL ARIASNo ratings yet
- Self Management Program of Client With Artritis Literature ReviewDocument7 pagesSelf Management Program of Client With Artritis Literature Reviewhafizayenti22No ratings yet
- Management of OADocument15 pagesManagement of OARudy HsNo ratings yet
- The Role of Personality in Patients With FibromyalgiaDocument18 pagesThe Role of Personality in Patients With FibromyalgiaPsiquiatria para todosNo ratings yet
- Journal of Ayurveda and Integrative MedicineDocument4 pagesJournal of Ayurveda and Integrative MedicineMiftakhul ViviNo ratings yet
- The Relationship of Cognitive Functions and Psychopathology On The Level of Insight in Patients With SchizophreniaDocument6 pagesThe Relationship of Cognitive Functions and Psychopathology On The Level of Insight in Patients With SchizophrenianandhaNo ratings yet
- Homoeopathic Approach in The Cases of Rheumatic Disorders of JointsDocument5 pagesHomoeopathic Approach in The Cases of Rheumatic Disorders of JointsEditor IJTSRD0% (1)
- The Interpersonal Dimension of Borderline Personality Disorder Toward A Neuropeptide ModelDocument28 pagesThe Interpersonal Dimension of Borderline Personality Disorder Toward A Neuropeptide Modelme13No ratings yet
- Sports Medicine Meets Musculoskeletal MeDocument3 pagesSports Medicine Meets Musculoskeletal MeMotea IoanaNo ratings yet
- Juvenile Idiopathic ArthritisDocument14 pagesJuvenile Idiopathic ArthritisLuis Enrique Jara Romero100% (1)
- Article 1480331265Document4 pagesArticle 1480331265LOKESH RATRENo ratings yet
- Arthritis and Related Disorders Types and TreatmentDocument8 pagesArthritis and Related Disorders Types and Treatmentmf6pjpswswNo ratings yet
- Manual Physical Therapy As A Novel Treatment Modality For Autism Spectrum Disorder - A Pilot StudyDocument6 pagesManual Physical Therapy As A Novel Treatment Modality For Autism Spectrum Disorder - A Pilot StudyLeandro Vieira de LaraNo ratings yet
- Neurological and Psychiatric Disorders in Psoriasis 2018Document9 pagesNeurological and Psychiatric Disorders in Psoriasis 2018Cristian QuitoNo ratings yet
- Neuroticism and Affective Instability: The Same or Different?Document7 pagesNeuroticism and Affective Instability: The Same or Different?Tălpău Laura-GabrielaNo ratings yet
- A Cele Rome TriaDocument18 pagesA Cele Rome TriaYessenia PasmayNo ratings yet
- Rheumatoid ArthritisDocument8 pagesRheumatoid ArthritisBriant BlantonNo ratings yet
- NusrsingDocument5 pagesNusrsingAntony OgemboNo ratings yet
- Functional Neurological Disorder New Subtypes and Shared Mechanisms - CLINICALKEY - DR RivasDocument14 pagesFunctional Neurological Disorder New Subtypes and Shared Mechanisms - CLINICALKEY - DR RivasFernando Pérez MuñozNo ratings yet
- 10.1515 - Jom 2021 0081Document8 pages10.1515 - Jom 2021 0081consueloamado.medNo ratings yet
- Management of Rheumatoid Arthritis Through AyurvedaDocument4 pagesManagement of Rheumatoid Arthritis Through AyurvedaManish BashyalNo ratings yet
- Kompres Jahe Merah Berpengaruh Terhadap Penurunan Skala Nyeri Osteoartritis Pada Lanjut Usia Di Wilayah Kerja Puskesmas Kampung Delima TAHUN 2016Document9 pagesKompres Jahe Merah Berpengaruh Terhadap Penurunan Skala Nyeri Osteoartritis Pada Lanjut Usia Di Wilayah Kerja Puskesmas Kampung Delima TAHUN 2016diarNo ratings yet
- Thoracic Outlet SyndromeDocument11 pagesThoracic Outlet SyndromeTan Zhen XinNo ratings yet
- Neurological Disorders: Causes and Treatments Strategies: April 2018Document10 pagesNeurological Disorders: Causes and Treatments Strategies: April 2018Friska HarianjaNo ratings yet
- OA Junal NeuroDocument6 pagesOA Junal NeuroDzulRizkaNo ratings yet
- Medicines 07 00067Document18 pagesMedicines 07 00067Natasya Ayusandra MahersaputriNo ratings yet
- Evaluation of Integrated Approach of Psycho and Yoga Therapy in Management of Anxiety Neurosis: A Case StudyDocument13 pagesEvaluation of Integrated Approach of Psycho and Yoga Therapy in Management of Anxiety Neurosis: A Case StudyDr. Manoranjan TripathyNo ratings yet
- OsteoartritisDocument9 pagesOsteoartritisWalter Espinoza CiertoNo ratings yet
- NIH Public Access: Optical Imaging: New Tools For ArthritisDocument29 pagesNIH Public Access: Optical Imaging: New Tools For ArthritisMuhammad Fadli RobbyNo ratings yet
- Retraining The Brain N AddictionDocument2 pagesRetraining The Brain N Addictionandromeda.godoyNo ratings yet
- Intersubjectivity and Its Role in Schizophrenic Experience: Elizabeth PienkosDocument16 pagesIntersubjectivity and Its Role in Schizophrenic Experience: Elizabeth Pienkosburrito2000No ratings yet
- Frontsheet08 MergedDocument10 pagesFrontsheet08 MergedKarthik CsNo ratings yet
- Psychodynamic 12Document14 pagesPsychodynamic 12Muhammad ZubairNo ratings yet
- SOAP - Case Study FormatsDocument8 pagesSOAP - Case Study FormatsDr-Sanjay SinghaniaNo ratings yet
- The Cognitive Emotion Regulation QuestionnaireDocument9 pagesThe Cognitive Emotion Regulation QuestionnaireAshNo ratings yet
- Impact of The COVID-19 Pandemic On Early Child Cognitive Development: Initial Findings in A Longitudinal Observational Study of Child HealthDocument37 pagesImpact of The COVID-19 Pandemic On Early Child Cognitive Development: Initial Findings in A Longitudinal Observational Study of Child HealthDjNo ratings yet
- Breathing Affects Our Thoughts and EmotionsDocument127 pagesBreathing Affects Our Thoughts and EmotionsarbetaNo ratings yet
- Anger Management JournalDocument1 pageAnger Management JournalRidwan SyafiudinNo ratings yet
- Effects of Depression On Learning CompetencyDocument50 pagesEffects of Depression On Learning CompetencySam AlerozaNo ratings yet
- TCP AlcoholicDocument13 pagesTCP AlcoholicTracey MarieNo ratings yet
- 1985 Narcissistic Psychosomatic DisordersDocument75 pages1985 Narcissistic Psychosomatic DisordersPsiquiatría CESAME100% (1)
- Assessment of Children and AdolescentsDocument17 pagesAssessment of Children and AdolescentsadrianaNo ratings yet
- G11 HOPE Module 1Document14 pagesG11 HOPE Module 1Unk NownNo ratings yet
- Annotated BibliographyDocument6 pagesAnnotated Bibliographyapi-466357099No ratings yet
- Badhaasaa Group Research PaperDocument62 pagesBadhaasaa Group Research PaperAbebaw AmareNo ratings yet
- Efficacy of Aromatherapy On Dental AnxietyDocument39 pagesEfficacy of Aromatherapy On Dental AnxietyDafne MendozaNo ratings yet
- Phatak Materia MedicaDocument869 pagesPhatak Materia Medicaminunat55% (11)
- Introduction FinalDocument8 pagesIntroduction FinalCarl Allen MancaoNo ratings yet
- IOC Mental Health in Elite Athletes Toolkit 2021Document100 pagesIOC Mental Health in Elite Athletes Toolkit 2021Ivan Cruz (Navi Zurc)100% (1)
- Understanding Anxiety in Children and Teens: 2018 Children's Mental Health ReportDocument20 pagesUnderstanding Anxiety in Children and Teens: 2018 Children's Mental Health ReportBernard Sid AhmedNo ratings yet
- Perinatal Psychiatry: Moderator: Dr. Navkiran S. MahajanDocument51 pagesPerinatal Psychiatry: Moderator: Dr. Navkiran S. MahajanAarti GuptaNo ratings yet
- Bài Báo Sô 1 - C QuỳnhDocument3 pagesBài Báo Sô 1 - C QuỳnhTran Thi Ngoc BinhNo ratings yet
- Speeches For School Morning Assembly by Shiksha PressDocument59 pagesSpeeches For School Morning Assembly by Shiksha Pressghdfrtu42No ratings yet
- Research Arc 2 - Universal ElementsDocument9 pagesResearch Arc 2 - Universal Elementsapi-633585085No ratings yet
- Adolescent Life SkillsDocument69 pagesAdolescent Life SkillsVelprashanth VenkatesanNo ratings yet
- Criminology 23 Human BehaviorDocument8 pagesCriminology 23 Human BehaviorArnel GutierrezNo ratings yet
- Mind-Body Medicine - University of Maryland Medical CenterDocument17 pagesMind-Body Medicine - University of Maryland Medical Centerjle_dlNo ratings yet
- Dental FearDocument8 pagesDental FearShrishtiChokhaniNo ratings yet
- Lassi-Hs User'S Manual: For Those Administering The Learning and Study Strategies Inventory-High SchoolDocument32 pagesLassi-Hs User'S Manual: For Those Administering The Learning and Study Strategies Inventory-High SchoolInês SacaduraNo ratings yet
- Mental Status Examination: A. Baseline DataDocument5 pagesMental Status Examination: A. Baseline DataTherese MargaretNo ratings yet
- The Employee Assistance Treatment Planner - James M. Oher & Daniel J. Conti & Arthur E. JongsmaDocument225 pagesThe Employee Assistance Treatment Planner - James M. Oher & Daniel J. Conti & Arthur E. JongsmaSergio Mora75% (8)
- Data CollectionDocument4 pagesData CollectionAknur AnarbekovaNo ratings yet
- Nle ReviewerDocument164 pagesNle ReviewerAntipala Jo100% (6)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (158)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (250)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Feeling Great: The Revolutionary New Treatment for Depression and AnxietyFrom EverandFeeling Great: The Revolutionary New Treatment for Depression and AnxietyNo ratings yet
- Breaking the Chains of Transgenerational Trauma: My Journey from Surviving to ThrivingFrom EverandBreaking the Chains of Transgenerational Trauma: My Journey from Surviving to ThrivingRating: 4.5 out of 5 stars4.5/5 (30)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (141)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItFrom EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (107)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (561)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Emotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyFrom EverandEmotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyRating: 5 out of 5 stars5/5 (6)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackFrom EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackRating: 4.5 out of 5 stars4.5/5 (153)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- How To Get Your Sh!t Together: Overcome Anxiety, Defeat Depression, Move on from Trauma, Get Organised, Find Meaning, Follow Your DreamsFrom EverandHow To Get Your Sh!t Together: Overcome Anxiety, Defeat Depression, Move on from Trauma, Get Organised, Find Meaning, Follow Your DreamsRating: 4 out of 5 stars4/5 (8)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1247)
- Happiness Hypothesis, The, by Jonathan Haidt - Book SummaryFrom EverandHappiness Hypothesis, The, by Jonathan Haidt - Book SummaryRating: 4.5 out of 5 stars4.5/5 (95)
- Decluttering at the Speed of Life: Winning Your Never-Ending Battle with StuffFrom EverandDecluttering at the Speed of Life: Winning Your Never-Ending Battle with StuffRating: 4.5 out of 5 stars4.5/5 (578)
- Beyond Thoughts: An Exploration Of Who We Are Beyond Our MindsFrom EverandBeyond Thoughts: An Exploration Of Who We Are Beyond Our MindsRating: 4.5 out of 5 stars4.5/5 (7)