Professional Documents
Culture Documents
Gender Differences in The Reporting of Physical.6
Gender Differences in The Reporting of Physical.6
Uploaded by
somya mathurOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Gender Differences in The Reporting of Physical.6
Gender Differences in The Reporting of Physical.6
Uploaded by
somya mathurCopyright:
Available Formats
Gender Differences in the Reporting of Physical and Somatoform Symptoms
Downloaded from http://journals.lww.com/psychosomaticmedicine by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbs
IHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 08/06/2023
KURT KROENKE, MD AND ROBERT L. SPITZER, MD
Objective: Women have consistently been shown to report greater numbers of physical symptoms. Our aim in this study was to
assess gender differences for specific symptoms and to assess how much of these differences were attributable to psychiatric
comorbidity. Method: Data from the PRIME-MD 1000 study (1000 patients from four primary care sites evaluated with the Primary
Care Evaluation of Mental Disorders interview) were analyzed to determine gender differences in the reporting of 13 common
physical symptoms. The effect of gender on symptom reporting was assessed by multivariate analysis, adjusting for depressive and
anxiety disorders as well as age, race, education, and medical comorbidity. Results: All symptoms except one were reported more
commonly by women, with the adjusted odds ratios (typically in the 1.5-2.5 range) showing statistically significant differences for
10 of 13 symptoms. Somatoform (ie, physically unexplained) symptoms were also more frequent in women. Although depressive
and anxiety disorders were the strongest correlate of symptom reporting, gender had an independent effect that persisted even after
adjusting for psychiatric comorbidity. Gender was the most important demographic factor associated with symptom reporting,
followed by education. Conclusions: Most physical symptoms are typically reported at least 50% more often by women than by
men. Although mental disorders are also more prevalent in women, gender influences symptom reporting in patients whether or not
there is psychiatric comorbidity. Key words: somatization, gender, depression, anxiety, prevalence.
associated with increased reporting of physical symptoms (2,
PRIME-MD = Primary Care Evaluation of Mental 7, 18). Failure to adjust for this potent confounder weakens
Disorders; PQ = patient questionnaire; CEG = Clinician conclusions about the independent effect of gender on symp-
Evaluation Guide. tom reporting.
The burden of physical symptoms in primary care coupled
with their excess prevalence among women makes additional
INTRODUCTION understanding of gender differences an important issue in
Symptoms such as back pain, headache, gastrointestinal women's health. In this paper, we analyze data from a large
disturbances, musculoskeletal pain, fatigue, dizziness, and mental health survey conducted in four primary care clinics to
other physical complaints are the leading reason for outpatient answer several questions:
visits and are associated with substantial disability and health 1. What are the differences between women and men in
care utilization (1-4). Because the cause and treatment of such their reporting of the most common symptoms seen in
complaints is less clearcut than well-defined diseases (2-4), primary care?
clinicians find the evaluation and management of physical
2. Are gender differences restricted to certain symptoms or
symptoms particularly challenging and difficult (5-7).
"generic" across most types of symptoms?
Women have consistently been shown to report symptoms
more frequently than men. Theories to account for this gender 3. Are gender differences similar for the subset of physical
difference include physiological, sociocultural, and psycho- symptoms that are medically unexplained?
logical explanations (8—10). 4. What is the independent effect of gender on symptom
reporting, controlling not only for demographic character-
Previous studies evaluating gender differences in symptom istics, but also current depressive and anxiety disorders?
reporting have had several limitations. First, some studies
have focused on persons residing in the general population METHODS
rather than those seeking health care, making it more difficult
to be certain what proportion of symptoms were, in fact, PRJME-MD 1000 Study
significant clinically (11-13). Second, the extensive literature Data was analyzed from the PRIME-MD 1000 study, a mental
health survey of 1000 patients in four primary care sites (hospital-
on somatization disorder (14—16)—a chronic mental disorder based group practice in Boston; city hospital clinic in New York;
occurring predominantly in women and characterized by large general medicine clinic serving military beneficiaries in Washington
numbers of unexplained symptoms, substantial impairment, DC; and family practice clinic in Mobile). Of the 1360 patients
and excessive health care utilization—is not generalizable to presenting for medical care who were approached, 1000 enrolled in
the majority of symptomatic patients in primary care. Third, the study and provided complete data. Reasons for nonparticipation
researchers often analyze total symptom counts without pro- included previous evaluation with PRIME-MD (N = 109), not
viding details on individual symptoms, so it is unclear whether providing informed consent (N = 89), inability to speak English
women are more likely to report all or most symptoms or only (N = 81), too ill (N = 53) and other (N = 28). The first 369 patients
certain specific symptoms. were selected by convenience but independently of the participating
physicians' knowing that a patient had psychopathology, whereas the
Fourth and most importantly, few studies have adequately remaining 631 patients were selected using site-specific methods to
controlled for patient characteristics and, in particular, psychi- avoid sampling bias. Within each site, the convenience sample and
atric comorbidity. Depressive and anxiety disorders are not the consecutive or randomly selected sample did not differ signifi-
only more prevalent in women (14, 17), but are strongly cantly in terms of age, sex, ethnicity, education, functional status, or
frequency of PRIME-MD diagnoses. Medical comorbidity was
assessed by asking the patient's physician to note the presence of
nine types of general medical disorders: hypertension, diabetes,
From the Regenstrief Institute for Health Care and Department of Medicine, Indiana arthritis, heart disease, pulmonary disease, renal disease, liver disease,
University School of Medicine, Indianapolis, Indiana (K.K.); Biometrics Research cancer, and other diseases. Details of the PRIME-MD study including
Department, New York State Psychiatric Institute and the Department of Psychiatry, patient sampling procedures have been previously described (19). The
Columbia University, New York, New York (R.L.S.). study protocol was approved by the institutional review boards of each
Address reprint requests to: Kurt Kroenke, MD, Regenstrief Institute for Health Care,
1001 West 10th Street, RG-6, Indianapolis, IN 46202. site, and each patient gave signed, informed consent.
Received for publication January 22, 1997; revision received May 20, 1997. All subjects were evaluated with PRIME-MD, a validated diag-
150 Psychosomatic Medicine 60:150-155 (1998)
0033-3174/98/6002-0150S03.00/0
Copyright © 1998 by the Americai Psychosomatic Society
GENDER DIFFERENCES IN PHYSICAL AND SOMATOFORM SYMPTOMS
nostic interview that consists of a 26-item self-administered patient disorders. Finally, to examine for the possibility of interaction
Downloaded from http://journals.lww.com/psychosomaticmedicine by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbs
questionnaire (PQ) and an accompanying clinician evaluation guide between gender and psychiatric comorbidity, a three-factor analysis
IHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 08/06/2023
(CEG) (19). Criteria-based DSM III-R diagnoses were made in five of variance was performed with number of physical symptoms as the
categories: depressive, anxiety, somatoform, alcohol, and eating. In dependent variable and sex, depressive disorder, and anxiety disorder
the validation study, 431 of the 1000 patients underwent a semistruc- as the three independent variables.
tured telephone reinterview by a mental health professional who was
blinded to the results of the PRIME-MD interview that had been
completed within the past 48 hours or less. The reinterviewed RESULTS
patients were similar to patients not reinterviewed in terms of Patient Characteristics
demographic profile, functional status, and frequency of psychiatric Patients had a mean age of 55 years (range, 18-91); 60%
diagnoses. Agreement between PRIME-MD and telephone reinter-
view diagnoses for depressive and anxiety disorders was satisfactory were women, 58% were white, and 28% were college gradu-
(kappa of 0.61 and 0.55, respectively) and approximates the levels of ates. Compared with men, there were more minority (non-
agreement among mental health professionals using diagnostic inter- white) women (48% vs 34%, p < .0001) and fewer with
view schedules (20, 21). Construct validity of the instrument was college degrees (21% vs 39%, p < .0001). There were no
supported additionally by strong associations between PRIME-MD gender differences in terms of age or number of chronic
psychiatric diagnoses and functional status measures, health care utili- medical disorders. The most common comorbid medical
zation, and validated self-rated psychiatric symptom severity scales (19). conditions were hypertension (48% of all patients), arthritis
The somatoform section of the PQ inquires about 15 physical (23%), diabetes (17%), and cardiac disease (15%). The
symptoms or symptom clusters that account for over 90% of physical number of types of current medical disorders was none in 18%
complaints (excluding upper respiratory symptoms) reported in the of the patients, one in 34%, two in 29%, three in 14%, and
outpatient setting (1-3). These 15 symptoms are: stomach pain, back four or more in 5%. A DSM-III-R psychiatric diagnosis was
pain, headache, chest pain, dizziness, fainting, palpitations, shortness present in 26% of the patients, and an additional 13% had a
of breath, bowel complaints (constipation or diarrhea), dyspeptic
complaints (nausea, gas, or indigestion), fatigue, trouble sleeping, subthreshold diagnosis. Depressive and anxiety disorders were
pain in joints or limbs, menstrual pain or problems, and pain or present in 26% and 18% of the patients, respectively.
problems during sexual intercourse. For this study, fainting (because
of its low prevalence) and menstrual symptoms (which occur only in
Individual Symptoms
women) are excluded from the analysis.
The symptoms are prefaced in the PQ by the query: "During the Table 1 summarizes the frequency of physical symptoms
past month, have you been bothered a tor by . . . Stomach pain? Back according to gender. The first columns displaying all symp-
pain? . . ." In the original study, clinicians entered the CEG somato- toms (both physically explained and somatoform) show that
form module for any patient who endorsed three or more physical every symptom except one is more prevalent in women. Ten
symptoms on the PQ. In the CEG, the clinician is asked to decide: of the 13 symptoms are significantly more common in women,
"Based on your clinical judgment, does the symptom have a physical with most of these differences being highly significant (p <
explanation that is adequate to explain its severity and associated .001). Only abdominal pain and chest pain have a similar
disability?" Symptoms for which the clinician answered "No" were
classified as somatoform. An important exception is that if the patient frequency among women and men, and the sexual symptom
meets criteria for a depressive or anxiety disorder, symptoms explicitly ("pain or problems during sexual intercourse") is the single
part of the diagnostic criteria for that disorder (eg, fatigue or insomnia for symptom noted more commonly by men.
a depressive disorder; cardiopulmonary or gastrointestinal symptoms for Somatoform symptoms were also significantly more fre-
panic disorder) are not counted as somatoform. In summary, it was the quent in women (second set of columns in Table 1). We also
patient's own physician (ie, the one administering the PRIME-MD determined for each symptom how often clinicians judged the
interview) who made the final decision as to whether a particular symptom to be somatoform. Each symptom, except sexual
symptom was classified as somatoform. problems, was more likely to be considered somatoform in
women than in men, with the greatest differences being for
Statistical Analysis abdominal pain (24% vs 17%), back pain (19% vs 11%),
For both individual symptoms and symptom counts, two depen- bowel complaints (27% vs 16%), chest pain (29% vs 25%),
dent variables were analyzed: all physical symptoms and somatoform dizziness (30% vs 22%), dyspnea (22% vs 13%), headache
symptoms. In assessing headache, for example, the first analysis (34% vs 22%), joint or limb pain (15% vs 8%), and nausea or
would include all patients reporting headache, whereas the second indigestion (26% vs 19%).
analysis would include only those with medically unexplained head-
aches. Chi-square analysis was used to assess the univariate relationship Table 2 displays the likelihood of each symptom being
between gender and reporting of the 13 physical symptoms. Logistic reported by women compared with men. Odds ratios are
regression analysis was used to determine the independent effect of presented in two ways: 1) adjusted for age, race, education,
gender of symptom reporting. Odds ratios were adjusted for each and number of general medical disorders; 2) psychiatric-
symptom in two steps: the first controlled for age, race, education, and adjusted, ie, adjusting for these same variables, plus the
medical comorbidity (expressed as the number of general medical presence of depressive and anxiety disorders. These odds
disorders); the second controlled for these factors plus depressive and ratios are presented both for all physical symptoms (eg, all
anxiety disorders (each represented by a binary variable coding the
disorder as present or absent). This allowed us to assess (by change in patients with headache) and somatoform symptoms (ie, only
odds ratio) how much the gender effects were due to psychiatric those patients whose headache is medically unexplained).
comorbidity. The effect of gender on somatoform symptoms was also Similar to the univariate analysis results (Table 1), the odds
assessed by using the same logistic regression procedure. ratios in Table 2 demonstrate that most physical symptoms are
Multivariate linear regression was used to determine the effect of more common in women, usually on the order of one and a
gender on total symptom counts. Variables were entered stepwise in half to two times more likely. Furthermore, adjusting for
three groups: 1) sex, age, education, and race; 2) medical comorbid- psychiatric comorbidity only slightly altered the odds ratios.
ity; 3) psychiatric comorbidity, ie, presence of depressive and anxiety Adding depressive and anxiety disorders to the logistic regres-
Psychosomatic Medicine 60:150-155 (1998)
K. KROENKE A N D R. L. SPITZER
TABLE 1. Frequency of Physical Symptoms by Gender in 1000 Primary Care Patients
Downloaded from http://journals.lww.com/psychosomaticmedicine by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbs
IHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 08/06/2023
All Physical Symptoms Somatoform Symptoms
Symptom
Women Men Women Men
p p
(N = 569) (N = 385) (W = 532) (N = 358)
(% of patients reporting symptom)
Abdominal pain 21.1 17.9 .23 5.1 3.1 .15
Back pain 46.4 33.8 .0001 8.9 3.6 .002
Bowel complaints 33.2 22.9 .0005 8.9 3.7 .002
Chest pain 23.0 18.4 .09 6.6 4.5 .18
Dizziness 28.8 15.8 <.00001 8.7 3.4 .002
Dyspnea 36.2 24.7 .0002 8.1 3.1 .002
Headache 46.2 22.1 •c.OOOOl 15.6 4.8 <.00001
Fatigue 66.8 45.2 <.00001 12.7 8.1 .03
Insomnia 38.3 26.8 .0002 6.9 4.5 .14
Joint or limb pain 65.2 49.4 <.00001 9.8 3.9 .001
Nausea/indigestion 48.3 37.4 .0009 12.7 7.0 .007
Palpitations 32.7 19.2 <.00001 8.9 5.3 .047
Sexual problems 4.7 9.1 .008 1.1 2.2 .19
TABLE 2. Increased Likelihood of Physical Symptoms in Women
All Physical Symptoms Somatofor m Symptoms
Symptom
Adjusted Odds Ratio Psychiatric-Adjusted Adjusted Odds Ratio Psychiatric-Adjusted
(95% CI)° Odds Ratio (95% CI) 6 (95% CI)" Odds Ratio (95% CI)"
Headache 2.8 (2.1,3.9) 2.6(1.9,3.7) 3.6 (2.0,6 6) 3.2(1.5,5.9)
Fatigue 2.3(1.7,3.0) 2.1 (1.5,2.8) 1.8(1.1,3.0) 1.7(1.0,2.8)
Dizziness 2.0(1.4,2.9) 1.8(1.3,2.6) 2.7(1.3,5.5) 2.2(1.1,4.7)
Joint or limb pain 1.8(1.4,2.5) 1.7(1.2,2.2) 2.3(1.2,4.4) 1.8(0.9,3.5)
Palpitations 1.9(1.3,2.6) 1.7 (1.2,2.4) 1.4(0.8,2.5) 1.1 (0.6,2.1)
Dyspnea 1.8(1.2,2.4) 1.6(1.1,2.2) 3.1 (1.5,6.2) 2.6(1.2,5.4)
Back pain 1.7(1.3,2.3) 1.5(1.1,2.1) 2.2(1.1,4.4) 1.9(1.0,3.8)
Bowel complaints 1.6(1.2,2.2) 1.5(1.1,2.1) 2.3(1.2,4.4) 2.0(1.0,3.8)
Insomnia 1.6(1.2,2.2) 1.3(0.9,1.9) 1.6(0.8,3.1) 1.4(0.7,2.7)
Nausea/indigestion 1.5(1.1,2.0) 1.4(1.0,1.8) 1.6(1.0,2.7) 1.4(0.8,2.4)
Chest pain 1.2(0.9,1.8) 1.1 (0.8,1.6) 1.3(0.7,2.5) 1.0(0.5,2.0)
Abdominal pain 1.1 (0.8,1.6) 1.0(0.7,1.4) 1.1 (0.5,2.4) 0.9 (0.4,2.0)
Sexual problems 0.5 (0.3,0.8) 0.4 (0.3,0.8) 0.4(0.1,1.3) 0.3(0.1,1.1)
" Adjusted odds ratios are adjusted for age, race, education, and number of general medical disorders.
b
Psychiatric-adjusted odds ratios are adjusted for above factors, plus depressive and anxiety disorders.
sion model typically lowered the adjusted odds ratios only 0.1 groups, the addition of medical comorbidity in the second step
to 0.2 (only one symptom changing by as much as 0.3). did not significantly change the strength of association of the
The odds of reporting somatoform symptoms (second set of demographic variables entered in the first step in either the model
columns in Table 2) was also greater in women for most for all physical symptoms or the model for somatoform symp-
symptoms. Because the base rate of somatoform symptoms for toms. Therefore, in Table 3 we display the results of two models:
both women and men is low, confidence intervals are wider Model 1 adjusts for demographic characteristics and medical
and fewer of the adjusted odds ratios are statistically signifi- comorbidity, and Model 2 further adjusts for psychiatric comor-
cant. Again, adjusting for psychiatric comorbidity only bidity. Three parameters are reported (22). The unstandardized
slightly lowered the odds ratios. regression coefficient, /3, is a measure of the independent effect
One question on the PRIME-MD questionnaire screens for of a particular variable on symptom counts, controlling for all
hypochondriacal concerns by asking the patient: "Have you other variables. The standardized regression coefficient, Beta
often been bothered by the thought that you have a serious (which is /3 divided by the standard error of /3), is one means of
undiagnosed disease." In responding to this item, women were comparing variables with one another: those with a larger beta
not more likely to express serious illness worry (adjusted odds are typically stronger predictors. Partial B? is an estimate of the
ratio 1.08; 95% CI, 0.7-1.7; p = .71).
amount of variance in total symptom count that is explained by
Total Symptom Counts a variable.
Multivariable linear regression was performed to determine Examining total symptom count first, the |3 for sex in
the independent effect of specific variables on symptom report- Model 1 indicates that women on average report an additional
ing. Although we stepped variables into the model in three 1.47 physical symptoms compared with men. Model 2 shows
Psychosomatic Medicine 60:150-155 (1998)
Downloaded from http://journals.lww.com/psychosomaticmedicine by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbs
IHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 08/06/2023
GENDER DIFFERENCES IN PHYSICAL AND SOMATOFORM SYMPTOMS
TABLE 3. Predictors of Total Number of Physical Symptoms"
All Physical Symptoms' Somatoform Symptoms'7
Model 1 Model 2 Model 1 Model 2
Variable
Partial Partial Partial Partial
Beta
R2 /3 Beta
R2 P Beta
R2 J8 Beta
R2
Depressive disorder 2.54 .331 .237 0.83 .188 .030
Anxiety disorder 2.02 .231 .052 1.10 .222 .110
Female sex 1.47 .216 .067 1.10 .162 .031 0.54 .138 .026 0.43 .110 .011
Education -0.56 .219 .042 -0.32 .125 .008 -0.18 .125 .012 ns ns ns
Medical comorbidity 0.46 .165 .019 0.45 .159 .022 ns ns ns ns ns ns
(no. diseases)
Age (in decades) -0.35 .171 .008 -0.20 .096 .006 -0.17 .145 .009 -0.08 .070 .004
" All variables are significant atp < .001 except: age in Model 2 for all physical symptoms (p = .003) and for somatoform symptoms (p = .03), and variables
listed as NS (ie, not significant).
'' /3 and Beta are unstandardized and standardized regression coefficients, respectively. Model 1 includes sex, age, education, number of physical diseases, and
race as independent variables. Model 2 includes these same variables, plus presence of depressive and anxiety disorders.
that psychiatric disorders have the strongest association with number of symptoms reported was significantly greater in
symptom reporting: the number of additional physical symp- women among patients with no disorder (F = 40.05, p <
toms associated with a depressive or anxiety disorder is 2.54 .001) and approached significance in those with only an
and 2.02, respectively. However, female sex is still associated anxiety disorder (F = 3.16, p = .08) and both an anxiety and
with 1.1 additional symptoms even after controlling for psychi- depressive disorder (F = 3.28, p = .07). On the other hand,
atric comorbidity. The partial R2 values in Model 1 show that symptom counts were similar in men and women who had
gender accounts for 6.7% of the variance in symptom reporting; only a depressive disorder, confirming the interaction detected
education, 4.2%; the number of medical disorders, 1.9%; and by ANOVA and suggesting that depressive disorders may
age, 0.8%. Although adding psychiatric disorders in Model 2 have a greater influence on symptom reporting in men.
shows the substantial proportion of variance attributable to
depressive (23.7%) and anxiety (5.7%) disorders, gender still DISCUSSION
accounts for more of the variance (3.1%) than the other nonpsy- Our study has several important findings. First, increased
chiatric variables. This is confirmed by examination of the symptom reporting in women is a generic phenomenon rather
standardized regression coefficients: psychiatric disorders have than one restricted to certain types of symptoms. Second,
the largest beta, followed by gender. medically unexplained symptoms are also more common in
Table 3 also shows the association between these same women. Third, the effect of gender on symptom reporting is
variables and the reporting of somatoform symptoms. Again, independent of psychiatric comorbidity.
psychiatric disorders have the greatest effects, and gender
continues to be the strongest nonpsychiatric predictor. The
negative regression coefficients for age and education indicate 10
that younger patients and those with less education tend to
report more symptoms. Regarding somatoform symptoms,
medical comorbidity does not have a significant effect in
either Model 1 or Model 2, whereas the effect of education is
no longer significant after adjusting for psychiatric comorbid-
ity. Interestingly, anxiety disorders explain a greater propor-
tion of the variance in somatoform symptom reporting than do
depressive disorders (11% and 3%, respectively).
The only significant interaction between gender and psychi-
atric disorders was between gender and depressive disorders for
predicting total physical symptom count. In this three-factor
ANOVA, depressive disorders had the strongest association (F =
71.8, p < .001), followed by anxiety disorders (F = 54.1, p <
.001), sex (F = 18.0, p < .001), and the interaction between sex
and depressive disorders (F = 5.0, p = .026). There was no
interaction between sex and anxiety disorders or between anxiety
and depressive disorders in predicting total physical symptom Neither Anxiety Depression Both
count. Also, there were no significant interactions between any of
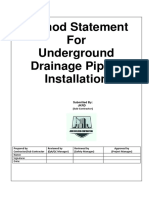
the factors in the ANOVA where somatoform symptom count Figure 1. The number of men/women classified into four psychiatric disor-
der categories was: neither anxiety or depression, 296/358; anxiety only, 16/35;
was the dependent variable. depression only, 40/86; and both anxiety and depression, 33/90. Gender differ-
Figure 1 illustrates the effects of gender and psychiatric ences were significant for neither (F = 40.05, p < .001) and approached
disorders on total physical symptom reporting. The mean significance for anxiety (F = 3.16, p = .08) and both (F = 3.28, p = .07).
Psychosomatic Medicine 60:150-155 (1998)
K. KROENKE A N D R. L. SPITZER
Numerous theories supported by varying degrees of evi- diagnostic criteria for a depressive or anxiety disorder were
Downloaded from http://journals.lww.com/psychosomaticmedicine by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbs
dence have been proposed to account for increased symptom not counted as somatoform in a particular patient if he or she
IHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 08/06/2023
reporting in women (8-10). One difference may be at the met diagnostic criteria for that mental disorder. Because panic
physiological level: laboratory and field studies have shown disorder was only diagnosed in a small proportion (4%) of
that women are more sensitive to external environmental cues patients, fatigue and insomnia (the PRIME-MD physical
(including stress) and men to internal physiological stimuli in symptoms included in all depressive disorder criteria as well
noticing, defining and reacting to physical symptoms (8, 23). as generalized anxiety disorder) are the two symptoms that
Secondly, certain psychosocial factors more prevalent in might have been substantively affected. Had these two symp-
women are strongly associated with symptom reporting, toms been classified as somatoform even in the presence of a
particularly depressive and anxiety disorders (2, 7, 17), as well diagnosed depressive disorder or generalized anxiety disorder,
as a history of sexual or physical abuse (24-26). Other the overall frequency of these symptoms (as well as gender
psychosocial antecedents that have been postulated include differences) would not have changed, but more fatigue and
cultural factors permitting less stoicism and greater expres- insomnia would have been classified as somatoform.
siveness among women; amplification of somatic symptoms; Only 3 of 13 symptoms were not significantly more
a lower threshold for seeking health care; and gender differ- common in women. Women would not be expected to report
ences in social roles and responsibilities (8-10, 27). chest pain more frequently, inasmuch as coronary artery
Although our study cannot address all of these theories, it disease is more prevalent in men (in our sample, cardiac
is stronger than most previous studies in controlling for disease was present in 21% of men vs 11% of women, p =
psychiatric comorbidity. Depressive and anxiety disorders .0001). The lack of differences regarding abdominal pain is
clearly had the strongest association with symptom reporting, more surprising because irritable bowel syndrome and other
and adjusting for these disorders did reduce the effect of functional abdominal complaints have been reported as more
gender. Even after adjustment, however, gender effect re- prevalent in women. However, irritable bowel syndrome is a
mained significant and stronger than the effect of other constellation of symptoms that includes bowel complaints as
demographic variables. Because depressive and anxiety dis- well as upper gastrointestinal symptoms such as bloating.
orders are both more prevalent in women and also powerful Both the bowel complaint item (constipation or diarrhea) and
correlates of symptom reporting, the independent effect of the upper gastrointestinal symptom item (nausea, indigestion,
gender is of particular interest. or gas) on PRIME-MD were endorsed more commonly by
Purported differences between women and men in their women in our sample. It is possible that the lack of a gender
threshold for seeking care for minor illness is also unlikely to difference for abdominal pain is a chance finding due to
explain the gender differences in symptom reporting revealed multiple statistical comparisons. Only pain or problems during
in our sample. All subjects in the PRIME-MD 1000 study sexual intercourse were more frequently reported by men.
(women and men) were seeking health care, and there were no Whether this is due to a higher prevalence of sexual problems
gender differences in age or medical comorbidity. Addition- in men or underreporting of this particular symptom in women
ally, the findings in our clinic sample are complemented by requires additional investigation.
two large population-based surveys where most symptoms The greater reporting of most symptoms, as well as
were more prevalent in women (11, 12). Thus, results from unexplained symptoms, may account for the increased prev-
clinical and community samples are consistent with and alence of functional syndromes among women, including
suggest that increased symptom reporting in women is not irritable bowel syndrome, fibromyalgia, chronic fatigue syn-
merely an artifact of higher health care utilization. drome, and migraine headache (8, 30, 31). These disorders are
Although few patients (2%) in our sample met full diag- defined predominantly by symptoms for which the precise
nostic criteria for hypochondriasis, 14% responded affirma- etiology and pathophysiology is yet to be established.
tively to the question: "During the past month, have you often Depressive and anxiety disorders were both strongly asso-
been bothered by the thought that you have a serious undiag- ciated with symptom reporting, yet differed in several re-
nosed disease?" The fact that similar proportions of women spects. Depression had a greater effect on total symptom
and men acknowledged serious illness worry suggests that reporting while anxiety had a somewhat greater effect on the
gender-related differences in symptom reporting is not a reporting of somatoform (ie, medically unexplained) symp-
consequence of excess illness worry among women. Previous toms. Second, the interaction between gender and depressive
studies have similarly shown a higher prevalence of somati- disorders (ie, men and women who only had depression
zation, but not hypochondriacal concerns in women (27, 28). reported a similar number of symptoms) did not exist between
Women also had a higher prevalence of somatoform gender and anxiety disorders.
symptoms. Although some of this could simply be because of Our study has several limitations. Physical symptoms were
increased symptom reporting in general, the proportion of measured by patient responses to a symptom checklist rather
symptoms considered unexplained in women was also greater than limiting our analysis to spontaneously volunteered "chief
for most symptoms. Certainly, this is consistent with the complaints." Although this might inflate the true prevalence of
extensive literature on gender differences in somatization and clinically significant symptoms, we did ask patients to report
somatoform disorders (7, 8, 13-15, 27-29). Still, inasmuch as only those that had bothered them a lot, and the same measure
deciding that a symptom lacks an adequate physical explana- was used for women and men. Second, classification of a
tion requires clinical judgment, clinicians and investigators symptom as somatoform was done by the primary care
alike must be careful to distinguish true differences from clinician and we cannot exclude the possibility of gender bias
potential gender biases in labeling symptoms somatoform. in labeling symptoms somatoform. The extent to which bias
Consistent with the DSM-III-R (and DSM-IV) classifica- actually exists in clinical practice is not well established and
tion, physical symptoms that were specifically part of the warrants further study. Furthermore, gender bias in research
154 Psychosomatic Medicine 60:150-153 (1998)
GENDER DIFFERENCES IN PHYSICAL AND SOMATOFORM SYMPTOMS
may mean that women's health problems are less studied and 12. Hammond EC: Some preliminary findings on physical com-
Downloaded from http://journals.lww.com/psychosomaticmedicine by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbs
less well understood, making it more likely that symptoms in plaints from a prospective study of 1,064,004 men and women.
IHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 08/06/2023
women might be interpreted as "unexplained." Third, we were Am J Public Health 54:11-23, 1964
better able to study and control for certain explanatory 13. Escobar JI, Burnam A, Karno M, et al: Somatization in the
variables (eg, demographic characteristics and psychiatric community. Arch Gen Psychiatry 44:713-718, 1987
comorbidity) than for other potential sociocultural or biolog- 14. Swartz M, Landerman R, George LK, et al: Somatization
ical mechanisms. Fourth, medical comorbidity was defined disorder. In Robins LN, Regier DA (eds), Psychiatric Disorders
simply as the number of general medical conditions; although in America. New York, The Free Press, 1991, 220-257
some epidemiologic studies have used this as an estimate of 15. Smith GR: Somatization disorder and undifferentiated somato-
comorbidity (32), more sophisticated measures also factor in
form disorder. In Gabbard GO (ed), Treatments of Psychiatric
illness severity.
Disorders, 2nd Edition. Washington DC, American Psychiatric
Physical symptoms play a prominent role in outpatient Press, 1995, 1718-1733
practice. The fact that gender is associated with both symptom
16. Keller R: Somatization and Hypochondriasis. New York, Prae-
prevalence as well as the likelihood that symptoms will be
ger, 1986
considered unexplained, make the evaluation and management
of physical symptoms a particularly salient issue in women's 17. Linzer M, Spitzer R, Kroenke K, et al: Gender, quality of life,
health. Depressive and anxiety disorders alone do not account and mental disorders in primary care: Results from the
for increased symptom reporting in women. Continuing re- PRIME-MD 1000 study. Am J Med 101:526-533, 1996
search is required to better explore the relative contributions 18. Katon W, Lin E, Von Korff M, et al: Somatization: A spectrum
of sociocultural factors, biological variables, sexual and phys- of severity. Am J Psychiatry 148:34-40, 1991
ical abuse, and other potential etiologies. 19. Spitzer RL, Williams JBW, Kroenke K, et al: Utility of a new
procedure for diagnosing mental disorders in primary care: The
The development of PRIME-MD was underwritten by an PRIME-MD 1000 study. JAMA 272:1749-1756, 1994
unrestricted educational grant from the Roerig and Pratt 20. Williams JBW, Gibbon M, First MB, et al. The Structured
Pharmaceuticals division of Pfizer Inc, New York, New York. Clinical Interview for DSM-III-R (SCID). II. Multisite test-retest
Also, the authors are grateful for the assistance of the reliability. Arch Gen Psychiatry 49:630-636, 1992
following PRIME-MD collaborators: Janet Williams, Steven 21. Andreasen NC, Flaum M, Arndt S: The Comprehensive Assess-
Hahn, Mark Linzer, Frank deGruy, and David Brody.
ment of Symptoms and History (CASH): An instrument for
REFERENCES assessing diagnosis and psychopathology. Arch Gen Psychiatry
1. Schappert SM: National Ambulatory Medical Care Survey: 1989 49:615-623, 1992
summary. National Center for Health Statistics. Vital Health Stat 22. Weisberg S. Applied Linear Regression, 2nd Edition. New York,
Series 13, No. 10, 1992 John Wiley & Sons, 1985
2. Kroenke K, Spitzer RL, Williams JBW, et al: Physical symptoms 23. Pennebaker JW: The Psychology of Physical Symptoms. New
in primary care: Predictors of psychiatric disorders and func- York, Springer-Verlag, 1982
tional impairment. Arch Fam Med 3:774-779, 1994 24. McCauley J, Kern DE, Kolodner K, et al: The "battering
3. Kroenke K, Arrington ME, Mangelsdorff AD: The prevalence of syndrome": Prevalence and clinical characteristics of domestic
symptoms in medical outpatients and the adequacy of therapy. violence in primary care internal medicine practices. Ann Intern
Arch Intern Med 150:1685-1689, 1990 Med 123:737-746, 1995
4. Kroenke K, Mangelsdorff AD: Common symptoms in ambula- 25. Drossman DA, Talley MJ, Leserman J, et al: Sexual and physical
tory care: Incidence, evaluation, therapy, and outcome. abuse and gastrointestinal illness: Review and recommendations.
Am J Med 86:262-266, 1989 Ann Intern Med 123:782-794, 1995
5. Hahn SR, Thompson KS, Wills TA, et al: The difficult doctor- 26. Springs FE, Friedrich WN: Health risk behaviors and medical
patient relationship: Somatization, personality, and psychopa- sequelae of childhood sexual abuse. Mayo Clin Proc 67:527-
thology. J Clin Epidemiol 47:647-657, 1994 532, 1992
6. Hahn SR, Kroenke K, Spitzer RL, et al: The difficult patient: 27. Barsky AJ, Wyshak G: Hypochondriasis and somatosensory
Prevalence, psychopathology, and functional impairment. J Gen amplification. Br J Psychiatry 157:404-409, 1990
Intern Med 11:1-8, 1996
28. Kirmayer LJ, Robbins JM: Three forms of somatization in
7. Katon W, Kleinman A, Rosen G: Depression and somatization:
primary care: Prevalence, co-occurrence, and sociodemographic
A review. Am J Med 72:127-135, 241-247, 1982
characteristics. J Nerv Ment Dis 179:647-655, 1991
8. Kirmayer LJ, Robbins JM (eds): Current Concepts of Somatiza-
tion: Research and Clinical Perspectives. Washington DC. 29. Andersen R, Francis A, Lion J, et al' Psychologically related
American Psychiatric Press, 1991 illness and health services utilization. Med Care 15:59-73, 1977
9. Verbrugge LM: Gender and health: An update on hypotheses and 30. Kellner R: Psychosomatic Syndromes and Somatic Symptoms.
evidence. J Health Soc Behav 26:156-182. 1985 Washington DC, American Psychiatric Press, 1991
10. Wool CA, Barsky AJ: Do women somatize more than men? Gender 31. Bass C (ed). Somatization: Physical Symptoms and Psycholog-
differences in somatization. Psychosomatics 35:445-452, 1994 ical Illness. London, Black well Scientific Publications, 1990
11. Kroenke K, Price RK: Symptoms in the community: Prevalence, 32. Guralnik JM, LaCroix AZ, Everett DF: Comorbidity of chronic
classification, and psychiatric comorbidity. Arch Intern Med conditions and disability among older persons—United States,
153:2474-2480, 1993 1984. Morb Mortal Wkly Rep (MMWR) 38:788-791, 1989
Psychosomatic Medicine 60:150-155 (1998) 155
You might also like
- The Premenstrual Symptoms Screening Tool (PSST) For CliniciansDocument7 pagesThe Premenstrual Symptoms Screening Tool (PSST) For CliniciansManju Goswami100% (1)
- Premenstrual Dysphoric Disorder Burden of IllnessDocument11 pagesPremenstrual Dysphoric Disorder Burden of IllnessLili Bodhert MNo ratings yet
- SAB CHCCOM005 CHCLEG001 Work Legally and EthicallyDocument95 pagesSAB CHCCOM005 CHCLEG001 Work Legally and EthicallyBibash Tripathi28% (53)
- Test: Module 6 Vocabulary: PIONEER Beginners - American EditionDocument3 pagesTest: Module 6 Vocabulary: PIONEER Beginners - American EditionMiguel Angel Alvarado100% (1)
- Psychosocial Dimensions of Displacement: Prevalence of Mental Health Outcomes and Related Stressors Among Idps in IraqDocument34 pagesPsychosocial Dimensions of Displacement: Prevalence of Mental Health Outcomes and Related Stressors Among Idps in IraqSocial InquiryNo ratings yet
- Method Statement For Underground Drainage Piping InstallationDocument8 pagesMethod Statement For Underground Drainage Piping InstallationUSAMANo ratings yet
- Annual Record of Homœopathic Literature.1874Document390 pagesAnnual Record of Homœopathic Literature.1874GustavoMarceloDareNo ratings yet
- ESP Worksheet OPTOMETRY - A1 - READING - What Is An OptometristDocument2 pagesESP Worksheet OPTOMETRY - A1 - READING - What Is An OptometristYelixe Manrique Ibañez100% (1)
- Eng7-Q4-iP5-v.02 Distinguishing Features of Selected Literary Genres During The Conteporary PeriodDocument8 pagesEng7-Q4-iP5-v.02 Distinguishing Features of Selected Literary Genres During The Conteporary PeriodreiyaNo ratings yet
- Fuel SystemDocument41 pagesFuel SystemSam100% (3)
- Nissan CaseDocument6 pagesNissan CaseUtchash Shahriar100% (1)
- Depression and Anxiety in Multisomatoform DisorderDocument4 pagesDepression and Anxiety in Multisomatoform DisorderAdeyemi OlusolaNo ratings yet
- Care MD ApproachDocument7 pagesCare MD ApproachDewina Dyani Rosari IINo ratings yet
- Nelson en Ingles Capitulos 16 A 20Document81 pagesNelson en Ingles Capitulos 16 A 20Mario TurichNo ratings yet
- BMJ 334 7593 CR 00579Document10 pagesBMJ 334 7593 CR 00579RonaMaulidiaBakhitaNo ratings yet
- Associations Between Neuropsychiatric Symptoms Mujeres Vs HombresDocument15 pagesAssociations Between Neuropsychiatric Symptoms Mujeres Vs HombresCONSEJO R4No ratings yet
- Depresión Post-PartoDocument12 pagesDepresión Post-PartoThiara RospigliosiNo ratings yet
- Generalized Anxiety Disorder Obsessive-Compulsive Disorder FinalDocument27 pagesGeneralized Anxiety Disorder Obsessive-Compulsive Disorder Finalapi-608106291No ratings yet
- Body Dissatisfaction and Mental HealthDocument9 pagesBody Dissatisfaction and Mental HealthBammy SiriratNo ratings yet
- Crissman, Stroumsa, Kobernik, & Berger, 2019Document9 pagesCrissman, Stroumsa, Kobernik, & Berger, 2019Anonymous 75M6uB3OwNo ratings yet
- Premenstrual Disorders: Table 1Document7 pagesPremenstrual Disorders: Table 1Ratna AhNo ratings yet
- Interpersonal Trauma and Aging-Related Genitourinary Dysfunction in A National Sample of Older WomenDocument7 pagesInterpersonal Trauma and Aging-Related Genitourinary Dysfunction in A National Sample of Older WomenKarina NathaniaNo ratings yet
- Braverman 2007 PMS and Dysphoric DisorderDocument10 pagesBraverman 2007 PMS and Dysphoric DisorderCarolina GómezNo ratings yet
- 1 s2.0 S0015028211027075 MainDocument8 pages1 s2.0 S0015028211027075 MainHanine El-DekmakNo ratings yet
- Life 13 01268Document13 pagesLife 13 01268tafazzal.eduNo ratings yet
- Premenstrual Syndrome and Premenstrual Sydphoric Disorder, Definitions and Diagnosis.Document13 pagesPremenstrual Syndrome and Premenstrual Sydphoric Disorder, Definitions and Diagnosis.Valeria OrtegaNo ratings yet
- AJGP 0102 2023 Focus Chung Male Sexual Dysfunction WEBDocument5 pagesAJGP 0102 2023 Focus Chung Male Sexual Dysfunction WEBrisang akrima fikriNo ratings yet
- PSST Women Health2013Document8 pagesPSST Women Health2013Andreas NatanNo ratings yet
- Sex Gender DifferencesDocument2 pagesSex Gender DifferencesCamilaNo ratings yet
- Somatoform DisorderDocument14 pagesSomatoform DisorderRifa SalsabiilahNo ratings yet
- Greendale, 2010Document11 pagesGreendale, 2010Carolina EstradaNo ratings yet
- Body Mass Index and Anxiety/depression As Mediators of Theeffects of Child Sexual and Physical Abuse On Physical Healthdisorders in WomenDocument14 pagesBody Mass Index and Anxiety/depression As Mediators of Theeffects of Child Sexual and Physical Abuse On Physical Healthdisorders in WomenBadger6No ratings yet
- Impact of Menopause Symptoms On Women in The WorkplaceDocument13 pagesImpact of Menopause Symptoms On Women in The WorkplaceMarcos Pitta TerraNo ratings yet
- Jurnal GeriatriDocument9 pagesJurnal GeriatriInes DamayantiNo ratings yet
- Manejo Depresion 1Document10 pagesManejo Depresion 1Luis HaroNo ratings yet
- Park, 2019 - NEJM - DepressionDocument10 pagesPark, 2019 - NEJM - DepressionFabian WelchNo ratings yet
- Research PaperDocument10 pagesResearch PaperJan LAWNo ratings yet
- 12 PDFDocument9 pages12 PDFsiscaNo ratings yet
- Nejmp 1311047Document3 pagesNejmp 1311047Sebastian Andres Salazar VidalNo ratings yet
- Fpsyt 12 775762Document17 pagesFpsyt 12 775762Oana OrosNo ratings yet
- Simulation Study To Demonstrate Biases Created by Diagnostic Criteria of Mental Illnesses: Major Depressive Episodes, Dysthymia, and Manic EpisodesDocument27 pagesSimulation Study To Demonstrate Biases Created by Diagnostic Criteria of Mental Illnesses: Major Depressive Episodes, Dysthymia, and Manic EpisodesNovrizal Muhammad fadillahNo ratings yet
- The Measurement of Menstrual Symptoms: Factor Structure of The Menstrual Symptom Questionnaire in Adolescent GirlsDocument16 pagesThe Measurement of Menstrual Symptoms: Factor Structure of The Menstrual Symptom Questionnaire in Adolescent Girlshanna.oravecz1No ratings yet
- Movement Disorders in WomenDocument8 pagesMovement Disorders in WomenInes StrenjaNo ratings yet
- Kuehner 2016Document13 pagesKuehner 2016Claudio Angulo100% (1)
- Effectiveness of Physical Activity Interventions For Improving Depression, Anxiety and DistressDocument10 pagesEffectiveness of Physical Activity Interventions For Improving Depression, Anxiety and DistressDouglas SantosNo ratings yet
- Clinical Significance of A Proposed Developmental Trauma Disorder Diagnosis - Results of An International Survey of Clinicians - 2020 11 09 232956Document14 pagesClinical Significance of A Proposed Developmental Trauma Disorder Diagnosis - Results of An International Survey of Clinicians - 2020 11 09 232956abelim01No ratings yet
- Parkinson's Disease: A Treatment GuideDocument8 pagesParkinson's Disease: A Treatment GuideaimahNo ratings yet
- 1203 FullDocument10 pages1203 FullMeNo ratings yet
- Major Depressive Disorder and Difference Between Genders: Dzevad Sabic, Adela Sabic, Amila Bacic-BecirovicDocument4 pagesMajor Depressive Disorder and Difference Between Genders: Dzevad Sabic, Adela Sabic, Amila Bacic-BecirovicDzevad SabicNo ratings yet
- Assignment - 1 07062023 122711pmDocument5 pagesAssignment - 1 07062023 122711pmaz.rah.e.khudiNo ratings yet
- Social Science & Medicine: ReviewDocument17 pagesSocial Science & Medicine: ReviewNabellaNo ratings yet
- 01 Somatization Disorders in Children and AdolescentsDocument10 pages01 Somatization Disorders in Children and AdolescentsValeria Olarte ManjarresNo ratings yet
- The Prevalence of Women Selected Rural Groups PMDDDocument12 pagesThe Prevalence of Women Selected Rural Groups PMDDRebecaNo ratings yet
- Intl J Gynecology Obste - 2017 - Adelufosi - Cognitive Behavioral Therapy For Post Traumatic Stress Disorder DepressionDocument4 pagesIntl J Gynecology Obste - 2017 - Adelufosi - Cognitive Behavioral Therapy For Post Traumatic Stress Disorder DepressionGibran LeandroNo ratings yet
- Jamapsychiatry Ruscio 2017 Oi 170004Document11 pagesJamapsychiatry Ruscio 2017 Oi 170004Koas aningNo ratings yet
- Currentandexperimental TherapeuticsofinsomniaDocument14 pagesCurrentandexperimental Therapeuticsofinsomniastein godoy pachecoNo ratings yet
- Fragilidad Dolor y EjercicioDocument7 pagesFragilidad Dolor y EjercicioCecilia Suarez HerreraNo ratings yet
- Somatic Symptom and Related Disorders Presentation by Ngwu GinikaDocument35 pagesSomatic Symptom and Related Disorders Presentation by Ngwu Ginikangwuginika3No ratings yet
- Sexuality in Eating Disorders PatientsDocument20 pagesSexuality in Eating Disorders PatientsDuanne MendesNo ratings yet
- Psychiatric and Medical Correlates of DSM-5 Eating Disorders in A Nationally Representative Sample of Adults in The United StatesDocument9 pagesPsychiatric and Medical Correlates of DSM-5 Eating Disorders in A Nationally Representative Sample of Adults in The United StatesManny RosengallegosNo ratings yet
- Somatoform DisordersDocument41 pagesSomatoform DisordersTulika SarkarNo ratings yet
- Association of Psychologic and Nonpsychologic Factors With Primary DysmenorrheaDocument12 pagesAssociation of Psychologic and Nonpsychologic Factors With Primary DysmenorrheaNoviandita PutriNo ratings yet
- Stress - AnxietyDocument4 pagesStress - AnxietyHung Nguyen PhucNo ratings yet
- 507 ArticleDocument7 pages507 ArticleAkansha sharmaNo ratings yet
- Jurnal PsikoDocument11 pagesJurnal PsikoruryNo ratings yet
- Prevalence and Risk Factors For Symptoms of Common MentalDocument7 pagesPrevalence and Risk Factors For Symptoms of Common MentalZakkiyatus ZainiyahNo ratings yet
- Fatimah Sri Ayu Bijak Lestari Assagaf 4Document10 pagesFatimah Sri Ayu Bijak Lestari Assagaf 4Fatimah AssagafNo ratings yet
- Diagnosis of Psychological DisordersDocument1 pageDiagnosis of Psychological Disorderssomya mathurNo ratings yet
- Personality AssessmentDocument1 pagePersonality Assessmentsomya mathurNo ratings yet
- NephronsDocument3 pagesNephronssomya mathurNo ratings yet
- Anatomy of The KidneysDocument1 pageAnatomy of The Kidneyssomya mathurNo ratings yet
- Paper 5Document18 pagesPaper 5somya mathurNo ratings yet
- AttitudesDocument2 pagesAttitudessomya mathurNo ratings yet
- Group CohesionDocument5 pagesGroup Cohesionsomya mathurNo ratings yet
- Organization of PerceptionsDocument1 pageOrganization of Perceptionssomya mathurNo ratings yet
- PrejudiceDocument1 pagePrejudicesomya mathurNo ratings yet
- Procedures For Changing ConsciousnessDocument2 pagesProcedures For Changing Consciousnesssomya mathurNo ratings yet
- Ethical ConsiderationsDocument1 pageEthical Considerationssomya mathurNo ratings yet
- RPA1Document5 pagesRPA1somya mathurNo ratings yet
- Paper-Ii: PsychologyDocument24 pagesPaper-Ii: Psychologysomya mathurNo ratings yet
- Reliability Engineering Old Problems and New ChallengesDocument52 pagesReliability Engineering Old Problems and New Challengessomya mathurNo ratings yet
- 1977EavesEtAl5 26Document22 pages1977EavesEtAl5 26somya mathurNo ratings yet
- 2014 Sawyer How To Transform Schools To Foster CreativityDocument23 pages2014 Sawyer How To Transform Schools To Foster Creativitysomya mathurNo ratings yet
- Case Study 4Document3 pagesCase Study 4somya mathurNo ratings yet
- 33 Chapter THENEURALBASISOFATTENTION2019Document39 pages33 Chapter THENEURALBASISOFATTENTION2019somya mathurNo ratings yet
- EngineeringOurFuture Winter0910Document16 pagesEngineeringOurFuture Winter0910somya mathurNo ratings yet
- Status Scope NOTESDocument4 pagesStatus Scope NOTESsomya mathurNo ratings yet
- Forms of Research Design and (Expost Facto)Document6 pagesForms of Research Design and (Expost Facto)somya mathurNo ratings yet
- Guilford CriticismDocument17 pagesGuilford Criticismsomya mathurNo ratings yet
- Paper 3Document19 pagesPaper 3somya mathurNo ratings yet
- How Do Family Businesses GrowDocument12 pagesHow Do Family Businesses Growsomya mathurNo ratings yet
- Sullivan Neo-FreudianDocument12 pagesSullivan Neo-Freudiansomya mathurNo ratings yet
- Correspondent Inference TheoryDocument11 pagesCorrespondent Inference Theorysomya mathurNo ratings yet
- The Influence of Family Related Factors On Intellectual Capital Performance in Family BusinessesDocument26 pagesThe Influence of Family Related Factors On Intellectual Capital Performance in Family Businessessomya mathurNo ratings yet
- Theoretical Perspectives of Prosocial BehaviourDocument4 pagesTheoretical Perspectives of Prosocial Behavioursomya mathurNo ratings yet
- Unit 2 Role of Agents of SocializationDocument8 pagesUnit 2 Role of Agents of Socializationsomya mathurNo ratings yet
- Intimate Partner ViolenceDocument10 pagesIntimate Partner Violencesomya mathurNo ratings yet
- Giới thiệuDocument10 pagesGiới thiệuSỹ NguyễnNo ratings yet
- Art Therapy Group Intervention For ChildrenDocument10 pagesArt Therapy Group Intervention For ChildrenHarsheen Kaur ChadhaNo ratings yet
- Final CDP DanapurDocument191 pagesFinal CDP DanapurdrpklalNo ratings yet
- ISC Class XII Question Bank For Annual Exam - ENGLISHDocument18 pagesISC Class XII Question Bank For Annual Exam - ENGLISHRishav VermaNo ratings yet
- REPUBLIC ACT NO. 11291 (Magna Carta of The Poor)Document7 pagesREPUBLIC ACT NO. 11291 (Magna Carta of The Poor)Yappi NaniNo ratings yet
- CHCLEG003 HOMEWORK SAMPLE q2Document2 pagesCHCLEG003 HOMEWORK SAMPLE q2chetna sharmaNo ratings yet
- Hypertension & Diabetis MellitusDocument51 pagesHypertension & Diabetis MellitusSuma_Ramesan_5373100% (1)
- Leopold Filter Media ProductsDocument4 pagesLeopold Filter Media ProductsIbrahim Ben AmeurNo ratings yet
- PROTEAN® II Xi Cell IPG Conversion KitDocument2 pagesPROTEAN® II Xi Cell IPG Conversion KitdnajenNo ratings yet
- DABURDocument37 pagesDABURSA AvinashNo ratings yet
- 5070 w08 Ms 4Document4 pages5070 w08 Ms 4mstudy123456No ratings yet
- Earth Science: First Semester - Quarter 2Document28 pagesEarth Science: First Semester - Quarter 2Kurt Adrian AlonzoNo ratings yet
- Secondary GrowthDocument33 pagesSecondary Growthgsr_sasiNo ratings yet
- Technical Guide On IT Migration AuditDocument15 pagesTechnical Guide On IT Migration AudithNo ratings yet
- DCE Biodiesel Information BrochureDocument10 pagesDCE Biodiesel Information BrochureIshwar ChandraNo ratings yet
- Alice in WonderlandDocument13 pagesAlice in WonderlandLuca PresicciNo ratings yet
- First Year Physics Chapter Wise Mcqs PDFDocument49 pagesFirst Year Physics Chapter Wise Mcqs PDFabuzar khanNo ratings yet
- classVIIIenglishGeneral Science-8Document269 pagesclassVIIIenglishGeneral Science-8Tabib GamingNo ratings yet
- Gastritis 180122045533Document16 pagesGastritis 180122045533Manish SapkotaNo ratings yet
- Thalassaemias PDFDocument3 pagesThalassaemias PDFNidia100% (1)
- Contoh Soal TO Inggris Kelas 12Document15 pagesContoh Soal TO Inggris Kelas 12ZefaNo ratings yet
- Risk Benefit AnalysisDocument12 pagesRisk Benefit AnalysisAdinaMilitaruNo ratings yet