Professional Documents
Culture Documents
Jamaneurology Leuzy 2023 Oi 230023 1686342376.28349
Uploaded by
MA MAOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Jamaneurology Leuzy 2023 Oi 230023 1686342376.28349
Uploaded by
MA MACopyright:
Available Formats
Research
JAMA Neurology | Original Investigation
Comparison of Group-Level and Individualized Brain Regions
for Measuring Change in Longitudinal Tau Positron Emission Tomography
in Alzheimer Disease
Antoine Leuzy, PhD; Alexa Pichet Binette, PhD; Jacob W. Vogel, PhD; Gregory Klein, PhD; Edilio Borroni, PhD; Matteo Tonietto, PhD;
Olof Strandberg, PhD; Niklas Mattsson-Carlgren, MD, PhD; Sebastian Palmqvist, MD, PhD; Michael J. Pontecorvo, PhD; Leonardo Iaccarino, PhD;
Erik Stomrud, MD, PhD; Rik Ossenkoppele, PhD; Ruben Smith, MD, PhD; Oskar Hansson, MD, PhD; for the Alzheimer’s Disease Neuroimaging Initiative
Supplemental content
IMPORTANCE Longitudinal tau positron emission tomography (PET) is a relevant outcome
in clinical trials evaluating disease-modifying therapies in Alzheimer disease (AD). A key
unanswered question is whether the use of participant-specific (individualized) regions
of interest (ROIs) is superior to conventional approaches where the same ROI (group-level)
is used for each participant.
OBJECTIVE To compare group- and participant-level ROIs in participants at different stages
of the AD clinical continuum in terms of annual percentage change in tau-PET standardized
uptake value ratio (SUVR) and sample size requirements.
DESIGN, SETTING, AND PARTICIPANTS This was a longitudinal cohort study with consecutive
participant enrollment between September 18, 2017, and November 15, 2021. Included
in the analysis were participants with mild cognitive impairment and AD dementia from
the prospective and longitudinal Swedish Biomarkers For Identifying Neurodegenerative
Disorders Early and Reliably 2 (BioFINDER-2) study; in addition, a validation sample (the AVID
05e, Expedition-3, Alzheimer’s Disease Neuroimaging Initiative [ADNI], and BioFINDER-1
study cohorts) was also included.
EXPOSURES Tau PET (BioFINDER-2, [18F]RO948; validation sample, [18F]flortaucipir),
7 group-level (5 data-driven stages, meta-temporal, whole brain), and 5 individualized ROIs.
MAIN OUTCOMES AND MEASURES Annual percentage change in tau-PET SUVR across ROIs. Sample
size requirements in simulated clinical trials using tau PET as an outcome were also calculated.
RESULTS A total of 215 participants (mean [SD] age, 71.4 (7.5) years; 111 male [51.6%]) from
the BioFINDER-2 study were included in this analysis: 97 amyloid-β (Aβ)–positive cognitively
unimpaired (CU) individuals, 77 with Aβ-positive mild cognitive impairment (MCI), and
41 with AD dementia. In the validation sample were 137 Aβ-positive CU participants, 144 with
Aβ-positive MCI, and 125 with AD dementia. Mean (SD) follow-up time was 1.8 (0.3) years.
Using group-level ROIs, the largest annual percentage increase in tau-PET SUVR in
Aβ-positive CU individuals was seen in a composite ROI combining the entorhinal cortex,
hippocampus, and amygdala (4.29%; 95% CI, 3.42%-5.16%). In individuals with Aβ-positive
MCI, the greatest change was seen in the temporal cortical regions (5.82%; 95% CI,
4.67%-6.97%), whereas in those with AD dementia, the greatest change was seen in the
parietal regions (5.22%; 95% CI, 3.95%-6.49%). Significantly higher estimates of annual
percentage change were found using several of the participant-specific ROIs. Importantly,
the simplest participant-specific approach, where change in tau PET was calculated in Author Affiliations: Author
affiliations are listed at the end of this
an ROI that best matched the participant’s data-driven disease stage, performed best in all article.
3 subgroups. For the power analysis, sample size reductions for the participant-specific ROIs
Group Information: The members
ranged from 15.94% (95% CI, 8.14%-23.74%) to 72.10% (95% CI, 67.10%-77.20%) compared of the Alzheimer’s Disease
with the best-performing group-level ROIs. Findings were replicated using [18F]flortaucipir. Neuroimaging Initiative appear in
Supplement 2.
CONCLUSIONS AND RELEVANCE Finding suggest that certain individualized ROIs carry Corresponding Authors: Antoine
an advantage over group-level ROIs for assessing longitudinal tau changes and increase Leuzy, PhD, Clinical Memory
the power to detect treatment effects in AD clinical trials using longitudinal tau PET as Research Unit, Department of Clinical
Sciences, Lund University, SE-205 02
an outcome.
Malmö, Sweden (antoine.leuzy@
med.lu.se); Oskar Hansson, MD, PhD,
Memory Clinic, Skåne University
JAMA Neurol. 2023;80(6):614-623. doi:10.1001/jamaneurol.2023.1067 Hospital, SE-205 02 Malmö, Sweden
Published online May 8, 2023. (oskar.hansson@med.lu.se).
614 (Reprinted) jamaneurology.com
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease Original Investigation Research
T
he neuropathological hallmarks of Alzheimer disease
(AD) include deposition of extracellular amyloid β (Aβ) Key Points
and intracellular hyperphosphorylated tau. In con-
Question Does defining regions of interest (ROIs) for each
trast to Aβ pathology, which occurs in cortical regions de- participant (individualized) improve the sensitivity to tau
cades before dementia onset, tau pathology is thought to accumulation compared with the use of a conventional approach
emerge in circumscribed regions of the medial temporal lobe where each participant is assigned the same ROI (group-level)?
in early adulthood, before spreading into cortical regions
Findings Significantly higher estimates of annual change in tau
around the time of symptom onset.1 Studies using positron positron emission tomography (PET) were found using several
emission tomography (PET) ligands with high affinity for the of the participant-specific ROIs. Importantly, the simplest
tau aggregates formed in AD have shown that the degree and individualized approach, where change in tau PET was calculated
topography of cortical tau-PET retention overlap strongly with in an ROI that best matched the participant’s data-driven disease
neurodegeneration2 and associate with cognitive decline.2,3 As stage, performed best.
such, tau accumulation is a relevant intervention target and Meaning Individualized ROIs carry an advantage over group-level
potential outcome measure in AD.4 ROIs for assessing longitudinal tau PET and can increase the
The spread of tau in AD has classically been thought to fol- sensitivity to detect treatment effects in AD trials.
low a stereotypical spatiotemporal pattern based on postmor-
tem studies5,6—from the (trans)entorhinal cortex into the hip-
pocampus and inferior temporal lobe, before reaching cortical
association areas (Braak staging scheme). However, autopsy7 and Methods
both cross-sectional8-10 and longitudinal11-15 tau-PET studies have
found substantial interindividual differences in the deposition Participants
and accumulation of tau, with important deviations from the tra- This cohort study received ethical approval from the Regional
ditional Braak model.7-10 Indeed, several distinct subtypes of tau Ethical Committee in Lund, Sweden. Approval for PET imaging
pathology were recently identified using tau PET, with these was obtained from the Swedish Medicines and Products Agency
exhibiting distinct demographic and cognitive profiles, as well and the local Radiation Safety Committee at Skåne University
as differing longitudinal outcomes.16 Although the mechanisms Hospital in Sweden. All participants gave written informed con-
underlying this variability remain, as yet, unclear, they may be sent. We included cognitively unimpaired (CU) individuals, pa-
associated with individual differences in brain organization (eg, tients with mild cognitive impairment (MCI), and those with
variation in axonal connectivity patterns), regional vulnerabil- AD dementia from the prospective and longitudinal Swedish
ity (eg, deposition of tau along different networks), or variation Biomarkers For Identifying Neurodegenerative Disorders Early
in disease biochemistry (eg, individual differences in enzymatic and Reliably 2 (BioFINDER-2) study.21 Participants were enrolled
activity, copathology, or other biological processes).17 between September 18, 2017, and November 15, 2021. Inclusion
Longitudinal tau PET is increasingly used as an outcome and exclusion criteria have been described elsewhere (eMethods
measure to detect either drug target engagement or efficacy in 1 in Supplement 1).22,23 CU individuals were 60 years or older and
AD clinical trials evaluating disease-modifying therapies.18 Re- did not have MCI or dementia.22,23 Exclusion criteria included
cent work comparing tau PET and cognition as outcomes in clini- presence of objective cognitive impairment, severe somatic dis-
cal trials showed that significantly fewer participants were re- ease, and current alcohol/substance misuse. Patients with MCI
quired to detect a meaningful change in the rate of tau accumu- fulfilled the Diagnostic and Statistical Manual of Mental Disorders
lation compared with the rate of cognitive decline.19 However, (Fifth Edition) criteria for mild neurocognitive disorder whereas
interindividual heterogeneity in the pattern of tau spread poses patients with AD dementia fulfilled the DSM-5 criteria for ma-
a challenge to the accurate prediction of tau progression at the jor cognitive impairment due to AD.24 Aβ status was defined using
individual level.11-15 The use of participant-specific (individual- CSFAβ42/Aβ40, as previously described.23 This study followed
ized) approaches for the prediction of future tau spreading may the Strengthening the Reporting of Observational Studies in
help increase the sensitivity to detect treatment effects and help Epidemiology (STROBE) reporting guidelines.
reduce the number of patients included into these trials. Prelimi-
nary findings using one such approach showed that defining re- Image Acquisition and Processing
gions of interest (ROIs) for each participant improved the sen- [18F]RO948 PET was performed on digital scanners (Discovery
sitivity to tau accumulation and significantly reduced required MI [GE Healthcare]) 70 to 90 minutes after injection, as described
sample sizes when compared with the use of conventional (eg, previously.22 As some off-target binding has been described in
Braak stages, temporal and whole-brain meta-ROIs) approaches the meninges for [18F]RO948,22 no smoothing was performed
where each participant is assigned the same (group-level) ROI.20 during image reconstruction. To further reduce the possibility
In the present study, we aimed to expand on work on participant- an off-target signal, a more accurate meningeal segmentation was
specific ROIs by comparing group-level and individualized ROIs obtained using T1/T2 magnetic resonance imaging (with Se-
defined using a range of methods differing in complexity level quence Adaptive Multimodal Segmentation [SAMSEG] FreeSurfer
across several metrics using longitudinal [18F]RO948 tau PET utility [Laboratory for Computational Neuroimaging]),25 which
in participants at different stages of the AD clinical continuum. was then used to prune the adjacent FreeSurfer ROIs (eMethods
The results were validated in an independent data set with lon- 2 in Supplement 1). The corrected ROI set was then used in a geo-
gitudinal [18F]flortaucipir. metric transfer matrix (GTM) partial volume error correction.26
jamaneurology.com (Reprinted) JAMA Neurology June 2023 Volume 80, Number 6 615
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Research Original Investigation Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease
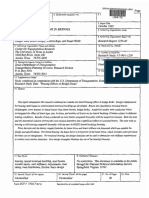
Figure 1. Group-Level Regions of Interest (ROIs)
A Data-driven stages B Meta-ROIs
Stage I Stage II Stage III Stage IV Stage V Temporal Whole brain
C Braak stages
Stage I Stage II Stage III Stage IV Stage V Stage VI
Group-level ROIs include previously published data-driven stages for [18F]RO948 (A), temporal and whole-brain meta-ROIs (B), and Braak stages (C).
Serial high-resolution T1-weighted magnetic resonance images (5) subtype and stage inference (SUSTAIN). In Q1, as described
were acquired (3T MAGNETOM Prisma [Siemens Healthineers]) elsewhere,20 Gaussian-mixture modeling (GMM) was first
for PET image coregistration, template normalization, and seg- performed across all 200 cortical regions of the Schaefer brain
mentation using longitudinal FreeSurfer, version 6.0.27 Standard- atlas34 in order to extract the probability of being tau-PET posi-
ized uptake value ratio (SUVR) images were created using the in- tive for each region. After establishing participant-specific tau-
ferior cerebellar cortex as the reference region. A sensitivity analy- PET epicenters (ie, the top 10% regions with the highest prob-
sis was performed using an alternative reference region consisting ability of having abnormal tau-PET SUVR values), the functional
of the whole cerebellum, brainstem, and eroded subcortical white connectivity-based distance of each the remaining ROIs to the
matter. In keeping with the ROI-based analyses that were cor- epicenter was determined and divided into nonoverlapping
rected for partial volume effects using GTM, voxelwise analyses quartiles based each region’s connectivity to the epicenter.20
were performed using region-based voxelwise correction,28 Q1, representing the top 25% regions with strongest functional
a partial-volume technique that extends the GTM method and connectivity to the epicenter, was used to calculate change in tau-
performs a voxelwise correction of the entire image. PET SUVR. Functional connectivity data was obtained from
69 CU individuals from the ADNI cohort who were Aβ-negative
Tau-PET ROI Definition and had low (global SUVR <1.30) tau-PET binding.35 Distance
Complete details for group-level and individualized ROIs are between epicenter and nonepicenter ROIs was determined by
included in eMethods 3 and eTables 1, 2, and 3 in Supple- converting average participant-specific functional connectivity
ment 1. All approaches were implemented in native space. matrices to a distance-based connectivity matrix, with shorter
Group-level ROIs (Figure 1) included previously described path length between ROIs indicating stronger connectivity.36
stages for [18F]RO948,29 established using a data-driven ap- Using the probability-based approach, the probability of
proach combining clustering and event-based modeling.30,31 being tau-PET positive was extracted for each region from the
This approach identified target ROIs that were broadly con- FreeSurfer atlas using GMM.20 Different probability intervals
sistent with widely used [18F]flortaucipir-derived Braaklike were then selected, with brain regions with probabilities within
imaging stages and covered the full spectrum of AD tau aggre- the selected interval combined into a composite ROI for each
gation, from early to later affected areas. In addition, we in- participant and used to calculated change in tau-PET SUVR.
cluded whole-brain and temporal meta-ROIs.32 A sensitivity The probability interval yielding the highest average change
analysis was performed using Braak ROIs.33 across participants was then selected.
For individualized ROIs (Figure 2), the following 5 approaches Overlap index is a recently proposed method that assesses
were used: (1) quartile 1 (Q1), (2) probability based, (3) overlap in- the stability of voxels above a defined threshold,37 based on the
dex, (4) highest tau-PET–positive data-driven stage (DDS), and assumption that suprathreshold voxels that remain stable over
616 JAMA Neurology June 2023 Volume 80, Number 6 (Reprinted) jamaneurology.com
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease Original Investigation Research
Figure 2. Approaches to Derive Individualized Regions of Interest (ROIs)
A Quartile 1 approach B Probability-based approach
1. Extract probabilities of tau positivity from ROIs 2. Define tau epicenters 1. Extract probabilities of tau positivity from ROIs
GMM applied to ROI-specific tau PET SUVRs ROIs GMM applied to ROI-specific tau PET SUVRs ROIs
2.0 2.0
1.5 Tau negative 1.5 Tau negative
Participants
Density
Density
Tau-positive Tau-positive
Participants
Tau positive probabilities Tau positive probabilities
1.0 1.0
0.5 0.5
0 0
1 2 3 4 5 1 2 3 4 5
SUVR Epicenter (top 10%) SUVR
3. Identify quartile 1 using connectivity-based distance to epicenters 2. Calculate change in SUVR across different
Connectivity-based distance 72-ROI probability intervals
200-ROI brain parcellation
to epicenter 6
brain parcellation 8.18 0.2-0.7 0.2-0.8 0.2-0.9 0.2-1
4
7.42
Longitudinal change in tau PET
Mean tau PET SUVR change per y, %
6.67 Select interval
Q1 0
5.91 with highest
5.16 Aβ+CU Aβ+CU Aβ+CU Aβ+CU
Q2 annual Group
4.4
3.65 percentage
Q3 6
2.89 change in 0.3-0.7 0.3-0.8 0.3-0.9 0.3-1
4
2.14 SUVR
1.38
Q4 2
0.63 0
Connectivity-based distance to epicenter Aβ+CU Aβ+CU Aβ+CU Aβ+CU
Group
6 0.4-0.7 0.4-0.8 0.4-0.9 0.4-1
C Overlap Index approach 4
2
Apply cutoff of 0
Tau PET SUVR
SUVR >1.4 Aβ+CU Aβ+CU Aβ+CU Aβ+CU
Binary masks Group
D Highest tau PET-positive DDS approach
Spatial overlap For each of the 5 DDS ROIs
Tau PET positive
Follow-up Follow-up Apply GMM-based cutoff
Tau PET negative
DDSs
Stage I Stage IV
Select highest DDS that is tau
PET positive and calculate
Stage II Stage V
change in SUVR in that stage
Stage III
Baseline Baseline
A, In the quartile 1 approach, we extracted gaussian mixture modeling intervals. In order to limit the number of intervals, 0.2 to 0.4 (ie, 0.2, 0.3, 0.4)
(GMM)–based probabilities of being tau positive from all brain regions in the and 0.7 to 1 (ie, 0.7, 0.8 0.9, 1) were used as lower and upper start values,
Schaefer brain atlas and defined the top 10% of ROIs as tau epicenters (ie, brain respectively. The interval that resulted in the highest annual percentage change
regions in which tau emerges first). After calculating the connectivity-based in tau-PET SUVR across participants was then selected for use. The approach is
distance of each ROI to the participant-specific epicenters, ROIs were grouped illustrated for amyloid-β (Aβ)–positive cognitively unimpaired (CU) individuals.
into nonoverlapping quartiles on the basis of their connectivity-based distance C, In the overlap index approach, change in tau PET was determined using the
to the epicenter (ie, quartile 1 [Q1] is closest to the epicenter). B, In the mask resulting from the spatial overlap of the baseline and follow-up scans.
probability-based approach, GMM-based probabilities of being tau positive D, In the highest tau-PET–positive data-driven stage (DDS) approach, cutoffs
were first extracted from the FreeSurfer (Laboratory for Computational were applied to baseline SUVR data in group-level data-driven ROIs, with
Neuroimaging) atlas and change in tau–positron emission tomography (PET) change calculated using the highest (ie, latest in the tau progression cascade)
standardized uptake value ratio (SUVR) calculated across different probability ROI that was tau positive.
time represent a true positive signal due to tau pathology and hierarchical pattern in the cortex.29,38,39 We hypothesized that
not random variability. Only cortical gray matter was consid- change in tau-PET SUVRs would be highest in those regions
ered, with a mask extracted from the FreeSurfer segmenta- most recently affected. We therefore applied GMM-based
tion. After obtaining masks for the baseline and follow-up scans cutoffs to baseline SUVR values for each of the 5 DDS ROIs
using an SUVR threshold of greater than 1.40, their spatial over- (designated stages 1-5) (Figure 1) to determine which of these
lap was determined, with the resulting mask then used to cal- ROIs were affected by tau at baseline in each individual. Next,
culate change in tau-PET SUVR. In keeping with the ROI-based we measured longitudinal change in the ROI affected last in
analyses, the analysis was performed in native space. the tau accumulation cascade in each participant (eg, using
The highest tau-PET–positive DDS is based on in vivo tau- the stage 4 ROI in an individual positive in stage ROIs 1, 2, 3,
PET studies showing that tau aggregation in AD follows a and 4) (eTable 4 in Supplement 1).
jamaneurology.com (Reprinted) JAMA Neurology June 2023 Volume 80, Number 6 617
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Research Original Investigation Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease
Table. Characteristics of Participants in the Biomarkers For Identifying Neurodegenerative Disorders Early
and Reliably 2 (BioFINDER-2) Cohort
Amyloid-β positive
AD dementia
Characteristic CU (n = 97) MCI (n = 77) (n = 41)
Age, mean (SD), y 68.89 (9.19) 72.39 (7.68) 72.57 (7.27)
Sex, No. (%)
Male 51 (52.6) 42 (54.5) 18 (43.9)
Female 46 (47.4) 35 (45.5) 23 (56.1) Abbreviations: AD, Alzheimer
Education, mean (SD), y 12.38 (3.57) 13.11 (4.63) 11.70 (4.45) disease; CU, cognitively impaired;
MCI, mild cognitive impairment;
MMSE score, mean (SD) 28.68 (1.45) 26.81 (1.97) 23.39 (1.82)
MMSE, Mini-Mental State
Tau PET, mean (SD) scan 1.83 (0.36) 1.92 (0.53) 1.66 (0.34) Examination; PET, positron
interval, y emission tomography.
SUSTAIN is an unsupervised machine-learning tech- in tau-PET SUVR were significant, 1-sample t tests against 0
nique that identifies population subgroups with common were performed groupwise for each ROI. To determine the ef-
patterns of disease progression.40 Specifically, it first identi- fect of ROI on sample size requirements in theoretical trials
fies subtypes and then reconstructs the trajectory of stages using tau PET as outcome, a power analysis was performed
within each subtype, with a subtype and stage assigned to each groupwise, assuming 20%, 30%, or 40% reductions in the an-
participant. SUSTAIN has recently been used to identify 4 nual percentage change in tau-PET SUVR compared with pla-
tau-PET subtypes in AD using [18F]flortaucipir.16 cebo. Differences between group-level and individualized
The 4-subtype model was applied to probabilistically as- ROIs—for both annual change in SUVR and sample size reduc-
sign individuals to 1 of 30 progressive stages along 1 of 4 sub- tions—were tested using bootstrapping (n = 1000; ie, does the
type trajectories. In order to create an individualized ROI mean of the higher value exceed the 95% CI of the lower value).
for each participant, the FreeSurfer regions included in each All analyses were done with R version, 4.2.1 (R Foundation).
stage were grouped as follows: 1 to 10, 11 to 20, and 21 to 30.
Power and Sensitivity Analysis Comparing Change
Results
in SUVR and Tau Extent
As preliminary data using [18F]GTP-1 has shown greater sen- Participant Characteristics and Change in Tau PET
sitivity to longitudinal change in tau PET using tau extent, de- A total of 215 participants (mean [SD] age, 71.4 (7.5) years;
fined as the number of voxels above a defined threshold 111 male [51.6%]; 104 female [48.4%]) with longitudinal tau
divided by the total number of voxels in that region (ie, the PET were included in this analysis: 97 Aβ-positive CU individu-
percentage of abnormal voxels within a given region), in als (45%), 77 Aβ-positive individuals with MCI (36%), and 41
the temporal meta-ROI,41 we compared sample size reduc- individuals with AD dementia (19%) from the BioFINDER-2
tion using annual percentage change in tau extent and SUVR study. Mean (SD) follow-up time was 1.8 (0.3) years. Partici-
for [18F]RO948 in this region (eMethods 3 in Supplement 1). pant characteristics are summarized in the Table. Group-level
ROIs are shown in Figure 1 whereas the approaches used to de-
Independent Validation Sample rive individualized ROIs are shown in Figure 2 and Figure 3.
Participants (Aβ-positive CU individuals and those with Aβ- A total of 406 participants with longitudinal [18F]flor-
positive MCI and AD dementia) with longitudinal [18F]flortaucipir taucipir tau PET composed the validation sample: 137 Aβ-
tau PET (from the AVID 05e, Expedition-3, ADNI, and Sweden positive CU individuals, 144 with Aβ-positive MCI, and 125 with
BioFINDER-1 cohorts) were included as a validation cohort. In- AD dementia. The validation sample included participants from
clusionandexclusioncriteriaaredescribedelsewhere42;Aβ-status the following study cohorts AVID 05e (n = 151), Expedition-3
was determined using amyloid-PET (AVID 05e and Expedition- (n = 82), ADNI (n = 117), and Sweden BioFINDER-1 (n = 56).
3, [18F]florbetapir; ADNI, [18F]florbetaben or [18F]florbetapir; Usinggroup-levelROIs,thelargestannualpercentageincrease
BioFINDER, [18F]flutemetamol) and neocortical composite in [18F]RO948 SUVR in Aβ-positive CU individuals was seen in DDS
cutoffs (eMethods 4 in Supplement 1). Although the group-level I (entorhinal cortex, hippocampus, and amygdala: 4.29%; 95%
ROIs were the same as those used with [18F]RO948, individual- CI, 3.42%-5.16%; P < .001) (Figure 4A). In Aβ-positive individu-
ized ROIs were redefined using [18F]flortaucipir. als with MCI, the greatest change was seen in DDS II (temporal cor-
tical regions: 5.82%; 95% CI, 4.67%-6.97%; P < .001) (Figure 4A),
Statistical Analyses whereas in individuals with AD dementia, the greatest change was
Annual percentage change in tau-PET SUVR was determined seen in stage III (parietal regions: 7.47%; 95% CI, 6.18%-8.78%;
between baseline and follow-up within ROIs. This was calcu- P < .001) (Figure 4A; eTables 4 and 5 in Supplement 1). Findings
lated as the difference between follow-up and baseline, di- from 1-sample t tests are included in the eTables 4, 5, 6, and 7 in
vided by baseline uptake and divided by the time interval be- Supplement 1. Findings using Braak ROIs were similar to those
tween scans in years. Annual change in SUVR [(follow-up SUVR using DDSs (eTables 6 and 7 in Supplement 1). Across both data-
− baseline SUVR) / change in time] is reported in eTables 4 to driven and Braak ROIs, variation in the number of tau-positive
7 in Supplement 1. In order to test whether the annual changes ROIs decreased across clinical groups (eTable 8 in Supplement 1).
618 JAMA Neurology June 2023 Volume 80, Number 6 (Reprinted) jamaneurology.com
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease Original Investigation Research
Figure 3. Subtype and Stage Inference Regions of Interest
A Limbic-predominant phenotype B MTL-sparing phenotype C Posterior occipitotemporal phenotype D Lateral temporal phenotype
Limbic-predominant stage 5 Limbic-predominant stage 10 Limbic-predominant stage 15 Limbic-predominant stage 20
The 4-tau–positron emission tomography (PET) subtypes are shown. D, Subtype 4, lateral temporal. A representation of different stages (5, 10, 15,
A, Subtype 1, limbic-predominant phenotype. B, Subtype 2, medial temporal 20) for subtype 1 is displayed.
lobe (MTL) sparing. C, Subtype 3, posterior occipitotemporal phenotype.
Estimates of annual change in SUVR were generally numerically sample size reductions for group-level and individualized ROIs
higher using individualized ROIs (Figure 4A). However, signifi- were estimated compared with the temporal meta-ROI due to
cance levels varied by ROI and disease stage (eTable 9 in Supple- its widespread use with tau PET in the AD field and the best-
ment 1). Although all individualized ROIs outperformed group- performing group-level ROI (Figure 4B). In Aβ-positive CU in-
level DDS I in Aβ-positive CU participants (DDS I, 4.29%; 95% dividuals, sample size reductions for the individualized ROIs
CI, 3.42%-5.16%; overlap index, 5.14%; 95% CI, 4.29%-6.13%; ranged from 42.74% (overlap index, 95% CI, 35.44%-49.74%;
SUSTAIN, 5.32%; 95% CI, 4.33%-6.31%; probability, 5.89%; 95% P < .001) to 72.10% (highest tau-PET positive DDS, 95% CI,
CI, 5.23%-6.84%; highest tau-PET–positive DDS, 6.69%; 95% CI, 67.10%-77.20%; P < .001) compared with the temporal meta-
5.66%-7.54%; all P <.001), only the probability and highest tau- ROI and between 12.21% (overlap index, 95% CI, 5.91%-18.51%;
PET–positive DDS approaches resulted in significantly higher es- P = .01) and 56% (highest tau-PET–positive DDS, 95% CI, 51.17%-
timates of annual percentage change in [18F]RO948 SUVR com- 60.10%; P < .001) compared with DDS I (Figure 4B). A similar pat-
paredwiththebest-performinggroup-leveldata-drivenROIacross tern was seen in Aβ-positive MCI sample size reductions be-
Aβ-positive CU individuals and those with MCI (DDS II, 5.82%; tween 15.94% (overlap index, 95% CI, 8.14%-23.74%; P = .001)
95% CI, 4.67%-6.97%; probability, 7.92%; 95% CI, 6.82%-9.02%; and 53.02% (highest tau-PET–positive DDS, 95% CI, 47.10%-
highest tau-PET–positive DDS, 8.67%; 95% CI, 7.49%-9.85%; 59.87%; P < .001) compared with temporal meta-ROI and be-
P <.001) and AD dementia (DDS III, 7.47%; 95% CI, 5.98%- 8.96%; tween 12.22% (overlap index, 95% CI, 4.42%-18.10%; P = .01) and
probability, 9.20%; 95% CI, 7.95%-10.45%; highest tau-PET– 50.38% (highest tau-PET–positive DDS, 95% CI, 45.43%-
positive DDS, 10.74%; 95% CI, 9.33%-11.84%; P <.001). 55.34%; P < .001) compared with DDS II (Figure 4B). In AD de-
Using individualized ROIs, the highest tau-PET–positive mentia, sample size reductions varied between 16.83% (over-
DDS approach performed best across diagnostic groups lap index, 95% CI, 8.78%-25.61%; P = .002) and 48.30% (highest
(Aβ-positive CU, 6.69%; 95% CI, 5.83%- 7.55%; P < .001; Aβ- tau-PET–positive DDS, 95% CI, 41.03%-89.10%; P < .001) com-
positive MCI, 8.67%; 95% CI, 7.49%-9.85%; P < .001; AD de- pared with temporal meta-ROI and between 9.73% (overlap in-
mentia, 10.74%; 95% CI, 9.33%-12.20%; P < .001) (eTable 9 dex, 95% CI, 2.68%-12.41%; P = .004) and 43.59% (highest tau-
in Supplement 1), even when using an alternative reference PET–positive DDS, 95% CI, 38.39%-81.98%; P < .001) compared
region combining the cerebellum, brainstem, and eroded with DDS III (Figure 4B). Only in Aβ-positive CU individuals were
subcortical white matter (eFigure in Supplement 1). significant differences seen between sample size reductions
using the temporal meta-ROI and best-performing DDS (quar-
Power Analysis for Hypothetical Clinical Trials tile 1: temporal meta-ROI, 50.56%; 95% CI, 44.63%-56.50%; DDS
Having compared annual percentage change estimates for I, 22%; 95% CI, 17.10%-26.94%; P <.001; overlap index: tempo-
[18F]RO948 using group-level and individualized ROIs, we es- ral meta-ROI, 42.74%; 95% CI, 35.44%-50.03%; DDS I, 11.65%;
timated sample size requirements for a simulated intervention 95% CI, 5.36%-17.95%; P <.001; SUSTAIN; temporal meta-ROI,
that reduced longitudinal tau accumulation by 30%. For each 47.88%; 95% CI, 38.45%-57.30%; DDS I, 17.76%; 95% CI, 9.34%-
group (ie, Aβ-positive CU, Aβ-positive MCI, and AD dementia), 26.18%; P <.001; probability based: temporal meta-ROI, 64.78%;
jamaneurology.com (Reprinted) JAMA Neurology June 2023 Volume 80, Number 6 619
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Research Original Investigation Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease
Figure 4. Annual Percentage Change in Tau–Positron Emission Tomography (PET) Standardized Uptake Value Ratio (SUVR)
and Sample Size Reductions in a Theoretical Clinical Trial Using Tau-PET as an End Point Using Different Regions of Interest (ROIs)
A Mean percentage change in [18F]RO948 SUVR per y B Mean percentage sample size reductions
Aβ-positive CU individuals Aβ-positive CU individuals
DDS I a
ROI type Quartile 1 DDS I a
DDS II a
Group level
DDS III Temporal
Individualized meta-ROI a
DDS IV Overlap index a
b
DDS V
a
Meta-temporal a
SUSTAIN a
Whole brain a
Quartile 1
a
Overlap index Probability a
a
SUSTAIN
Probability a
Highest tau-positive DDS a
Highest tau-positive DDS a
0 2 4 6 8 10 12 –100 –80 –60 –40 –20 0
Mean tau PET SUVR change per y, % Sample size reduction
Aβ-positive individuals with MCI Aβ-positive individuals with MCI
DDS I a
Quartile 1 DDS II
ROI type a
DDS II
Group level Temporal
DDS III
meta-ROI b
DDS IV Individualized Overlap index
b
DDS V
Meta-temporal a a
SUSTAIN
Whole brain b
Quartile 1
a
Overlap index Probability
a
SUSTAIN
Probability a
Highest tau-positive DDS
Highest tau-positive DDS a
0 2 4 6 8 10 12 –100 –80 –60 –40 –20 0
Mean tau PET SUVR change per y, % Sample size reduction
Individuals with AD dementia Individuals with AD dementia
DDS a
ROI type Quartile 1
DDS II DDS III a
Group level
DDS III Temporal
Individualized meta-ROI b
DDS IV Overlap index
b
DDS V
Meta-temporal a
SUSTAIN
Whole brain b
a
Quartile 1
a
Overlap index Probability
a
SUSTAIN
Probability a
Highest tau-positive DDS
Highest tau-positive DDS a
0 2 4 6 8 10 12 –100 –80 –60 –40 –20 0
Mean tau PET SUVR change per y, % Sample size reduction
A, Mean percentage change in [18F]RO948 SURV per year along with 95% CIs dementia). P values are shown for each bar for comparisons against 0.
for group level and individualized ROIs. P values are shown groupwise for Comparisons in sample reductions between temporal and the best-performing
comparisons between individualized ROIs and the best-performing group-level data-driven stage were only significant in Aβ-positive CU individuals (ie, sample
ROI. B, Mean percentage sample size reductions along with 95% CIs are shown size reductions were significantly greater in Aβ-positive CU individuals using
for group-level and individualized ROIs compared with the temporal meta-ROI data driven stage I, compared with the temporal meta-ROI).
and best-performing data-driven ROIs (ie, data-driven stage I in amyloid β a
P <.001.
(Aβ)–positive cognitively unimpaired [CU]; data-driven stage II in Aβ-positive b
P <.01.
mild cognitive impairment [MCI]; data-driven stage III in Alzheimer disease [AD]
95% CI, 59.67%-69.89%; DDS I, 44.43%; 95% CI, 40.32%- (ie, the number of participants required per arm to detect an
48.54%; P <.001; highest tau-PET–positive DDS: temporal meta- intervention effect) assuming hypothetical intervention ef-
ROI, 72.10%; 95% CI, 66.60%-77.50%; DDS I, 55.90%; 95% CI, fects of 20%, 30%, and 40% are included in eTables 10, 11,
51.45%-60.35%; P <.001) (Figure 4B). Sample size estimations and 12 in the Supplement.
620 JAMA Neurology June 2023 Volume 80, Number 6 (Reprinted) jamaneurology.com
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease Original Investigation Research
Power and Sensitivity Analysis Comparing SUVR progression.5,47,48 The greater sensitivity of individualized
and Tau Extent assessment of tau accumulation over spatially predefined ROIs
When performing a sensitivity analysis comparing annual per- (eg, data-driven or Braak ROIs) across groups, however, suggests
centage change in tau extent and [18F]RO948 SUVR in the tem- the view that tau deposition can be heterogeneous in AD.7-10
poral meta-ROI in a simulated intervention that reduced Variation in the number of tau-PET–positive data-driven or Braak
longitudinal tau accumulation by 30%, sample sizes were ROIs showed that the regional heterogeneity of tau accumula-
consistently lower for SUVR (Aβ-positive CU, 17.90%; 95% tion decreased with disease progression. This observation, com-
CI, 11.47%-24.33%; P = .007; Aβ-positive MCI, 29.47%; 95% CI, bined with the fact that the differences in sample size reductions
19.55%-39.39%; P = .003; AD dementia, 33.94%; 95% between individualized and groupwise ROIs were only signifi-
CI, 25.02%-42.86%; P < .001) (eTable 13 in Supplement 1). cant in Aβ-positive CU individuals, suggests that the utility of in-
dividualized ROIs may be greatest at the preclinical stage of AD.
Independent Validation Sample Heterogeneity in tau deposition may be associated with varying
Among the 406 participants (137 Aβ-positive CU, 144 Aβ-positive tau starting sites (ie, epicenters) and the subsequent spread of
MCI, and 41 AD dementia) with longitudinal [18F]flortaucipir tau tau via connections between brain regions. Previous work using
PET, the mean (SD) age was 77.18 (7.74) years, and 41 were female [18F]flortaucipir found that tau accumulation rates were high-
(48.32%) (eTable 14 in Supplement 1). Similar to findings in est in brain regions with the closest connectivity-based proxim-
BioFINDER-2, the largest annual increase in [18F]flortaucipir SUVR ity to tau epicenters (ie, Q1)20; here, we reproduced these find-
was seen in stage I (3.88%; 95% CI, 3.17%-4.58%) in Aβ-positive ings and extended them through our comparison with DDSs.
CU individuals, with Aβ-positive individuals with MCI and AD de- A similar explanation may also apply to the SUSTAIN-based
mentia showing the largest increases in stages II (5.41%; 95% CI, subtypes in that the distinct tau-PET patterns seen across the
4.51%-6.31%) and III (6.08%; 95% CI, 4.90%-7.26%), respectively 4 different subtypes resembled macroscale neuronal networks
(eTables 15, 16, 17, and 18 in Supplement 1). Further, individual- seeded from different regions within the temporal lobe.16
ized ROIs resulted in significantly higher estimates of annual On the basis of earlier work showing that tau pathology may pla-
percentage change compared with group-level ROIs, with the teau or decrease with more advanced disease stage,49 contrib-
highest tau-PET–positive DDS approach performed best across uting to interindividual variation in longitudinal change, the
diagnostic groups (eTables 15 and 16 in Supplement 1). Similar probability-based approach was an attempt to exclude both
to [18F]RO948, sample size reductions were greater using indi- low-probability regions unlikely to show tau accumulation and
vidualized ROIs compared with group-level ROIs, with highest high-probability regions thought to be at or approaching their
tau-PET–positive DDS performing best (eTables 19, 20, and 21 maximum possible concentrations of tau.49,50
in Supplement 1). Consistent with the hierarchical aggregation characteristic
of the Braak staging system for tau,5,47,48 we found that tau ac-
cumulation was greatest using the highest DDS showing abnor-
mal [18F]RO948 SUVR levels (highest tau-PET–positive DDS).
Discussion Though tau-PET positivity and pathological tau accumulation
In this cohort study, we compared 2 approaches to defining ROIs were also seen in the stages preceding the highest abnormal stage,
for use with longitudinal tau PET: a group-level approach, where suggesting that although there is an increasing burden of tau
the same ROI was used for each participant, and an individual- across the brain—as opposed to the spread of tau from one unin-
ized approach where each participant received their own specific volved area to the next—the accumulation of tau aggregates was
ROI. Our main finding suggests that individualized ROIs increased greatest in the most recently affected brain region. In the context
the sensitivity to detect longitudinal tau accumulation as well of clinical trials using tau PET as outcome, this approach would
as intervention effects in simulated clinical trials using tau PET be comparatively straightforward to implement. Using the base-
as outcome. The added value of the individualized ROIs—in terms linetau-PETscan,prespecifiedtracer-specificcutoffsderivedfrom
of sensitivity to change in tau-PET signal over time and required a large academic cohort could be applied to either data-driven or
sample size—was greater in the Aβ-positive CU group, compared Braak ROIs, with the highest tau-PET–positive ROI then selected
with the Aβ-positive MCI and AD dementia groups. Importantly, for longitudinal use. However, further studies are required to as-
among the methods used to generate the individualized ROIs, the sess the reproducibility of the thresholds for tau positivity pre-
simplest approach (highest tau-PET–positive DDS, where change sented here. In addition to its simplicity, the fact that the high-
in tau PET was calculated in the highest tau-PET–positive DDS) est tau-PET–positive DDS approach was the best-performing ROI
performed best, providing the highest tau-PET change estimates across groups suggests that it could be used in trials across the AD
and sample size reductions. continuum. Although cognitive decline is typically considered as
Findings using group-level data-driven and PET-based Braak a primary outcome measure for clinical trials,51 recent work has
ROIs were consistent with previous longitudinal tau-PET stud- highlighted the potential role of tau PET in clinical trials.19,29 This
ies in that tau accumulation was primarily seen in the medial is further evidenced by antitau drugs entering the clinical trial
temporal lobe early in the disease process (ie, DDS I and Braak pipeline.52 Although further comparative studies are required,
I/II in Aβ-positive CU individuals) and primarily in temporal due to large within- and between-patient variability in frequently
and parietal cortical regions (ie, DDSs II/III and Braak III/IV) used cognitive measures,53 tau PET may allow for AD trials of
in Aβ-positive individuals with cognitive impairment,13,38,43-46 shorter duration and with fewer participants. Lastly, comparison
consistent with the hierarchical Braak staging model of tau of sample size reductions between annual percentage change
jamaneurology.com (Reprinted) JAMA Neurology June 2023 Volume 80, Number 6 621
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Research Original Investigation Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease
in tau extent and SUVR in the temporal meta-ROI suggests that mate within-participant measurement error because partici-
SUVR may be the preferred metric for longitudinal tau PET. pants only had 2 tau-PET scans. This study contributes to the
continuing investigation of optimized trial outcomes and
Strengths and Limitations precision medicine.54
Strengths of this study include that we compared several group-
level and individualized approaches to defining ROIs, with the
methods used for individualized ROIs varying in their level
of complexity. Further, our study covered the clinical con-
Conclusions
tinuum of AD and had a comparatively long follow-up inter- Findings of this cohort study suggest that individualized ROIs
val that was similar across groups. Importantly, we replicated carried an advantage over group-level ROIs for assessing lon-
our main findings with [18F]RO948 using longitudinal [18F]flor- gitudinal tau changes and may increase the sensitivity to de-
taucipir PET in an independent cohort. Limitations include the tect treatment effects in AD clinical trials using longitudinal
modest number of participants scanned with [18F]RO948 in the tau-PET as an outcome. Future studies should assess addi-
AD dementia group and the fact that we could not esti- tional methods for defining individualized ROIs.
ARTICLE INFORMATION Conflict of Interest Disclosures: Dr Leuzy reported Data Sharing Statement: See Supplement 3.
Accepted for Publication: February 15, 2023. receiving consultant fees from Enigma Biomedical Additional Information: Data used in preparation
USA outside the submitted work. Drs Klein, Borroni, of this article were obtained from the Alzheimer’s
Published Online: May 8, 2023. and Tonietto reported being full-time employees of
doi:10.1001/jamaneurol.2023.1067 Disease Neuroimaging Initiative (ADNI) database
F. Hoffmann-La Roche during the conduct of the (http://adni.loni.usc.edu/).
Open Access: This is an open access article study. Dr Palmqvist reported serving on scientific
distributed under the terms of the CC-BY License. advisory boards and/or given lectures in symposia REFERENCES
© 2023 Leuzy A et al. JAMA Neurology. sponsored by BioArctic, Biogen, Cytox, Eli Lilly,
Geras Solutions, and Roche. Drs Pontecorvo and 1. Hansson O. Biomarkers for neurodegenerative
Author Affiliations: Clinical Memory Research diseases. Nat Med. 2021;27(6):954-963.
Unit, Department of Clinical Sciences, Lund Iaccarino reported being full-time employees and
doi:10.1038/s41591-021-01382-x
University, Malmö, Sweden (Leuzy, Binette, shareholders of Eli Lilly and Company. Dr Hansson
reported receiving nonfinancial support (precursor 2. Strikwerda-Brown C, Hobbs DA, Gonneaud J,
Strandberg, Mattsson-Carlgren, Palmqvist, et al; PREVENT-AD, HABS, and AIBL Research
Stomrud, Ossenkoppele, Smith, Hansson); Penn/ of RO948 and AVID PET images) from AVID/Eli Lilly
during the conduct of the study and consultant/ Groups. Association of elevated amyloid and
CHOP Lifespan Brain Institute, University of tau positron emission tomography signal with
Pennsylvania, Philadelphia (Vogel); Department of speaker fees from AC Immune, Amylyx, Alzpath,
near-term development of Alzheimer disease
Psychiatry, University of Pennsylvania, Philadelphia ADx, AVID Radiopharmaceuticals, Biogen, Cerveau,
symptoms in older adults without cognitive
(Vogel); F. Hoffmann-La Roche Ltd, Basel, Eli Lilly, Eisai, Fujirebio, Genentech, Novartis,
impairment. JAMA Neurol. 2022;79(10):975-985.
Switzerland (Klein, Borroni, Tonietto); Department BioArctic, GE Healthcare, Pfizer, Roche, and
doi:10.1001/jamaneurol.2022.2379
of Neurology, Skåne University Hospital, Lund, Siemens outside the submitted work. No other
disclosures were reported. 3. Ossenkoppele R, Smith R, Mattsson-Carlgren N,
Sweden (Mattsson-Carlgren, Smith); Wallenberg et al. Accuracy of tau positron emission
Centre for Molecular Medicine, Lund University, Funding/Support: This work was supported in part tomography as a prognostic marker in preclinical
Lund, Sweden (Mattsson-Carlgren); Memory Clinic, by grants 2016-00906 and 2018-02052 from and prodromal Alzheimer disease: a head-to-head
Skåne University Hospital, Lund, Sweden the Swedish Research Council, grant 2017-0383 comparison against amyloid positron emission
(Palmqvist, Stomrud, Hansson); Avid from the Knut and Alice Wallenberg Foundation, tomography and magnetic resonance imaging.
Radiopharmaceuticals, Philadelphia, Pennsylvania grant 2015.0125 from the Marianne and Marcus JAMA Neurol. 2021;78(8):961-971. doi:10.1001/
(Pontecorvo, Iaccarino); Eli Lilly and Company, Wallenberg Foundation, the Strategic Research jamaneurol.2021.1858
Indianapolis, Indiana (Pontecorvo, Iaccarino); Area MultiPark (Multidisciplinary Research in 4. Gauthier S, Boxer A, Knopman D, et al.
Alzheimer Center Amsterdam, Neurology, Parkinson’s disease) at Lund University, grant Therapeutic targets for Alzheimer disease: amyloid
Vrije Universiteit Amsterdam, Amsterdam UMC AF-939932 from the Swedish Alzheimer vs nonamyloid—where does consensus lie today:
location VUmc, Amsterdam, the Netherlands Foundation, grants FO2019-0326 and a CTAD task force report. J Prev Alzheimers Dis.
(Ossenkoppele); Amsterdam Neuroscience, FO2022-0204 from the Swedish Brain Foundation, 2022;9(2):231-235. doi:10.14283/jpad.2022.29
Neurodegeneration, Amsterdam, the Netherlands grant 1280/20 from the Parkinson Foundation of 5. Braak H, Braak E. Neuropathological staging of
(Ossenkoppele). Sweden, grant 2020-O000028 from the Skåne Alzheimer-related changes. Acta Neuropathol. 1991;
Author Contributions: Drs Leuzy and Hansson had University Hospital Foundation, grants 2020-0314 82(4):239-259. doi:10.1007/BF00308809
full access to all of the data in the study and take and 2020-0383 from Regionalt Forskningsstöd,
6. Kaufman SK, Del Tredici K, Thomas TL, Braak H,
responsibility for the integrity of the data and the grants 2018-Projekt0279 and 2018-Projekt0226
Diamond MI. Tau seeding activity begins in the
accuracy of the data analysis. from the Swedish federal government from the transentorhinal/entorhinal regions and anticipates
Concept and design: Leuzy, Vogel, Klein, Borroni, Swedish federal government, and grant 949570 phospho-tau pathology in Alzheimer disease and
Ossenkoppele, Hansson. from the European Research Council under the PART. Acta Neuropathol. 2018;136(1):57-67.
Acquisition, analysis, or interpretation of data: European Union’s Horizon 2020 research and doi:10.1007/s00401-018-1855-6
Leuzy, Pichet Binette, Vogel, Klein, Tonieto, innovation program. The precursor of
18 7. Murray ME, Graff-Radford NR, Ross OA,
Strandberg, Mattsson-Carlgren, Palmqvist, F-flutemetamol was sponsored by GE Healthcare.
Petersen RC, Duara R, Dickson DW.
Pontecorvo, Iaccarino, Stomrud, Smith, Hansson. The precursor of 18F-RO948 was provided by Neuropathologically defined subtypes of Alzheimer
Drafting of the manuscript: Leuzy. Roche. The precursor of 18F-flortaucipir was disease with distinct clinical characteristics:
Critical revision of the manuscript for important provided by AVID Radiopharmaceuticals. a retrospective study. Lancet Neurol. 2011;10(9):
intellectual content: All authors. Role of the Funder/Sponsor: The funding source 785-796. doi:10.1016/S1474-4422(11)70156-9
Statistical analysis: Leuzy, Vogel, Strandberg, ADNI contributed to the design and implementation 8. Day GS, Gordon BA, Jackson K, et al. Tau-PET
Mattsson-Carlgren. of ADNI and/or provided data but did not participate binding distinguishes patients with early-stage
Obtained funding: Mattsson-Carlgren, Palmqvist, in study analysis or interpretation of data, or in the posterior cortical atrophy from amnestic Alzheimer
Ossenkoppele, Smith, Hansson. writing, review, or approval of the manuscript. disease dementia. Alzheimer Dis Assoc Disord. 2017;
Administrative, technical, or material support: Klein, 31(2):87-93. doi:10.1097/WAD.
Group Information: Members of the Alzheimer’s
Borroni, Strandberg, Palmqvist, Smith, Hansson. 0000000000000196
Disease Neuroimaging Initiative appear in
Supervision: Klein, Tonieto, Ossenkoppele, Hansson. Supplement 2.
622 JAMA Neurology June 2023 Volume 80, Number 6 (Reprinted) jamaneurology.com
Downloaded From: https://jamanetwork.com/ on 09/04/2023
Brain Regions for Measuring Change in Longitudinal Tau PET in Alzheimer Disease Original Investigation Research
9. Ossenkoppele R, Schonhaut DR, Schöll M, et al. 24. American Psychiatric Association; DSM-5 Task Neuroimaging Initiative (ADNI). Uncovering the
Tau PET patterns mirror clinical and neuroanatomical Force. Diagnostic and Statistical Manual of Mental heterogeneity and temporal complexity of
variability in Alzheimer disease. Brain. 2016;139(Pt 5): Disorders: DSM-5. 5th ed. American Psychiatric neurodegenerative diseases with subtype and
1551-1567. doi:10.1093/brain/aww027 Publishing; 2013. stage inference. Nat Commun. 2018;9(1):4273.
10. Ossenkoppele R, Lyoo CH, Sudre CH, et al. 25. Puonti O, Iglesias JE, Van Leemput K. Fast and doi:10.1038/s41467-018-05892-0
Distinct tau PET patterns in atrophy-defined sequence-adaptive whole-brain segmentation using 41. Sanabria Bohórquez S, Marik J, Ogasawara A,
subtypes of Alzheimer disease. Alzheimers Dement. parametric bayesian modeling. Neuroimage. 2016; et al. [18F]GTP1 (Genentech Tau Probe 1),
2020;16(2):335-344. doi:10.1016/j.jalz.2019.08.201 143:235-249. doi:10.1016/j.neuroimage.2016.09.011 a radioligand for detecting neurofibrillary tangle
11. Chiotis K, Saint-Aubert L, Rodriguez-Vieitez E, 26. Rousset OG, Ma Y, Evans AC. Correction for tau pathology in Alzheimer disease. Eur J Nucl Med
et al. Longitudinal changes of tau PET imaging in partial volume effects in PET: principle and Mol Imaging. 2019;46(10):2077-2089.
relation to hypometabolism in prodromal and validation. J Nucl Med. 1998;39(5):904-911. doi:10.1007/s00259-019-04399-0
Alzheimer disease dementia. Mol Psychiatry. 2018; 27. Reuter M, Schmansky NJ, Rosas HD, Fischl B. 42. Smith R, Strandberg O, Mattsson-Carlgren N,
23(7):1666-1673. doi:10.1038/mp.2017.108 Within-subject template estimation for unbiased et al. The accumulation rate of tau aggregates is
12. Sintini I, Graff-Radford J, Senjem ML, et al. longitudinal image analysis. Neuroimage. 2012;61 higher in females and younger amyloid-positive
Longitudinal neuroimaging biomarkers differ across (4):1402-1418. doi:10.1016/j.neuroimage.2012. subjects. Brain. 2020;143(12):3805-3815.
Alzheimer disease phenotypes. Brain. 2020;143(7): 02.084 doi:10.1093/brain/awaa327
2281-2294. doi:10.1093/brain/awaa155 28. Thomas BA, Erlandsson K, Modat M, et al. 43. Johnson KA, Schultz A, Betensky RA, et al.
13. Jack CR Jr, Wiste HJ, Schwarz CG, et al. The importance of appropriate partial volume Tau positron emission tomographic imaging in
Longitudinal tau PET in aging and Alzheimer correction for PET quantification in Alzheimer aging and early Alzheimer disease. Ann Neurol.
disease. Brain. 2018;141(5):1517-1528. doi:10.1093/ disease. Eur J Nucl Med Mol Imaging. 2011;38(6): 2016;79(1):110-119. doi:10.1002/ana.24546
brain/awy059 1104-1119. doi:10.1007/s00259-011-1745-9 44. Pontecorvo MJ, Devous MD Sr, Navitsky M,
14. Pontecorvo MJ, Devous MD, Kennedy I, et al. 29. Leuzy A, Smith R, Cullen NC, et al. et al; 18F-AV-1451-A05 investigators. Relationships
A multicentre longitudinal study of flortaucipir (18F) Biomarker-based prediction of longitudinal tau between flortaucipir PET tau binding and amyloid
in normal aging, mild cognitive impairment and positron emission tomography in Alzheimer burden, clinical diagnosis, age, and cognition. Brain.
Alzheimer disease dementia. Brain. 2019;142(6): disease. JAMA Neurol. 2022;79(2):149-158. 2017;140(3):748-763. doi:10.1093/brain/aww334
1723-1735. doi:10.1093/brain/awz090 doi:10.1001/jamaneurol.2021.4654 45. Sanchez JS, Becker JA, Jacobs HIL, et al. The
15. Harrison TM, La Joie R, Maass A, et al. 30. Young AL, Oxtoby NP, Daga P, et al; Alzheimer’s cortical origin and initial spread of medial temporal
Longitudinal tau accumulation and atrophy in aging Disease Neuroimaging Initiative. A data-driven tauopathy in Alzheimer disease assessed with
and Alzheimer disease. Ann Neurol. 2019;85(2): model of biomarker changes in sporadic Alzheimer positron emission tomography. Sci Transl Med. 2021;
229-240. doi:10.1002/ana.25406 disease. Brain. 2014;137(Pt 9):2564-2577. 13(577):eabc0655. doi:10.1126/scitranslmed.abc0655
16. Vogel JW, Young AL, Oxtoby NP, et al; doi:10.1093/brain/awu176 46. Lowe VJ, Wiste HJ, Senjem ML, et al.
Alzheimer’s Disease Neuroimaging Initiative. Four 31. Hilger K, Fukushima M, Sporns O, Fiebach CJ. Widespread brain tau and its association with
distinct trajectories of tau deposition identified in Temporal stability of functional brain modules ageing, Braak stage and Alzheimer dementia. Brain.
Alzheimer disease. Nat Med. 2021;27(5):871-881. associated with human intelligence. Hum Brain Mapp. 2018;141(1):271-287. doi:10.1093/brain/awx320
doi:10.1038/s41591-021-01309-6 2020;41(2):362-372. doi:10.1002/hbm.24807 47. Braak H, Alafuzoff I, Arzberger T,
17. Vogel JW, Hansson O. Subtypes of Alzheimer 32. Jack CR Jr, Wiste HJ, Weigand SD, et al. Kretzschmar H, Del Tredici K. Staging of Alzheimer
disease: questions, controversy, and meaning. Defining imaging biomarker cut points for brain disease-associated neurofibrillary pathology using
Trends Neurosci. 2022;45(5):342-345. doi:10.1016/j. aging and Alzheimer disease. Alzheimers Dement. paraffin sections and immunocytochemistry. Acta
tins.2022.02.001 2017;13(3):205-216. doi:10.1016/j.jalz.2016.08.005 Neuropathol. 2006;112(4):389-404. doi:10.1007/
s00401-006-0127-z
18. Shcherbinin S, Evans CD, Lu M, et al. 33. Cho H, Choi JY, Hwang MS, et al. In vivo
Association of amyloid reduction after donanemab cortical spreading pattern of tau and amyloid in the 48. Braak H, Braak E. Staging of Alzheimer’s
treatment with tau pathology and clinical Alzheimer disease spectrum. Ann Neurol. 2016;80 disease-related neurofibrillary changes. Neurobiol
outcomes: the TRAILBLAZER-ALZ randomized (2):247-258. doi:10.1002/ana.24711 Aging. 1995;16(3):271-278. doi:10.1016/0197-4580
clinical trial. JAMA Neurol. 2022;79(10):1015-1024. (95)00021-6
34. Schaefer A, Kong R, Gordon EM, et al.
doi:10.1001/jamaneurol.2022.2793 Local-global parcellation of the human cerebral 49. Phillips JS, Nitchie FJ IV, Da Re F, et al;
19. Giorgio J, Jagust WJ, Baker S, Landau SM, cortex from intrinsic functional connectivity MRI. Alzheimer’s Disease Neuroimaging Initiative. Rates
Tino P, Kourtzi Z; Alzheimer’s Disease Cereb Cortex. 2018;28(9):3095-3114. of longitudinal change in 18 F-flortaucipir PET vary
Neuroimaging Initiative. A robust and interpretable doi:10.1093/cercor/bhx179 by brain region, cognitive impairment, and age in
machine learning approach using multimodal atypical Alzheimer disease. Alzheimers Dement.
35. Franzmeier N, Neitzel J, Rubinski A, et al; 2022;18(6):1235-1247. doi:10.1002/alz.12456
biological data to predict future pathological tau Alzheimer’s Disease Neuroimaging Initiative
accumulation. Nat Commun. 2022;13(1):1887. (ADNI). Functional brain architecture is associated 50. Whittington A, Gunn RN; Alzheimer’s Disease
doi:10.1038/s41467-022-28795-7 with the rate of tau accumulation in Alzheimer Neuroimaging Initiative. TauIQ: a canonical
20. Franzmeier N, Dewenter A, Frontzkowski L, disease. Nat Commun. 2020;11(1):347. image-based algorithm to quantify tau PET scans.
et al. Patient-centered connectivity-based doi:10.1038/s41467-019-14159-1 J Nucl Med. 2021;62(9):1292-1300. doi:10.2967/
prediction of tau pathology spread in Alzheimer jnumed.120.258962
36. Rubinov M, Sporns O. Complex network
disease. Sci Adv. 2020;6(48):eabd1327. doi:10.1126/ measures of brain connectivity: uses and 51. Sperling RA, Rentz DM, Johnson KA, et al.
sciadv.abd1327 interpretations. Neuroimage. 2010;52(3):1059-1069. The A4 study: stopping AD before symptoms
21. The Swedish BioFINDER 2 Study (BioFINDER 2). doi:10.1016/j.neuroimage.2009.10.003 begin? Sci Transl Med. 2014;6(228):228fs13.
ClinicalTrials.gov identifier: NCT03174938. Updated doi:10.1126/scitranslmed.3007941
37. Lee J, Burkett BJ, Min HK, et al. The overlap
March 2, 2021. Accessed September 10, 2022. index as a means of evaluating early tau PET signal 52. Cummings J, Blennow K, Johnson K, et al.
https://clinicaltrials.gov/ct2/show/NCT03174938 reliability. J Nucl Med. 2022;63(11):1748-1753. Antitau trials for Alzheimer disease: a report from
22. Leuzy A, Smith R, Ossenkoppele R, et al. doi:10.2967/jnumed.121.263136 the EU/US/CTAD task force. J Prev Alzheimers Dis.
Diagnostic performance of RO948 F 18 tau positron 2019;6(3):157-163. doi:10.14283/jpad.2019.14
38. Pascoal TA, Benedet AL, Tudorascu DL, et al.
emission tomography in the differentiation of Longitudinal 18F-MK-6240 tau tangles 53. Sabbagh MN, Hendrix S, Harrison JE.
Alzheimer disease from other neurodegenerative accumulation follows Braak stages. Brain. 2021;144 FDA position statement “Early Alzheimer disease:
disorders. JAMA Neurol. 2020;77(8):955-965. (11):3517-3528. doi:10.1093/brain/awab248 developing drugs for treatment, guidance for
doi:10.1001/jamaneurol.2020.0989 industry”. Alzheimers Dement (N Y). 2019;5:13-19.
39. Therriault J, Pascoal TA, Firoza LZ, et al. doi:10.1016/j.trci.2018.11.004
23. Palmqvist S, Janelidze S, Quiroz YT, et al. Biomarker modeling of Alzheimer disease using
Discriminative accuracy of plasma phospho-tau217 PET-based Braak staging. Nat Aging. 2022;2:525-535. 54. Coughlan G, Coutrot A, Khondoker M,
for Alzheimer disease vs other neurodegenerative doi:10.1038/s43587-022-00204-0 Minihane AM, Spiers H, Hornberger M. Toward
disorders. JAMA. 2020;324(8):772-781. personalized cognitive diagnostics of at-genetic-risk
doi:10.1001/jama.2020.12134 40. Young AL, Marinescu RV, Oxtoby NP, et al; Alzheimer disease. Proc Natl Acad Sci U S A. 2019;
Genetic FTD Initiative (GENFI); Alzheimer’s Disease 116(19):9285-9292. doi:10.1073/pnas.1901600116
jamaneurology.com (Reprinted) JAMA Neurology June 2023 Volume 80, Number 6 623
Downloaded From: https://jamanetwork.com/ on 09/04/2023
You might also like
- Dodge Symposium MCI 2014 V7 LatestDocument34 pagesDodge Symposium MCI 2014 V7 LatestWorldEventsForumNo ratings yet
- Dodge - Symposium MCI 2014 V5Document33 pagesDodge - Symposium MCI 2014 V5WorldEventsForumNo ratings yet
- TMP 768 BDocument8 pagesTMP 768 BFrontiersNo ratings yet
- Predicting Opioid Overdose Risk of PatientsDocument8 pagesPredicting Opioid Overdose Risk of PatientsSabin TabircaNo ratings yet
- A Meta-Analysis On Progressive Atrophy in Intractable Temporal Lobe EpilepsyDocument12 pagesA Meta-Analysis On Progressive Atrophy in Intractable Temporal Lobe EpilepsyBeny RiliantoNo ratings yet
- Caveats of Longitudinal Automated Hippocampal Volumetry in Alzheimer's DiseaseDocument22 pagesCaveats of Longitudinal Automated Hippocampal Volumetry in Alzheimer's Diseasedess101No ratings yet
- Biomarker Progressions Explain Higher Variability in Stage S - 2014 - AlzheimerDocument14 pagesBiomarker Progressions Explain Higher Variability in Stage S - 2014 - AlzheimerPriscilla ChantalNo ratings yet
- Piis0007091217349061 2Document6 pagesPiis0007091217349061 2Ana Belén Artero CastañoNo ratings yet
- Changes in Plasma Amyloid and Tau in ADocument16 pagesChanges in Plasma Amyloid and Tau in AeastareaNo ratings yet
- REvisión sistemática 2023Document38 pagesREvisión sistemática 2023juanpaNo ratings yet
- Machine Learning Did Not Beat Logistic Regression in Time Series Prediction For Severe Asthma ExacerbationsDocument8 pagesMachine Learning Did Not Beat Logistic Regression in Time Series Prediction For Severe Asthma ExacerbationsfabianoferrariNo ratings yet
- Alzheimer 'S Disease Profiled by Uid and Imaging Markers: Tau PET Best Predicts Cognitive DeclineDocument11 pagesAlzheimer 'S Disease Profiled by Uid and Imaging Markers: Tau PET Best Predicts Cognitive DeclineChouaib OujhainNo ratings yet
- Fnins 14 558532Document16 pagesFnins 14 558532anita putri effendiNo ratings yet
- A New Age-Related Cutoff of Medial Temporal Atrophy Scale On MRI Improving The Diagnostic Accuracy of Neurodegeneration Due To Alzheimer's Disease in A Chinese PopulationDocument8 pagesA New Age-Related Cutoff of Medial Temporal Atrophy Scale On MRI Improving The Diagnostic Accuracy of Neurodegeneration Due To Alzheimer's Disease in A Chinese PopulationMuhammad Naqvi Al FarisiNo ratings yet
- Type 2 Diabetes, Skin Auto Uorescence, and Brain AtrophyDocument7 pagesType 2 Diabetes, Skin Auto Uorescence, and Brain AtrophyTeky WidyariniNo ratings yet
- HarP The EADC ADNI Harmonized Protocol For Manual Hippocampal Segmentation. A Standard of Reference From A Global Working GroupnnDocument13 pagesHarP The EADC ADNI Harmonized Protocol For Manual Hippocampal Segmentation. A Standard of Reference From A Global Working GroupnnValeria AlzateNo ratings yet
- Jsaa 086Document11 pagesJsaa 086Elías Coreas SotoNo ratings yet
- ADNIannualchangebiomarkers clinicaloutcomeA&D10Document8 pagesADNIannualchangebiomarkers clinicaloutcomeA&D10brunoabramoffNo ratings yet
- Clinical Features, Diagnosis, and Survival Analysis of Dogs With GliomaDocument16 pagesClinical Features, Diagnosis, and Survival Analysis of Dogs With GliomaEquilibrium EduardoNo ratings yet
- Proximity To Dementia Onset and Multimodal Neuroimaging ChangesDocument12 pagesProximity To Dementia Onset and Multimodal Neuroimaging ChangesaffanbasmalahNo ratings yet
- Tau PET and Multimodal Brain Imaging in Patients at Risk F - 2019 - NeuroImageDocument13 pagesTau PET and Multimodal Brain Imaging in Patients at Risk F - 2019 - NeuroImageBruno MañonNo ratings yet
- Ossenkoppele 2019 PET Tau Pet Amyloid Cortical ThicknessDocument13 pagesOssenkoppele 2019 PET Tau Pet Amyloid Cortical ThicknessAngela SilvaNo ratings yet
- Reduced Cortical Folding in PPPDDocument12 pagesReduced Cortical Folding in PPPDDanielNo ratings yet
- Is Electrocochleography Still Helpful in Early Diagnosis of Meniere Disease?Document5 pagesIs Electrocochleography Still Helpful in Early Diagnosis of Meniere Disease?nandaanggiNo ratings yet
- Journal Pre-Proofs: Radiotherapy and OncologyDocument29 pagesJournal Pre-Proofs: Radiotherapy and OncologyRaul Matute MartinNo ratings yet
- NEJMoa 2307952Document13 pagesNEJMoa 2307952cehborrotoNo ratings yet
- 2020-Incremental Prognostic Value and Underlying Biological Pathways of Radiomics Patterns in MedulloblastomaDocument10 pages2020-Incremental Prognostic Value and Underlying Biological Pathways of Radiomics Patterns in Medulloblastoma原彬科No ratings yet
- Efficacy and Safety of Radiofrequency Ablation Versus Ethanol AblationDocument11 pagesEfficacy and Safety of Radiofrequency Ablation Versus Ethanol AblationIJAR JOURNALNo ratings yet
- Paper TEADocument10 pagesPaper TEAmetteoroNo ratings yet
- Feng C. 2024. Small Needle Knife Vs ESWT Plantar FasciitisDocument11 pagesFeng C. 2024. Small Needle Knife Vs ESWT Plantar FasciitisJavier MartinNo ratings yet
- Association Between Retinal Layer Thickness and Cognitive Decline in Older AdultsDocument8 pagesAssociation Between Retinal Layer Thickness and Cognitive Decline in Older AdultsLuis Daniel Gutierrez GarciaNo ratings yet
- Amico F Et Al (2023) A Resting State EEG Study On Depressed Persons With Suicidal Ideation IBRO Neuroscience ReportsDocument7 pagesAmico F Et Al (2023) A Resting State EEG Study On Depressed Persons With Suicidal Ideation IBRO Neuroscience ReportsAlparslan OnderNo ratings yet
- Association of Plasma Total Tau Level With Cognitive Decline and Risk of Mild Cognitive Impairment or Dementia in The Mayo Clinic Study On AgingDocument8 pagesAssociation of Plasma Total Tau Level With Cognitive Decline and Risk of Mild Cognitive Impairment or Dementia in The Mayo Clinic Study On AgingeastareaNo ratings yet
- Sleep and Psychiatric Abnormalities in Gullian Barré SyndromeDocument7 pagesSleep and Psychiatric Abnormalities in Gullian Barré SyndromeShri RamNo ratings yet
- Long-Term Prognosis After Childhood Convulsive Status Epilepticus: A Prospective Cohort StudyDocument9 pagesLong-Term Prognosis After Childhood Convulsive Status Epilepticus: A Prospective Cohort Studynadia pramitha157No ratings yet
- An H Et Al, Large Intracranial Volume Accelerates Conversion To Dementia, 2016Document10 pagesAn H Et Al, Large Intracranial Volume Accelerates Conversion To Dementia, 2016henryfv2010No ratings yet
- VIP Fang and Shi 2019 Arch Pathol 2019Document11 pagesVIP Fang and Shi 2019 Arch Pathol 2019Jemma ArakelyanNo ratings yet
- Stereoractic Surgery and Brain MetastasisDocument42 pagesStereoractic Surgery and Brain MetastasisCara MagbitangNo ratings yet
- A Real-Time FMRI Neurofeedback System For The Clinical Alleviation of Depression With A Subject-Independent Classification of Brain States A Proof of Principle StudyDocument12 pagesA Real-Time FMRI Neurofeedback System For The Clinical Alleviation of Depression With A Subject-Independent Classification of Brain States A Proof of Principle Studysiowan wongNo ratings yet
- Diagnostic Problems in Tumors of Central Nervous System: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Central Nervous System: Selected TopicsNo ratings yet
- ARTÍCULODocument7 pagesARTÍCULOPablo GuillénNo ratings yet
- Journal or Rheumatology 2021 - Effect of Disease Activity On Organ Damage Progression in SLE, University of Toronto Lupus Clinic CohortDocument7 pagesJournal or Rheumatology 2021 - Effect of Disease Activity On Organ Damage Progression in SLE, University of Toronto Lupus Clinic CohortTengku Reza MaulanaNo ratings yet
- Jurnal Neuropaty dm2Document2 pagesJurnal Neuropaty dm2ferryNo ratings yet
- ijamscrjournal1,+IJAMSCR-21-313+PDFDocument5 pagesijamscrjournal1,+IJAMSCR-21-313+PDFARUL CHOKKANNo ratings yet
- Safety and Efficacy Red Light For Alzheimer'sDocument9 pagesSafety and Efficacy Red Light For Alzheimer'sMonica SaavedraNo ratings yet
- Cortical Thickness Gray White Matter Contrast and Intracortica - 2023 - PsychiDocument9 pagesCortical Thickness Gray White Matter Contrast and Intracortica - 2023 - Psychitito syahjihadNo ratings yet
- Optic Nerve Imaging Solving Demyelination MysteryDocument1 pageOptic Nerve Imaging Solving Demyelination MysteryOncología CdsNo ratings yet
- Clinical Study: Autologous Bone Marrow Mononuclear Cell Therapy For Autism: An Open Label Proof of Concept StudyDocument14 pagesClinical Study: Autologous Bone Marrow Mononuclear Cell Therapy For Autism: An Open Label Proof of Concept StudyMunam MustafaNo ratings yet
- Association of Migraine With Patent Foramen Ovale Closure A Systematic Review and Meta-AnalysisDocument6 pagesAssociation of Migraine With Patent Foramen Ovale Closure A Systematic Review and Meta-AnalysisEndin Nokik StujannaNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and Researchrhegi isdiara FairuzNo ratings yet
- Alabi 2019Document8 pagesAlabi 2019Avijit ChaudhuriNo ratings yet
- Longitudinal neuroimaging biomarkers differ across Alzheimer's disease phenotypesDocument14 pagesLongitudinal neuroimaging biomarkers differ across Alzheimer's disease phenotypesBrenda GonçalvesNo ratings yet
- Franca 2020 AtaxiaDocument6 pagesFranca 2020 AtaxiainervavsNo ratings yet
- MRI of Degenerative Disease of the Spine: A Case-Based AtlasFrom EverandMRI of Degenerative Disease of the Spine: A Case-Based AtlasNo ratings yet
- 2017 Article 141 Part9Document5 pages2017 Article 141 Part9Karina MonasaNo ratings yet
- Gold-Nanobeacons For Gene Therapy: Evaluation of Genotoxicity, Cell Toxicity and Proteome Profiling AnalysisDocument63 pagesGold-Nanobeacons For Gene Therapy: Evaluation of Genotoxicity, Cell Toxicity and Proteome Profiling AnalysisGargi MishraNo ratings yet
- Detection of Cognitive Impairment in Multiple Sclerosis Based On P300 Event-Related PotentialDocument8 pagesDetection of Cognitive Impairment in Multiple Sclerosis Based On P300 Event-Related Potentialzwecker4458No ratings yet
- E2920 FullDocument14 pagesE2920 Fullnatsumi18No ratings yet
- noad045Document20 pagesnoad045albertoNo ratings yet
- Interpersonal Justice and DevianceDocument52 pagesInterpersonal Justice and DevianceMohammad Sohail RashidNo ratings yet
- The Search For A Communication Theory of International Relations GILBOADocument18 pagesThe Search For A Communication Theory of International Relations GILBOARaphaelRicaudNo ratings yet
- Cognitive Behavioral Therapy (CBT) For ChildrenDocument18 pagesCognitive Behavioral Therapy (CBT) For ChildrenIgor100% (1)
- Graphic Rating ScaleDocument12 pagesGraphic Rating ScaledaintycamielNo ratings yet
- Term Paper Curriculum DevelopmentDocument6 pagesTerm Paper Curriculum Developmentafdtsdece100% (1)
- Digital EthnographyDocument11 pagesDigital EthnographySourav DuttaNo ratings yet
- Costa's Levels of Questioning: One - Two - Three Story Intellect PoemDocument5 pagesCosta's Levels of Questioning: One - Two - Three Story Intellect PoemVincent GiuntaNo ratings yet
- Stat HWDocument6 pagesStat HWRalph0% (1)
- Critical evaluation of water coning correlations for vertical wellsDocument9 pagesCritical evaluation of water coning correlations for vertical wellsWilliam Cabrera CastroNo ratings yet
- Transformative LeadershipDocument5 pagesTransformative LeadershipJennifer OestarNo ratings yet
- Bracind of Steel Beams in Bridges PDFDocument96 pagesBracind of Steel Beams in Bridges PDFAndré Luiz NogueiraNo ratings yet
- Evidence Guide For School Excellence: Qualitative DataDocument2 pagesEvidence Guide For School Excellence: Qualitative DataQueresminoctavio RupavaNo ratings yet
- Photography and Cultural Heritage in The Age of Nationalisms Europes Eastern Borderlands (1867-1945) (Ewa Manikowska) (Z-Library)Document269 pagesPhotography and Cultural Heritage in The Age of Nationalisms Europes Eastern Borderlands (1867-1945) (Ewa Manikowska) (Z-Library)thierry100% (2)
- Entrepreneurial Opportunities in AgricultureDocument5 pagesEntrepreneurial Opportunities in AgricultureJan NimerNo ratings yet
- AssignmentDocument4 pagesAssignmentJosh Ross100% (1)
- The Level of Social Media Addiction On The Grade 10 Students in Cirilo Roy Montejo National High SchoolDocument4 pagesThe Level of Social Media Addiction On The Grade 10 Students in Cirilo Roy Montejo National High SchoolRenelsNo ratings yet
- Assignment 1 Dan 2 BJTP 3013Document4 pagesAssignment 1 Dan 2 BJTP 3013Amirul HaziqNo ratings yet
- Performance AssessmentDocument14 pagesPerformance AssessmentRose DesyNo ratings yet
- Cse N14 June2019 PDFDocument131 pagesCse N14 June2019 PDFeeng8124No ratings yet
- Emergency CodesDocument6 pagesEmergency Codesdhshwjdlkjdas;No ratings yet
- Customer satisfaction levels in online shoppingDocument21 pagesCustomer satisfaction levels in online shoppingAlyssa JaneNo ratings yet
- 3a Ej DoE Factorial BreretonDocument4 pages3a Ej DoE Factorial BreretonCecy CepedaNo ratings yet
- ISSN No: 2456: International Open Access Journal International Open Access JournalDocument9 pagesISSN No: 2456: International Open Access Journal International Open Access JournalEditor IJTSRDNo ratings yet
- The Marketing Plan for EntrepreneursDocument48 pagesThe Marketing Plan for EntrepreneursTabaaa YtNo ratings yet
- EAPP Review NotesDocument7 pagesEAPP Review NotesRodjone Binondo100% (1)
- LEREW Thomas E ProQuest Submission No 2Document328 pagesLEREW Thomas E ProQuest Submission No 2elNo ratings yet
- Susi Mulyani 3 Feb 2021Document22 pagesSusi Mulyani 3 Feb 2021Sushi mulyaniNo ratings yet
- Case HARD ROCK CAFEDocument1 pageCase HARD ROCK CAFEGOHAR GHAFFARNo ratings yet
- MPPC 1303 Curriculum Evaluation Individual Assignment Literature ReviewDocument12 pagesMPPC 1303 Curriculum Evaluation Individual Assignment Literature ReviewushaNo ratings yet
- Rapid7 Nexpose ArcSight ESM Solution Brief PDFDocument2 pagesRapid7 Nexpose ArcSight ESM Solution Brief PDFahmad53350% (1)