You might also like
- Tamil Siddhar Jeeva Samadhi PDFDocument23 pagesTamil Siddhar Jeeva Samadhi PDFsenthilkumar100% (1)
- 10 Interview Questions and Answers - DAILY JOBS Dubai UAE - New Job OpeningsDocument27 pages10 Interview Questions and Answers - DAILY JOBS Dubai UAE - New Job OpeningsRaza ButtNo ratings yet
- Kanban COP - Lean Kanban Training PDFDocument14 pagesKanban COP - Lean Kanban Training PDFEdward Schaefer100% (1)
- Lguvisitation-Municipality of CaintaDocument23 pagesLguvisitation-Municipality of CaintaDaniel BulanNo ratings yet
- Altmayer 2019Document50 pagesAltmayer 2019Radiologi RSPDNo ratings yet
- Idiopathic Myositis Ossificans of The Deltoid Muscle A Case Report With Unique Presentation and MRI FindingsDocument4 pagesIdiopathic Myositis Ossificans of The Deltoid Muscle A Case Report With Unique Presentation and MRI FindingsNabil Sangga BuanaNo ratings yet
- Review Article: Radiologic Mimics of Osteomyelitis and Septic Arthritis: A Pictorial EssayDocument18 pagesReview Article: Radiologic Mimics of Osteomyelitis and Septic Arthritis: A Pictorial EssayILham AKbarNo ratings yet
- Lymphoblastic Lymphoma Mimicking Osteomyelitis of Femur in An Immunocompetent Individual. A Case ReportDocument5 pagesLymphoblastic Lymphoma Mimicking Osteomyelitis of Femur in An Immunocompetent Individual. A Case ReportAbdullah ZakiNo ratings yet
- Young Patient With Generalized Lymphangiomatosis: Differentiating The DifferentialDocument6 pagesYoung Patient With Generalized Lymphangiomatosis: Differentiating The DifferentialAngel FloresNo ratings yet
- Synovial Knee Disease: MRI Differential Diagnosis: Poster No.: Congress: Type: AuthorsDocument18 pagesSynovial Knee Disease: MRI Differential Diagnosis: Poster No.: Congress: Type: AuthorsEka JuliantaraNo ratings yet
- Pseudotumor Deltoideus Touch Me Not Lesion of TheDocument5 pagesPseudotumor Deltoideus Touch Me Not Lesion of TheneelimagooglyNo ratings yet
- Cuti Bacterium 2019 Aid2019Document10 pagesCuti Bacterium 2019 Aid2019Vita BūdvytėNo ratings yet
- Collagenous Fibroma (Desmoplastic Fibroblastoma) : Clinical, Pathological and Imaging FindingsDocument41 pagesCollagenous Fibroma (Desmoplastic Fibroblastoma) : Clinical, Pathological and Imaging FindingsAnonymous bE4VegCcNo ratings yet
- Forefoot Myopericytoma: A Case Reportand Review of The LiteratureDocument4 pagesForefoot Myopericytoma: A Case Reportand Review of The LiteratureIJAR JOURNALNo ratings yet
- Hronic Expanding Hematoma of The Left FlankDocument6 pagesHronic Expanding Hematoma of The Left FlankGabriela Serra del CarpioNo ratings yet
- FirbomatnedonDocument7 pagesFirbomatnedonAbiyoga PramanaNo ratings yet
- Case ReportDocument5 pagesCase Reportyudhi kurniawanNo ratings yet
- JournalDocument6 pagesJournalYessi PerlitasariNo ratings yet
- Teno GCT Case ReportDocument6 pagesTeno GCT Case ReportWemdi Priya PrasetyaNo ratings yet
- Radiology - Pathology Conference: Cutaneous Angiosarcoma of The LegDocument6 pagesRadiology - Pathology Conference: Cutaneous Angiosarcoma of The LegFrancisco ZurgaNo ratings yet
- Management of Achilles and Patellar Tendinopathy What We Know, What We Can DoDocument10 pagesManagement of Achilles and Patellar Tendinopathy What We Know, What We Can DoAlberto GallariniNo ratings yet
- Ijerph 19 05837Document9 pagesIjerph 19 05837chan kyoNo ratings yet
- Jurnal 21Document4 pagesJurnal 21Rini Suhartia22No ratings yet
- Merolla 2015Document8 pagesMerolla 2015Sandro RolimNo ratings yet
- Diagnostic Imaging in Neurocysticercosis: Costantino SA, Capiel CA, Rossini SA, Landi M, Bouzas CADocument12 pagesDiagnostic Imaging in Neurocysticercosis: Costantino SA, Capiel CA, Rossini SA, Landi M, Bouzas CAMG LilliNo ratings yet
- General OrthopaedicsDocument50 pagesGeneral Orthopaedicsضبيان فرحانNo ratings yet
- Bone Marrow Edema: Pathogenetic FeaturesDocument6 pagesBone Marrow Edema: Pathogenetic FeaturesRobert Partarrieu StegmeierNo ratings yet
- Synovial Knee Disease: MRI Differential Diagnosis: Poster No.: Congress: Type: AuthorsDocument18 pagesSynovial Knee Disease: MRI Differential Diagnosis: Poster No.: Congress: Type: Authorsjuny138No ratings yet
- RG 244035151Document21 pagesRG 244035151Radio ResidentNo ratings yet
- Intramuscular Cysticercosis 2 CasesDocument3 pagesIntramuscular Cysticercosis 2 CasesDr m amirNo ratings yet
- Muchemwa 2007Document4 pagesMuchemwa 2007prajwal guptaNo ratings yet
- Ecr2010 C-2341 PDFDocument26 pagesEcr2010 C-2341 PDFradiologirsckNo ratings yet
- 03.bab 2Document3 pages03.bab 2abed wicaksonoNo ratings yet
- Surgical Neurology International: Unusual Growth Pattern of A MeningiomaDocument3 pagesSurgical Neurology International: Unusual Growth Pattern of A MeningiomaJamie NicholsNo ratings yet
- 5c. Pathologies of The Musculoskeletal SystemDocument40 pages5c. Pathologies of The Musculoskeletal SystemShehzad QureshiNo ratings yet
- Beyond The Bandeau 4 Variations On Fronto Orbital.58Document20 pagesBeyond The Bandeau 4 Variations On Fronto Orbital.58ahmad humidatNo ratings yet
- LeiomyomaDocument3 pagesLeiomyomacandiddreamsNo ratings yet
- OsteomylitisDocument11 pagesOsteomylitisSri AgustinaNo ratings yet
- High-Resolution Ultrasound in The Assessment of Soft Tissue Tumors and Tumor-Like LesionsDocument41 pagesHigh-Resolution Ultrasound in The Assessment of Soft Tissue Tumors and Tumor-Like LesionsAlvin JulianNo ratings yet
- Giant Cell Tumor of The Tendon Sheath: A Rare Case in The Left Knee of A 15-Year-Old BoyDocument3 pagesGiant Cell Tumor of The Tendon Sheath: A Rare Case in The Left Knee of A 15-Year-Old BoyFriadi NataNo ratings yet
- 2015 Article 367 PDFDocument8 pages2015 Article 367 PDFJesse CusterNo ratings yet
- Myeloma MultipleDocument7 pagesMyeloma MultipleCriissthiiann HernnandezNo ratings yet
- An Interesting Case of Gluteal Swelling - Intramuscular Myxoma (IMM) by DR Zothansanga ZadengDocument3 pagesAn Interesting Case of Gluteal Swelling - Intramuscular Myxoma (IMM) by DR Zothansanga ZadengCJ MazualaNo ratings yet
- 0610case1 Metastatic MelanomaDocument4 pages0610case1 Metastatic MelanomawillygopeNo ratings yet
- Limb Salvage Procedure For Liposarcoma of The Left Thigh: A CaseDocument3 pagesLimb Salvage Procedure For Liposarcoma of The Left Thigh: A CaseL Yudhantoro YudhaNo ratings yet
- IntroductionDocument12 pagesIntroductionKenn yahweexNo ratings yet
- Tuberculosis of The Patella, Report CaseDocument4 pagesTuberculosis of The Patella, Report CaseAnonymous AzXah9n0YNo ratings yet
- Manejo de La Infección EspinalDocument10 pagesManejo de La Infección EspinalWilson Quispe AlanocaNo ratings yet
- Tubercular Osteomyelitis of Calcaneum Bone: A Rare OccurrenceDocument4 pagesTubercular Osteomyelitis of Calcaneum Bone: A Rare OccurrenceMuh Syarifullah ANo ratings yet
- A Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleDocument5 pagesA Rare Case of Large Size Undifferentiated Pleomorphic Sarcoma of AnkleIJAR JOURNALNo ratings yet
- Laporan Pemicu 4 DK 9Document53 pagesLaporan Pemicu 4 DK 9Ade Cahyo IslamiNo ratings yet
- Lab Activity #2 Cellular Adaptations To StressDocument8 pagesLab Activity #2 Cellular Adaptations To StressBernadette RepolNo ratings yet
- Subcutaneous Nodules With A Ground Glass AspectDocument4 pagesSubcutaneous Nodules With A Ground Glass AspectIJAR JOURNALNo ratings yet
- Infection: By: Dr. Abdullah NouhDocument5 pagesInfection: By: Dr. Abdullah NouhMajid Khan100% (1)
- Septic Arthritis UpgradedDocument47 pagesSeptic Arthritis UpgradedVishva Randhara AllesNo ratings yet
- Management of Chronic Osteomyelitis Following Gunshot Injuries: A Systematic Review of LiteratureDocument10 pagesManagement of Chronic Osteomyelitis Following Gunshot Injuries: A Systematic Review of LiteratureDiyah Ayu Nur SantiNo ratings yet
- Skeletal GB Mimant SarcomeDocument7 pagesSkeletal GB Mimant Sarcomeal qurtubi al andalusiNo ratings yet
- Diffuse LipomaDocument4 pagesDiffuse LipomaSASNo ratings yet
- PIIS1201971221000990Document6 pagesPIIS1201971221000990vefijo4087No ratings yet
- Surgical Interventions For Bertolottis Syndrome Case Report and Review of Unsatisfactory Cases in The LiteratureDocument8 pagesSurgical Interventions For Bertolottis Syndrome Case Report and Review of Unsatisfactory Cases in The LiteratureOscar Cayetano Herrera RodríguezNo ratings yet
- Lipohaemarthrosis of The Knee JointDocument13 pagesLipohaemarthrosis of The Knee JointShornai ClaudioNo ratings yet
- Volkmann's Ischemic Contracture by Innocent C. AbuguDocument38 pagesVolkmann's Ischemic Contracture by Innocent C. AbuguChukwuemeka ChidogoNo ratings yet
- Inflammatory Myopathies - An Update For NeurologistsDocument11 pagesInflammatory Myopathies - An Update For Neurologistsrafael rocha novaesNo ratings yet
- Cae Grammar TensesDocument4 pagesCae Grammar TensesYana MarinkovaNo ratings yet
- Extended AbstractDocument4 pagesExtended Abstractadi_6294No ratings yet
- Catalogue2019 PDFDocument12 pagesCatalogue2019 PDFlakavath arthiNo ratings yet
- Kelompok 1 Recount TextDocument11 pagesKelompok 1 Recount TextElvina RahmayaniNo ratings yet
- Current Logk VkbaDocument8 pagesCurrent Logk Vkba21muhammad ilham thabariNo ratings yet
- Arts - 9 - Quarter 3 Module 1Document4 pagesArts - 9 - Quarter 3 Module 1John Mark Prestoza100% (3)
- Timeline of My Exposure To Traditional and New Media - Justine Sheen Gay-12 ABM-BDocument16 pagesTimeline of My Exposure To Traditional and New Media - Justine Sheen Gay-12 ABM-Bapi-389627320No ratings yet
- English NotesDocument39 pagesEnglish NotesNorAini MohamadNo ratings yet
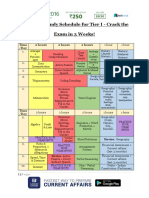
- SSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Document3 pagesSSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Tushita80% (15)
- Pre-Intermediate Tests Audio Script: Track 1Document25 pagesPre-Intermediate Tests Audio Script: Track 1arifsahidNo ratings yet
- Walt Disney BiographyDocument8 pagesWalt Disney BiographyIsaacRodríguezNo ratings yet
- Cherrylene Cabitana: ObjectiveDocument2 pagesCherrylene Cabitana: ObjectiveMark Anthony Nieva RafalloNo ratings yet
- Comptia Linux Xk0 004 Exam Objectives (1 0)Document16 pagesComptia Linux Xk0 004 Exam Objectives (1 0)mueramon100% (1)
- Pengembangan Transferable Skills Dalam PembelajaraDocument12 pagesPengembangan Transferable Skills Dalam PembelajaraKesat RiyanNo ratings yet
- Part 1-2 ProblemsDocument4 pagesPart 1-2 ProblemsDMYKNo ratings yet
- American History 2017-10 PDFDocument76 pagesAmerican History 2017-10 PDFCristian OvanisofNo ratings yet
- Grade 11 Reco ScriptDocument2 pagesGrade 11 Reco ScriptCecill Nicanor LabininayNo ratings yet
- Dwnload Full Using Mis 9th Edition Kroenke Solutions Manual PDFDocument35 pagesDwnload Full Using Mis 9th Edition Kroenke Solutions Manual PDFpasakazinum100% (10)
- Fforde Economic StrategyDocument29 pagesFforde Economic StrategyDinhThuyNo ratings yet
- PE-3-badminton ModuleDocument24 pagesPE-3-badminton ModuleBob Dominic DolunaNo ratings yet
- WWII Europe Organization ChartsDocument56 pagesWWII Europe Organization ChartsCAP History Library100% (1)
- Healthy Boundaries Healthy MinistryDocument5 pagesHealthy Boundaries Healthy MinistryMailey GanNo ratings yet
- 8 Extraordinary Qi VesselsDocument6 pages8 Extraordinary Qi VesselsRiccardo Lautizi100% (1)
- Unit Circle IAKTDocument5 pagesUnit Circle IAKTAnthony KhooNo ratings yet
- 131101-2 Gtu 3rd Sem PaperDocument4 pages131101-2 Gtu 3rd Sem PaperShailesh SankdasariyaNo ratings yet
- Incidence of Alveoloplasty PDFDocument4 pagesIncidence of Alveoloplasty PDFaleeza sanaNo ratings yet