You might also like
- Justice of The Peace Updated Listing As at May 2023Document34 pagesJustice of The Peace Updated Listing As at May 2023sardonyx1No ratings yet
- 17.HSAJB Pathology Services Handbook 4th Edition 2019Document131 pages17.HSAJB Pathology Services Handbook 4th Edition 2019siti nur aishah jalilNo ratings yet
- JKUAT2015 Placements 29 Jun 2016Document219 pagesJKUAT2015 Placements 29 Jun 2016Godfrey Muchai100% (1)
- Astra 200 Users ManualDocument77 pagesAstra 200 Users ManualMaria Isabel Alvarez Sisirucá100% (1)
- Siemens Acuson Sc2000 General Cardiologist Flyer v2Document4 pagesSiemens Acuson Sc2000 General Cardiologist Flyer v2bashir019No ratings yet
- MGMT 3P98 Course Outline S20Document6 pagesMGMT 3P98 Course Outline S20Jeffrey O'LearyNo ratings yet
- MOLO COVID Antigen - Results - 28TH JUNE 2022Document7 pagesMOLO COVID Antigen - Results - 28TH JUNE 2022Samwel GachokaNo ratings yet
- Updated Attachment List2021 IntakeDocument7 pagesUpdated Attachment List2021 IntakeHezekiah AtindaNo ratings yet
- Updated List of Non Eligible Bachelor Students For Fall 2023 ExaminationsDocument16 pagesUpdated List of Non Eligible Bachelor Students For Fall 2023 ExaminationsIllona SigneNo ratings yet
- Justice of The Peace Updated Listing As at February 2020 PDFDocument32 pagesJustice of The Peace Updated Listing As at February 2020 PDFnicksneel67% (3)
- CC Ananum Ing3 23-24 GLDocument3 pagesCC Ananum Ing3 23-24 GLandersfokouNo ratings yet
- Ge 1 Bee Ege 1 1 UtsDocument2 pagesGe 1 Bee Ege 1 1 UtsReyilla Mharie EsteronNo ratings yet
- Hasil Ujian Kasus Kompleks 2022Document1 pageHasil Ujian Kasus Kompleks 2022fitria ningsihNo ratings yet
- Pauta IndustrialDocument5 pagesPauta Industrialsheena.mussa3No ratings yet
- Bank ScheduleDocument18 pagesBank ScheduleChiamaka MaryjoyceNo ratings yet
- 12th - IIT-JEE - PRACTICE TEST (AP-JPT-01) - 15-04-2024Document1 page12th - IIT-JEE - PRACTICE TEST (AP-JPT-01) - 15-04-2024Gowri ShankarNo ratings yet
- Jaguar Community Chapter: Bro. Boogie Quinan Bro. Ruben SenaDocument1 pageJaguar Community Chapter: Bro. Boogie Quinan Bro. Ruben SenaRogelio eduardoNo ratings yet
- Data Bumil Tervaksin Puskesmas TamansariDocument3 pagesData Bumil Tervaksin Puskesmas Tamansariadua_dsdNo ratings yet
- Course Syllabus Acceptance Form CS 1 2Document2 pagesCourse Syllabus Acceptance Form CS 1 2Jerome TacataNo ratings yet
- E Class Record 8 Aguinaldo Science R.CAYANANDocument16 pagesE Class Record 8 Aguinaldo Science R.CAYANANRosita CayananNo ratings yet
- Republic of The Philippines Department of Education Region VII, Central Visayas Division of Cebu Province Cantumog National High School Carmen, CebuDocument7 pagesRepublic of The Philippines Department of Education Region VII, Central Visayas Division of Cebu Province Cantumog National High School Carmen, CebuShysytigre Rejolio SyNo ratings yet
- List & Group VIDocument2 pagesList & Group VImaheshsNo ratings yet
- Covid Laboratory Old, DHH Jharsuguda RT PCR Test Report: Spcimen DetailsDocument12 pagesCovid Laboratory Old, DHH Jharsuguda RT PCR Test Report: Spcimen DetailsPhanindraNo ratings yet
- Input Data Sheet For E-Class Record: Region Division School Name School Id School YearDocument17 pagesInput Data Sheet For E-Class Record: Region Division School Name School Id School YearJohn Paul DioneoNo ratings yet
- Early Registration 2018-2019 As of April 16, 2018Document16 pagesEarly Registration 2018-2019 As of April 16, 2018Benedicto MindajaoNo ratings yet
- BEng CA Report Sheets ENG 1 0 0Document53 pagesBEng CA Report Sheets ENG 1 0 0Gary ReyNo ratings yet
- Internship Placements Yr3Document4 pagesInternship Placements Yr3BUHNYUY RONALDNo ratings yet
- PARK PERMITS GwenDocument1 pagePARK PERMITS GwenCayner WongNo ratings yet
- Highest Possible Score 10 10 10 40 70: Details Essay M5 D-Test Ist Test CT Add'alDocument4 pagesHighest Possible Score 10 10 10 40 70: Details Essay M5 D-Test Ist Test CT Add'alcharyl jean cagaNo ratings yet
- Philosophy of LawDocument1 pagePhilosophy of LawBaptist BataanNo ratings yet
- Data Nik 2Document160 pagesData Nik 2Alvin Nicho Ireng50% (4)
- Attendance Register - CoursewiseDocument2 pagesAttendance Register - CoursewisePalraj KNo ratings yet
- Attendance Register - CoursewiseDocument2 pagesAttendance Register - CoursewisePalraj KNo ratings yet
- Laporan ImunisasiDocument2 pagesLaporan ImunisasiMita anggrainiNo ratings yet
- Daftar Hadir X Guru MapelDocument16 pagesDaftar Hadir X Guru MapelWinda Silviana AeniNo ratings yet
- Rates 2122Document1 pageRates 2122kisko pataNo ratings yet
- Data Promotor Kontrak Puskesmas Di Kabupaten / Kota Bengkulu Tahun 2019Document4 pagesData Promotor Kontrak Puskesmas Di Kabupaten / Kota Bengkulu Tahun 2019WahyuAstri PrastikaNo ratings yet
- Jadwal 2023-2024 Genap PuasaDocument1 pageJadwal 2023-2024 Genap PuasaRizkita SariNo ratings yet
- Bil. Nama Jantina A. Giliran No. K/P SidangDocument3 pagesBil. Nama Jantina A. Giliran No. K/P SidangSharizam Abd TalibNo ratings yet
- New-Report-Card-SHS-v.2.11 - (12 - FIDELITY)Document54 pagesNew-Report-Card-SHS-v.2.11 - (12 - FIDELITY)jannetfrancia.sorretaNo ratings yet
- Data Murid Kelas I S.D Vi Keadaan 12 Agustus 2020Document3 pagesData Murid Kelas I S.D Vi Keadaan 12 Agustus 2020Febri SusantyNo ratings yet
- Prota-Prosem SMAW XII Ganjil 2022-2023Document14 pagesProta-Prosem SMAW XII Ganjil 2022-2023Teguh Pramono TunggalNo ratings yet
- Gazette Vol 89 13 5 22 Special Issue IEBC Independent Candidates PDFDocument428 pagesGazette Vol 89 13 5 22 Special Issue IEBC Independent Candidates PDFKhaledNo ratings yet
- School Form 8 Grade 6Document20 pagesSchool Form 8 Grade 6Mimi Ng PinasNo ratings yet
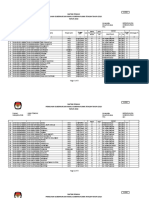
- Daftar Pemilih Pemilihan Gubernur Dan Wakil Gubernur Jawa Tengah Tahun 2018 TAHUN 2018Document77 pagesDaftar Pemilih Pemilihan Gubernur Dan Wakil Gubernur Jawa Tengah Tahun 2018 TAHUN 2018Alvin Nicho Ireng0% (1)
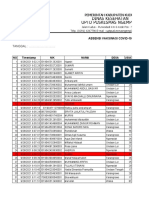
- Daftar Kontak Tracing Covid 19 Bulan Januari 2021Document6 pagesDaftar Kontak Tracing Covid 19 Bulan Januari 2021aminah sendangNo ratings yet
- 01 MarDocument5 pages01 MarFalentinaNo ratings yet
- Visum BadutaDocument6 pagesVisum BadutaFarhan Al FariziNo ratings yet
- Acfrogct8283dxybflcsdmrkzl4v3g3d2uuvflvcljxbpevuax1efvlzev Ufvpef Lwqjxb9a55ebvwmrh2fza Lects1ecvarmdaqj7kj4jt6ps Zzasqv3rplwwxjcjkabmwsd2gyaswudf71Document5 pagesAcfrogct8283dxybflcsdmrkzl4v3g3d2uuvflvcljxbpevuax1efvlzev Ufvpef Lwqjxb9a55ebvwmrh2fza Lects1ecvarmdaqj7kj4jt6ps Zzasqv3rplwwxjcjkabmwsd2gyaswudf71JVC MaliackalNo ratings yet
- Pulo Shs Updates For Graduates Batch 17 18Document8 pagesPulo Shs Updates For Graduates Batch 17 18Cristina MaquintoNo ratings yet
- Gesi3 Ananum 23-24Document3 pagesGesi3 Ananum 23-24presyliamvondoNo ratings yet
- School Form 8 Grade 3Document20 pagesSchool Form 8 Grade 3Mimi Ng PinasNo ratings yet
- MataDocument3 pagesMataJeni Marlin SetiawanNo ratings yet
- IyrmergedDocument4 pagesIyrmergedapi-554428889No ratings yet
- Formulir Pendaftaran Vaksinasi Dosis 1 Sinovac UPTD Puskesmas Ngemplak 28 September 2021 (Jawaban)Document8 pagesFormulir Pendaftaran Vaksinasi Dosis 1 Sinovac UPTD Puskesmas Ngemplak 28 September 2021 (Jawaban)Salam GamersNo ratings yet
- Hong Kong Open 2018 - M - Q Report Version 4 - Updated Tuesday, 23rd October 2018Document16 pagesHong Kong Open 2018 - M - Q Report Version 4 - Updated Tuesday, 23rd October 2018Syafrian Noor HadiNo ratings yet
- Form Pencatatan Vaksin Bri 9 Okt 2021 Di Mcu RSSVDocument211 pagesForm Pencatatan Vaksin Bri 9 Okt 2021 Di Mcu RSSVDeby NoNo ratings yet
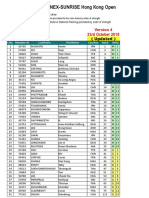
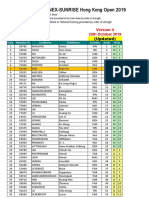
- M & Q REPORT - YONEX-SUNRISE Hong Kong Open 2019: (Updated)Document18 pagesM & Q REPORT - YONEX-SUNRISE Hong Kong Open 2019: (Updated)yoga paripurnaNo ratings yet
- YULIANA PASANG - CVDocument1 pageYULIANA PASANG - CVBudiman HamidNo ratings yet
- New Compliant ListDocument6 pagesNew Compliant Listtq7wtcjprbNo ratings yet
- Deworming ReportDocument8 pagesDeworming ReportCez AkmadNo ratings yet
- G10A GMRCDocument14 pagesG10A GMRCGerbas Julina AredidonNo ratings yet
- REP31OCT2022@1236 3652006433088351034-NewDocument1 pageREP31OCT2022@1236 3652006433088351034-NewSamwel GachokaNo ratings yet
- REP04SEP2023@1329 9185357723681350894-NewDocument1 pageREP04SEP2023@1329 9185357723681350894-NewSamwel GachokaNo ratings yet
- MOLO COVID Antigen - Results - 28TH JUNE 2022Document7 pagesMOLO COVID Antigen - Results - 28TH JUNE 2022Samwel GachokaNo ratings yet
- REP13NOV2022@0038 1618653094445954575-NewDocument1 pageREP13NOV2022@0038 1618653094445954575-NewSamwel GachokaNo ratings yet
- (Day 1 - Part 1) - Phlebotomy-Patient Preparation and ConsiderationDocument5 pages(Day 1 - Part 1) - Phlebotomy-Patient Preparation and ConsiderationAlexia MagtibayNo ratings yet
- NCP Askep BPH PrasDocument9 pagesNCP Askep BPH Prasbaba loxoNo ratings yet
- Team NB PositionPaper BPG TechnicalDocEU MDR 2017 745 V1 20221005Document44 pagesTeam NB PositionPaper BPG TechnicalDocEU MDR 2017 745 V1 20221005eliNo ratings yet
- Reproducibility of Antimicrobial Test Methods: Albert E. Parker, Martin A. Hamilton & Darla M. GoeresDocument9 pagesReproducibility of Antimicrobial Test Methods: Albert E. Parker, Martin A. Hamilton & Darla M. GoeresIkhva RiskianiNo ratings yet
- Belo. Nur 192. Session 11 LecDocument2 pagesBelo. Nur 192. Session 11 LecTam BeloNo ratings yet
- 2000 Ericson Resorption of Incisors AfterDocument9 pages2000 Ericson Resorption of Incisors Afterplayer osamaNo ratings yet
- Firefighter Training, S-130 Fire Exercise Day Instructions To The InstructorDocument22 pagesFirefighter Training, S-130 Fire Exercise Day Instructions To The InstructorVictor Hugo CabralNo ratings yet
- Mapeh 6 Q1 Sy 2022-2023Document11 pagesMapeh 6 Q1 Sy 2022-2023jasonNo ratings yet
- 01 45 00 Quality Control Plan ExampleDocument47 pages01 45 00 Quality Control Plan Examplefranz.scarsNo ratings yet
- Class Vi Jawahar Navodaya Vidyalaya Selection Test - 2021Document2 pagesClass Vi Jawahar Navodaya Vidyalaya Selection Test - 2021AkanshaNo ratings yet
- Second The Friendship ScaleDocument23 pagesSecond The Friendship Scale朱楷文No ratings yet
- WA-705 Water Quality RegulationDocument40 pagesWA-705 Water Quality RegulationvbgiriNo ratings yet
- Img 013Document1 pageImg 013Melchor VasquezNo ratings yet
- RDPL Royal Diagnostics Pvt. Ltd.Document6 pagesRDPL Royal Diagnostics Pvt. Ltd.Royal Diagnostic Centre in Vaishali Nagar JaipurNo ratings yet
- CALIDAD EN EL DISEÑO-QbDDocument24 pagesCALIDAD EN EL DISEÑO-QbDSilvia OrdazNo ratings yet
- Template Assessment EvaluationDocument4 pagesTemplate Assessment EvaluationAlma Tomas-CafeNo ratings yet
- Extending Registration WindowDocument1 pageExtending Registration WindowRaj BahiramkarNo ratings yet
- Psychological Adjustment and Substance UseDocument28 pagesPsychological Adjustment and Substance Usesacit ozkurtNo ratings yet
- GHB H Met GlycohemoglobinDocument37 pagesGHB H Met GlycohemoglobinElizabeth FridayNo ratings yet
- The Clinical NeuropsychologistDocument10 pagesThe Clinical NeuropsychologistroxanaNo ratings yet
- Offshore CableLaid SlingsDocument20 pagesOffshore CableLaid SlingsAdhiPrajakaNo ratings yet
- Inspection and Certification Services For Elevators and EscalatorsDocument4 pagesInspection and Certification Services For Elevators and EscalatorsTek tek hapNo ratings yet
- MT 102 Principles of Medical Laboratory Sciece Practice 2: Clinical Laboratory Asssistance and PhlebotomyDocument2 pagesMT 102 Principles of Medical Laboratory Sciece Practice 2: Clinical Laboratory Asssistance and PhlebotomyAIRAH SALALIMANo ratings yet
- CASP RCT Checklist PDFDocument4 pagesCASP RCT Checklist PDFtengku aniNo ratings yet
- Lp-PLA2 Rapid Quantitative Test COA-F24216102 ADocument1 pageLp-PLA2 Rapid Quantitative Test COA-F24216102 ATerakola VictorNo ratings yet
- Presidential Decree 498Document3 pagesPresidential Decree 498LexaNatalieConcepcionJuntadoNo ratings yet