You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Recommended Doses of IVERMECTINDocument3 pagesRecommended Doses of IVERMECTINRonald LunasNo ratings yet
- What Looks Like Crazy On An Ordinary DayDocument9 pagesWhat Looks Like Crazy On An Ordinary Dayapi-271170207100% (1)
- Fundus PhotoDocument10 pagesFundus PhotoWong Jia YingNo ratings yet
- Aquatic Therapy in RehabilitationDocument28 pagesAquatic Therapy in RehabilitationRadu StoenescuNo ratings yet
- Aetcom 3.5Document4 pagesAetcom 3.5Kondayoor SharadaNo ratings yet
- Urolithiasis SeminarDocument50 pagesUrolithiasis SeminarSiddharth GuptaNo ratings yet
- DRUG STUDY DoxycyclineDocument2 pagesDRUG STUDY DoxycyclineAMIN BARINo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Maladaptive Patterns of BehaviorDocument3 pagesMaladaptive Patterns of BehaviorKimTot Octaviano100% (1)
- Jurnal 882Document1 pageJurnal 882saddamNo ratings yet
- BCCA AB in Febrile Neutropenia GuidelinesDocument2 pagesBCCA AB in Febrile Neutropenia GuidelinesAlvy SyukrieNo ratings yet
- Journal Club 1Document2 pagesJournal Club 1api-549451092No ratings yet
- COVID-19 Antiviral and Pharmacotherapy Information: PreferentialDocument6 pagesCOVID-19 Antiviral and Pharmacotherapy Information: Preferentialmrosyidn0% (1)
- UTI Guideline Example 2 Appendix B PDFDocument4 pagesUTI Guideline Example 2 Appendix B PDFamira catriNo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Document4 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)enquzerNo ratings yet
- COVID-19 InterimGuidelines Treatment ENGDocument25 pagesCOVID-19 InterimGuidelines Treatment ENGMartin PaturlanneNo ratings yet
- Vaksin Hepatitis A, BDocument4 pagesVaksin Hepatitis A, BElvantia MarilynNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument51 pagesSee Full Prescribing Information For Complete Boxed WarningAjay KumarNo ratings yet
- Drug Study: Adult: ChildDocument4 pagesDrug Study: Adult: ChildKristian Karl Bautista Kiw-isNo ratings yet
- Guidance For Treatment of Covid-19 in Adults and Children: Patient PopulationDocument10 pagesGuidance For Treatment of Covid-19 in Adults and Children: Patient PopulationAhmed EljenanNo ratings yet
- Guidance For Treatment of Covid-19 in Adults and Children: Patient PopulationDocument10 pagesGuidance For Treatment of Covid-19 in Adults and Children: Patient PopulationFarmasi RSUD Kramat JatiNo ratings yet
- Covid-19, Sars Cov-2Document8 pagesCovid-19, Sars Cov-2siti lailatul mahmudahNo ratings yet
- COVID-19 ER Clinical Pathway: Registration or Triage NurseDocument2 pagesCOVID-19 ER Clinical Pathway: Registration or Triage NurseBassam AlqadasiNo ratings yet
- Covid-19 Vaccine and CancerDocument12 pagesCovid-19 Vaccine and CancerJelyn DiwaNo ratings yet
- MMC Adult COVID 19 Treatment 3202020Document7 pagesMMC Adult COVID 19 Treatment 3202020Nidal RakanNo ratings yet
- Annex I Summary of Product CharacteristicsDocument35 pagesAnnex I Summary of Product Characteristicsmihaela vlad100% (1)
- Annex I Summary of Product CharacteristicsDocument33 pagesAnnex I Summary of Product CharacteristicsEva DominguezNo ratings yet
- Annex I Summary of Product CharacteristicsDocument33 pagesAnnex I Summary of Product CharacteristicsMohamed AllamNo ratings yet
- UH Treatment Protocol Edit 6 March 24 2020Document9 pagesUH Treatment Protocol Edit 6 March 24 2020zeeNo ratings yet
- 2022 ACR Latest COVID and Rheumatic Disease Therapies - Perritt SawDocument70 pages2022 ACR Latest COVID and Rheumatic Disease Therapies - Perritt SawLiza EgudinsNo ratings yet
- COVID 19 TreatmentDocument8 pagesCOVID 19 TreatmentCWS ScapeNo ratings yet
- 02-2022 CC SupportivePreventiveDocument34 pages02-2022 CC SupportivePreventiveNada AhmedNo ratings yet
- Rituxan Infusion Flow SheetDocument61 pagesRituxan Infusion Flow SheetMartha OktaviaNo ratings yet
- MSHS Treatment Guidelines COVIDDocument4 pagesMSHS Treatment Guidelines COVIDFrancisco MuñozNo ratings yet
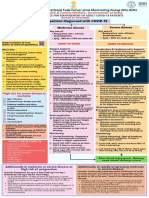
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Annex I Summary of Product CharacteristicsDocument34 pagesAnnex I Summary of Product CharacteristicsLaura RačytėNo ratings yet
- Sjs Fatal KRN AlopurinolDocument6 pagesSjs Fatal KRN AlopurinolMerliana DebyantiNo ratings yet
- DR Deshinta - KIPI Dan Penanganan Syok AnafilaksisDocument45 pagesDR Deshinta - KIPI Dan Penanganan Syok AnafilaksisTRI WIDJAJANo ratings yet
- Management of Acute Asthma inDocument14 pagesManagement of Acute Asthma inDedhy HartantoNo ratings yet
- Drug Study23Document2 pagesDrug Study23Joh Acedo BantingNo ratings yet
- Interim Public Health Testing Utilization Plan (Revision Date: 6/04/20) SUBJECT TO CHANGEDocument6 pagesInterim Public Health Testing Utilization Plan (Revision Date: 6/04/20) SUBJECT TO CHANGEWWMTNo ratings yet
- Levels of Critical Care For Adult Patients (ReviseDocument12 pagesLevels of Critical Care For Adult Patients (Revisejtsk2No ratings yet
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoNo ratings yet
- Early Treatment Information For Doctors Updated 11042022Document4 pagesEarly Treatment Information For Doctors Updated 11042022han tianNo ratings yet
- Management of Infection in Primary Care Adapted For Local UseDocument15 pagesManagement of Infection in Primary Care Adapted For Local UseWizri SuharianiNo ratings yet
- Management of CAP in Adults - Ontario GovernmentDocument2 pagesManagement of CAP in Adults - Ontario GovernmentSukhvir AujlaNo ratings yet
- Micromonospora Purpurea. Action IsDocument3 pagesMicromonospora Purpurea. Action IsCarlos H. AcuñaNo ratings yet
- ULUAVNIV ProtocolDocument10 pagesULUAVNIV ProtocolsatishNo ratings yet
- CCO COVID19 Resources Center Treatment Downloadable 1Document185 pagesCCO COVID19 Resources Center Treatment Downloadable 1YoshimuneNo ratings yet
- Duke Radiology Contrast Media Guidelines Final 10.13.16 PDFDocument35 pagesDuke Radiology Contrast Media Guidelines Final 10.13.16 PDFAdina BatajuNo ratings yet
- ImmunizationDocument20 pagesImmunizationsarguss14100% (2)
- Annex I Summary of Product CharacteristicsDocument34 pagesAnnex I Summary of Product CharacteristicsgladioNo ratings yet
- Guidance For Treatment of Covid-19 in Adults and Children: Patient PopulationDocument10 pagesGuidance For Treatment of Covid-19 in Adults and Children: Patient PopulationIulianNo ratings yet
- Prescriber - 2011 - Meisner - Current Treatments For Lower Respiratory Tract inDocument16 pagesPrescriber - 2011 - Meisner - Current Treatments For Lower Respiratory Tract inamanabduwahabNo ratings yet
- COVID-19 Treatment Guidelines: Clinical ManagementDocument6 pagesCOVID-19 Treatment Guidelines: Clinical ManagementPetra SpringNo ratings yet
- COVID-19 InterimGuidelines Treatment ENGDocument24 pagesCOVID-19 InterimGuidelines Treatment ENGHouda LaatabiNo ratings yet
- Guidance For Treatment of Covid-19 in Adults and Children: Patient PopulationDocument7 pagesGuidance For Treatment of Covid-19 in Adults and Children: Patient PopulationonkarratheeNo ratings yet
- Fact Sheet For Health Workers: Paediatric Formulation of Pfizer-Biontech Covid-19 Vaccine, Bnt162B2Document3 pagesFact Sheet For Health Workers: Paediatric Formulation of Pfizer-Biontech Covid-19 Vaccine, Bnt162B2marie-eve guyNo ratings yet
- Vitamin K (Phytonadione)Document1 pageVitamin K (Phytonadione)E75% (4)
- Azithromycin Medication PDFDocument1 pageAzithromycin Medication PDFmp1757No ratings yet
- Screenshot 2020-03-20 at 08.25.44 PDFDocument10 pagesScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresNo ratings yet
- MGH mass-general-COVID-19-treatment-guidanceDocument21 pagesMGH mass-general-COVID-19-treatment-guidanceAli KhanzadaNo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- Frontiers in Clinical Drug Research - Anti-Cancer Agents: Volume 5From EverandFrontiers in Clinical Drug Research - Anti-Cancer Agents: Volume 5No ratings yet
- Ibtphem Course Flyer and Application 2020Document3 pagesIbtphem Course Flyer and Application 2020Kj_bdNo ratings yet
- Fire Safety Basic Series Flyer TB1Document1 pageFire Safety Basic Series Flyer TB1Kj_bdNo ratings yet
- E1 NLPDocument2 pagesE1 NLPKj_bdNo ratings yet
- 802Document29 pages802Kj_bdNo ratings yet
- Dynamic System Models ShortDocument19 pagesDynamic System Models ShortKj_bdNo ratings yet
- Lecture Note 2: Configuration Space: ECE5463: Introduction To RoboticsDocument19 pagesLecture Note 2: Configuration Space: ECE5463: Introduction To RoboticsKj_bdNo ratings yet
- Positioner Set Up & Calibration: Dyna-Flo Control Valve Services LTDDocument1 pagePositioner Set Up & Calibration: Dyna-Flo Control Valve Services LTDKj_bdNo ratings yet
- Functional Upgrade: SiemensDocument1 pageFunctional Upgrade: SiemensKj_bdNo ratings yet
- Application of Geographical Information System (GIS) Technology in The Control of Buruli Ulcer in GhanaDocument9 pagesApplication of Geographical Information System (GIS) Technology in The Control of Buruli Ulcer in GhanaKj_bdNo ratings yet
- Positioner Set Up & Calibration: Dyna-Flo Control Valve Services LTDDocument1 pagePositioner Set Up & Calibration: Dyna-Flo Control Valve Services LTDKj_bdNo ratings yet
- Siemens Overview For Factory Mounted Ps2'SDocument1 pageSiemens Overview For Factory Mounted Ps2'SKj_bdNo ratings yet
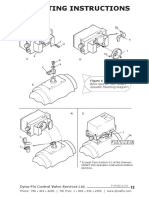
- Mounting Instructions: Basic Quarter Turn Rotary Actuator Mounting DiagramDocument1 pageMounting Instructions: Basic Quarter Turn Rotary Actuator Mounting DiagramKj_bdNo ratings yet
- Siemens PS2: Installation and F.A.Q.'SDocument1 pageSiemens PS2: Installation and F.A.Q.'SKj_bdNo ratings yet
- Mounting Instructions: Basic Quarter Turn Rotary Actuator Mounting DiagramDocument1 pageMounting Instructions: Basic Quarter Turn Rotary Actuator Mounting DiagramKj_bdNo ratings yet
- Siemens Overview For Factory Mounted Ps2'S: Figure 7 Display WindowDocument1 pageSiemens Overview For Factory Mounted Ps2'S: Figure 7 Display WindowKj_bdNo ratings yet
- Siemens PS2: Installation and F.A.Q.'SDocument1 pageSiemens PS2: Installation and F.A.Q.'SKj_bdNo ratings yet
- 9758-Article Text-17770-2-10-20190313Document15 pages9758-Article Text-17770-2-10-20190313Kj_bdNo ratings yet
- Access Fast Fact 2019Document46 pagesAccess Fast Fact 2019see naaNo ratings yet
- Microcarrier Cell Culture ScaleUp Procedures HandbookDocument32 pagesMicrocarrier Cell Culture ScaleUp Procedures HandbookDolphingNo ratings yet
- Bio-Enhancers: A Potential Tool To Improve Soil Fertility and Plant Health in Organic Production of Horticultural CropsDocument19 pagesBio-Enhancers: A Potential Tool To Improve Soil Fertility and Plant Health in Organic Production of Horticultural CropsAzizrahman AbubakarNo ratings yet
- Preparation of Soyabean Milk and ItDocument22 pagesPreparation of Soyabean Milk and Itniki dadhichNo ratings yet
- MS Drug Study 1Document6 pagesMS Drug Study 1Elijah MarfilNo ratings yet
- Tugas Siswa Analytical Exposition 25 SoalDocument7 pagesTugas Siswa Analytical Exposition 25 SoalSid Nade DwNo ratings yet
- Seminar PaperDocument25 pagesSeminar PaperDaguale Melaku Ayele67% (3)
- 1 3 3 Evidence ReportDocument11 pages1 3 3 Evidence Reportapi-296590894No ratings yet
- Microbiology Chapter 4 Laboratory Methods Staining Body FluidsDocument19 pagesMicrobiology Chapter 4 Laboratory Methods Staining Body FluidsAkhilesh TiwariNo ratings yet
- Motivation Day 1Document53 pagesMotivation Day 1sambaNo ratings yet
- Satsuma Brief HistoryDocument3 pagesSatsuma Brief Historyrocky21stNo ratings yet
- Ecotv PDFDocument18 pagesEcotv PDFmacarena castilloNo ratings yet
- Renal Replacement TherapyDocument23 pagesRenal Replacement TherapybgfhnfgNo ratings yet
- Report On Current and Emerging Issues in The Healthcare Sector - Including Home and Community CareDocument148 pagesReport On Current and Emerging Issues in The Healthcare Sector - Including Home and Community CareVica IancuNo ratings yet
- CaplanisDocument12 pagesCaplanisCarlos Zepeda GuidoNo ratings yet
- Meningitis (Deadly Diseases and Epidemics) (PDFDrive)Document121 pagesMeningitis (Deadly Diseases and Epidemics) (PDFDrive)Islamiyatul Hayati MiswanNo ratings yet
- Simple Schematic Diagram of PneumoniaDocument1 pageSimple Schematic Diagram of PneumoniaJason A. AdoyoganNo ratings yet
- 15 Fabrication of NoseDocument12 pages15 Fabrication of NoseNirav RathodNo ratings yet
- Cirrhosis of Liver: Characterized byDocument59 pagesCirrhosis of Liver: Characterized byangath2001No ratings yet
- General Biology 1 Remedial AnsweranDocument2 pagesGeneral Biology 1 Remedial AnsweranJoviNo ratings yet
- Nutrition SPMDocument24 pagesNutrition SPMBaranee NathenNo ratings yet
- MSDS - Shell Mysella - Engine OilDocument7 pagesMSDS - Shell Mysella - Engine OilAnonymous LfeGI2hMNo ratings yet
- 1 Perhitungan Kuda-KudaDocument11 pages1 Perhitungan Kuda-KudaListiyono BudiNo ratings yet
- Pharmacological Activities of Baheda (Terminalia: Bellerica) : A ReviewDocument4 pagesPharmacological Activities of Baheda (Terminalia: Bellerica) : A ReviewDavid BriggsNo ratings yet