You might also like
- 174 Full PDFDocument7 pages174 Full PDFAsyha KantifaNo ratings yet
- Mirtazapine relieves anxiety faster than paroxetine for depression patientsDocument7 pagesMirtazapine relieves anxiety faster than paroxetine for depression patientsSUBHADIPNo ratings yet
- Cognitive Effects of Antipsychotic Drugs in First-Episode Schizophrenia and Schizophreniform Disorder: A Randomized, Open-Label Clinical Trial (EUFEST)Document8 pagesCognitive Effects of Antipsychotic Drugs in First-Episode Schizophrenia and Schizophreniform Disorder: A Randomized, Open-Label Clinical Trial (EUFEST)yeremias setyawanNo ratings yet
- References: Monotherapy Versus Polypharmacy For Hospitalized Psychiatric PatientsDocument1 pageReferences: Monotherapy Versus Polypharmacy For Hospitalized Psychiatric PatientsLeslie CitromeNo ratings yet
- Linehan 1991Document5 pagesLinehan 1991Ekatterina DavilaNo ratings yet
- Tianeptine Combination For Partial or Non-Response To Selective Serotonin Re-Uptake Inhibitor MonotherapyDocument9 pagesTianeptine Combination For Partial or Non-Response To Selective Serotonin Re-Uptake Inhibitor MonotherapyJosuéNo ratings yet
- Comparison of Nefazodone, The Cog Behav Sys of Psychotherapy TX DepressionDocument9 pagesComparison of Nefazodone, The Cog Behav Sys of Psychotherapy TX DepressionCarolina BerríosNo ratings yet
- pcn.12335 (1)Document8 pagespcn.12335 (1)Ariel GaonNo ratings yet
- Original ResearchDocument8 pagesOriginal Researchmarc_2377No ratings yet
- AP JayubDocument4 pagesAP JayubUsama Bin ZubairNo ratings yet
- Efficacy of Antidepressants and Benzodiazepines in Minor Depression Systematic Review and MetaanalysisDocument6 pagesEfficacy of Antidepressants and Benzodiazepines in Minor Depression Systematic Review and MetaanalysisChica MirandaNo ratings yet
- Pharmacotherapy of Irritability in PDDsDocument14 pagesPharmacotherapy of Irritability in PDDsCamila Francisca Cortés ContrerasNo ratings yet
- UntitledDocument9 pagesUntitledNaiana PaulaNo ratings yet
- Pharmacotherapy For Dissociative Disorders - A Systematic ReviewDocument9 pagesPharmacotherapy For Dissociative Disorders - A Systematic ReviewRita Saravia TasaycoNo ratings yet
- Topiramate Augmentation in Patients With Resist 2011 Progress in Neuro PsychDocument4 pagesTopiramate Augmentation in Patients With Resist 2011 Progress in Neuro PsychChris KingNo ratings yet
- DNB Vol22 No4 544Document4 pagesDNB Vol22 No4 544cmarceauNo ratings yet
- Atypical Antipsychotics in Autism TreatmentDocument14 pagesAtypical Antipsychotics in Autism TreatmentEliana RieraNo ratings yet
- Mota Pereira 2018Document6 pagesMota Pereira 2018Dimitris StNo ratings yet
- Clozapine Alone Versus Clozapine and Risperidone With Refractory SchizophreniaDocument11 pagesClozapine Alone Versus Clozapine and Risperidone With Refractory SchizophreniawardahNo ratings yet
- BorderlineDocument22 pagesBorderlineHiba EhtramNo ratings yet
- The Treatment For Adolescents With Depression Study (TADS) : Long-Term Effectiveness and Safety OutcomesDocument14 pagesThe Treatment For Adolescents With Depression Study (TADS) : Long-Term Effectiveness and Safety OutcomesioanaNo ratings yet
- A Placebo-Controlled Trial of Phenelzine, Cognitive Behavioral Group Therapy, and Their Combination For Social Anxiety DisorderDocument10 pagesA Placebo-Controlled Trial of Phenelzine, Cognitive Behavioral Group Therapy, and Their Combination For Social Anxiety DisorderEmaa AmooraNo ratings yet
- Psychosocial Treatments For Bipolar Depression A 1-Year Randomized Trial From The Systematic Treatment Enhanced Program PDFDocument9 pagesPsychosocial Treatments For Bipolar Depression A 1-Year Randomized Trial From The Systematic Treatment Enhanced Program PDFMichael Spike LevinNo ratings yet
- Comparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaDocument6 pagesComparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaLonkesNo ratings yet
- GAD TreatmentDocument15 pagesGAD TreatmentHassan AhmedNo ratings yet
- A Comparison of Risperidone and Haloperidol For The Prevention of Relapse in Patients With SchizophreniaDocument8 pagesA Comparison of Risperidone and Haloperidol For The Prevention of Relapse in Patients With SchizophreniaIlham WahyuNo ratings yet
- Quetiapine or Haloperidol As Monotherapy For Bipolar Mania A 12week Doubleblind Randomised Placebo Controlled Trial - Europ Neuropsych 2005Document13 pagesQuetiapine or Haloperidol As Monotherapy For Bipolar Mania A 12week Doubleblind Randomised Placebo Controlled Trial - Europ Neuropsych 2005Pedro GargoloffNo ratings yet
- ArabeDocument9 pagesArabePablo Maldonado MuñozNo ratings yet
- Should Psychiatrists Use Atypical Antipsychotics To Treat Nonpsychotic Anxiety?Document9 pagesShould Psychiatrists Use Atypical Antipsychotics To Treat Nonpsychotic Anxiety?Andoni Trillo PaezNo ratings yet
- Tratamiento en Patología DualDocument7 pagesTratamiento en Patología DualBalmaNo ratings yet
- Analysis Assignment PsychDocument6 pagesAnalysis Assignment PsychBabs LlamasNo ratings yet
- Garlow 2013Document5 pagesGarlow 2013Doc HadiNo ratings yet
- Olanzapine Shows Superior Efficacy and Safety Profile Compared to Haloperidol in Treating SchizophreniaDocument10 pagesOlanzapine Shows Superior Efficacy and Safety Profile Compared to Haloperidol in Treating SchizophreniaWaoNo ratings yet
- Panss ScoreDocument8 pagesPanss ScoretriaclaresiaNo ratings yet
- Olanzapine Effective BPD AggressionDocument3 pagesOlanzapine Effective BPD Aggressionelvira9No ratings yet
- Yoi 150017Document8 pagesYoi 150017mnn164No ratings yet
- Ajp 156 5 702Document8 pagesAjp 156 5 7029 PsychologyNo ratings yet
- Current Treatments of The Anxiety Disorders in Adults: James C. BallengerDocument16 pagesCurrent Treatments of The Anxiety Disorders in Adults: James C. BallengerElizaIancuNo ratings yet
- ParanoiaDocument1 pageParanoiaFedericoFornariNo ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- Long-term treatments of anxiety disordersDocument16 pagesLong-term treatments of anxiety disordersHassan AhmedNo ratings yet
- Schizophrenia Case StudyDocument3 pagesSchizophrenia Case StudyKumar Suryavanshi100% (1)
- Paper 2Document5 pagesPaper 2fernanda cornejoNo ratings yet
- Boston Medical and Surgical Journal Volume 359 Issue 26 2008 (Doi 10.1056/nejmoa0804633) Walkup, John T. Albano, Anne Marie Piacentini, John Birmaher, - Cognitive Behavioral Therapy, SertralineDocument14 pagesBoston Medical and Surgical Journal Volume 359 Issue 26 2008 (Doi 10.1056/nejmoa0804633) Walkup, John T. Albano, Anne Marie Piacentini, John Birmaher, - Cognitive Behavioral Therapy, SertralineKharisma FatwasariNo ratings yet
- Effects of Risperidone and Olanzapine Dose Reduction On Cognitive Function in Stable Patients With SchizophreniaDocument6 pagesEffects of Risperidone and Olanzapine Dose Reduction On Cognitive Function in Stable Patients With Schizophreniawen zhangNo ratings yet
- Research 3Document12 pagesResearch 3Pratxxm PatelNo ratings yet
- Escitalopram in Post Traumatic Stress DisorderDocument11 pagesEscitalopram in Post Traumatic Stress DisorderVivekNo ratings yet
- Aripiprazole in Schizophrenia and Schizo PDFDocument18 pagesAripiprazole in Schizophrenia and Schizo PDFAlexandra PopaNo ratings yet
- 08 Aj 0844Document11 pages08 Aj 0844kenikirkucing2No ratings yet
- Risperidone Use in Young Children with Autism Spectrum DisordersDocument5 pagesRisperidone Use in Young Children with Autism Spectrum DisordersAdina CipariuNo ratings yet
- Current Evidence For The Management of Schizoaffective DisorderDocument12 pagesCurrent Evidence For The Management of Schizoaffective DisorderabdulNo ratings yet
- Ann Pharmacother 2011 Owenby 95 100Document6 pagesAnn Pharmacother 2011 Owenby 95 100Mahmud AnshoriNo ratings yet
- Antidepressants in Bipolar Depression An Enduring ControversyDocument6 pagesAntidepressants in Bipolar Depression An Enduring ControversyIzzyinOzzieNo ratings yet
- Evidence-Based Treatment For Depersonalisation-Derealisation Disorder (DPRD)Document13 pagesEvidence-Based Treatment For Depersonalisation-Derealisation Disorder (DPRD)Brick SNo ratings yet
- Eficacia de La Amisulprida para Los Síntomas Depresivos en Personas Con Trastornos Mentales Revisión Sistemática y MetanálisisDocument11 pagesEficacia de La Amisulprida para Los Síntomas Depresivos en Personas Con Trastornos Mentales Revisión Sistemática y MetanálisisIVAN ALVAREZNo ratings yet
- Management of Psychiatric Disorders in Children and Adolescents With Atypical AntipsychoticsDocument17 pagesManagement of Psychiatric Disorders in Children and Adolescents With Atypical Antipsychoticsnithiphat.tNo ratings yet
- ZiprasidoneHaloperidolAgitationlPostHocAbstractICOSR CITROME SchizBull2005Document2 pagesZiprasidoneHaloperidolAgitationlPostHocAbstractICOSR CITROME SchizBull2005Leslie CitromeNo ratings yet
- Amisulprid in DepresieDocument11 pagesAmisulprid in DepresieRobert MovileanuNo ratings yet
- Schizophrenia, the Long View Questions You Should Ask Your 34th Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for July 8th, 2022From EverandSchizophrenia, the Long View Questions You Should Ask Your 34th Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for July 8th, 2022No ratings yet
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- InglesDocument6 pagesInglesyarilisNo ratings yet
- Resumen en Ingles Del Diario Ana Frank Chisaguano EmilyDocument16 pagesResumen en Ingles Del Diario Ana Frank Chisaguano EmilyChisaguano EmilyNo ratings yet
- Lecture 9: Exploration and Exploitation: David SilverDocument47 pagesLecture 9: Exploration and Exploitation: David Silver司向辉No ratings yet
- Reflective EssayDocument5 pagesReflective Essaybwood17No ratings yet
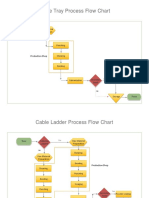
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- Unit 5 Grammar HFDocument7 pagesUnit 5 Grammar HFMilán Benjámin ZámbóNo ratings yet
- Ce6101 Problem Sheet 3Document4 pagesCe6101 Problem Sheet 3HT BinhNo ratings yet
- Mineral Resources: Earth ScienceDocument20 pagesMineral Resources: Earth ScienceRegina Mae Narciso NazarenoNo ratings yet
- PRACH Optimization - V1Document11 pagesPRACH Optimization - V1Tulipe Pivoine100% (5)
- Olympian G60F1 G75F1 Spec SheetDocument6 pagesOlympian G60F1 G75F1 Spec Sheetkman548No ratings yet
- Coastal Wall FinalDocument8 pagesCoastal Wall Finalapi-508287240No ratings yet
- Vibrations and Waves MP205 Assignment 6 SolutionsDocument2 pagesVibrations and Waves MP205 Assignment 6 SolutionsRitesh GhodraoNo ratings yet
- AOC L19W931 22W931 SvcMnlsDocument88 pagesAOC L19W931 22W931 SvcMnlsavrelecNo ratings yet
- Technical Sheet: Choline Chloride 60% VegetalDocument3 pagesTechnical Sheet: Choline Chloride 60% VegetalAnice CharafNo ratings yet
- Headache PAINDocument1 pageHeadache PAINOmarNo ratings yet
- Corn Tastes Better On The Honor System - Robin Wall KimmererDocument53 pagesCorn Tastes Better On The Honor System - Robin Wall Kimmerertristram59100% (1)
- LugeonDocument13 pagesLugeonRojan MaghsoodifarNo ratings yet
- STK6712BMK4: Unipolar Fixed-Current Chopper-Type 4-Phase Stepping Motor DriverDocument11 pagesSTK6712BMK4: Unipolar Fixed-Current Chopper-Type 4-Phase Stepping Motor DriverGerardo WarmerdamNo ratings yet
- Northridge E250pDocument23 pagesNorthridge E250pVion VionNo ratings yet
- Prof (1) F P Kelly - ProbabilityDocument78 pagesProf (1) F P Kelly - ProbabilitycoolmohitNo ratings yet
- Nile and Tigris v2Document554 pagesNile and Tigris v2shuwaarabNo ratings yet
- 3d Printing Thesis StatementDocument5 pages3d Printing Thesis Statementoabfziiig100% (2)
- Experiment 7 & 11: Presented By: Group 4Document55 pagesExperiment 7 & 11: Presented By: Group 4Julliane JuanNo ratings yet
- Reservoir SedimentationDocument20 pagesReservoir SedimentationKathlienNo ratings yet
- Downol PmaDocument2 pagesDownol Pmavanhung68100% (1)
- Bsczo 201Document280 pagesBsczo 201ishfaqqqNo ratings yet
- Industrial Coupling and HoseDocument57 pagesIndustrial Coupling and HoseCesar CoronelNo ratings yet
- Sumalinog Teodoro Jr. LPDocument5 pagesSumalinog Teodoro Jr. LPDAITO CHRISTIAN DHARELNo ratings yet
- Agilent DSO5014A Oscilloscope Tutorial: EE105 Lab ExperimentsDocument6 pagesAgilent DSO5014A Oscilloscope Tutorial: EE105 Lab ExperimentshendraprimaNo ratings yet
- Sir James ChadwickDocument6 pagesSir James ChadwickMichael GuevarraNo ratings yet